In summary, in Swiss Air-Rescue’s physician-staffed HEMS, adjusted on-scene and prehospital time for missions with paediatric patients was slightly longer than in missions with adult patients. Patients in remote areas that are difficult to access due to the terrain, requiring an evacuation involving a helicopter hoist, were associated with the greatest prolongation of on-scene time. Critical interventions, resuscitation and airway management also influenced the on-scene time to a varying degree (Fig. 3). Every single intervention and monitoring measure has a cumulative effect on on-scene time.
An observational study reported median HEMS on-scene times of only 10 min, which may be explained by a high proportion of treatment interventions being conducted by ground-based medical teams before final helicopter transport [20]. A German comparative registry analysis of trauma patients between 2007 and 2009 showed on-scene times of around 40 min for HEMS and explained these in terms of a high proportion of patients requiring airway management [21]. Patient survival for HEMS transport was improved in this German analysis compared to the cohort of ground transportation by ambulance. In our analysis, on-scene time significantly depended on the interventions and measurements performed. It remains unclear whether—and if so to what extent—prolonged on-scene time in general influences patient outcomes [3]. Fixating solely on shortening on-scene times might not capture the reality for patients, as life-saving interventions performed at the prehospital stage substantially reduced mortality in trauma patients [7, 10]. Discovering the correct diagnosis may reduce the delivery time for definitive treatment. For example, stroke patients had improved functional outcomes when treated by a mobile prehospital stroke unit as compared to traditional treatment in hospital [22].
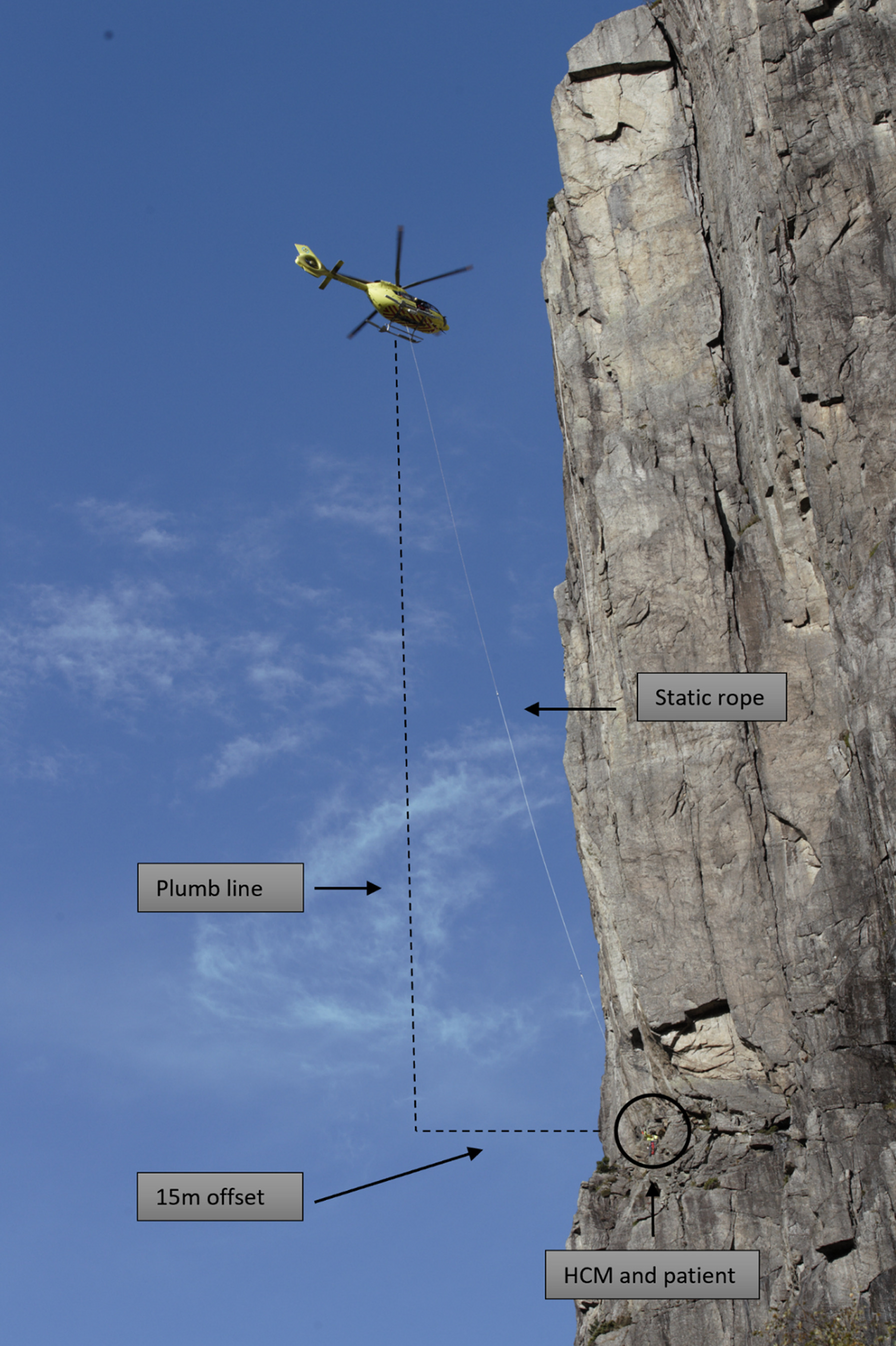
Helicopters enable missions to rescue patients, especially in remote and difficult terrain. Given the topography of Switzerland, with the Alps extending up to 4,634 m and many narrow valleys, these patients might be impossible to reach by ground ambulances. Many missions in this analysis involved patients undertaking recreational activities in the mountains in summer and winter (e.g. skiing, hiking or climbing). Rescue missions with ground-based evacuation teams could, to the patient’s disadvantage, easily require several hours just to reach the patient. A HEMS helicopter operating with a helicopter hoist can bring a physician to the patient directly and in a timely way, resulting in immediate access to clinical investigations and interventions [23]. This could be crucial, as an analysis of helicopter hoist missions in a physician-staffed HEMS reported that nearly 20% of the patients were severely injured and presented with a NACA score ≥ 4 [6]. Such helicopter hoist operations can avoid lengthy terrestrial evacuations, which potentially endanger both patients and rescue crews. Although our data revealed that helicopter hoist operations were associated with the greatest prolongation of on-scene time, the additional on-scene time spent in these HEMS missions results in substantially less rescue time and likely greater chances of neurologically intact survival, as compared to traditional ground rescue.
Advanced airway management in a patient with respiratory failure or the need for a patent airway is a potentially life-saving intervention, which is performed safely by physician-staffed HEMS services, often anaesthesiologists [24]. This skill could even be performed in-cabin as an en-route treatment to optimise time management during the flight to the hospital [25]. Resuscitation was associated with prolonged on-scene time. Performing cardiopulmonary resuscitation in the cabin by HEMS is challenging due to the helicopter’s limited personnel resources and working space. Nonetheless, mechanical chest compression devices facilitate high-quality cardiopulmonary resuscitation in such situations [26]. No evidence, such as outcome data, is yet available for cases after the use of mechanical resuscitation devices under HEMS conditions. Unfortunately, most of these devices cannot be used with paediatric patients, as reflected by the low numbers in our cohort.
Critical interventions were regularly performed and associated with prolonged on-scene time. Most common in this cohort was the administration of intravenous vasopressors to maintain perfusion, intraosseous access and chest needle decompression.
Intravenous access and analgesia were less frequently reported in children than in adults, even though children had more trauma. Our findings are in line with a recent observational study in a physician-staffed HEMS [27]. Even if missions involving children were rare and physicians might not be that thoroughly trained in paediatric rescue, not to mention afraid of the potential risks, the reasons behind this inequity are unclear and require further investigation. Furthermore, the adjusted model revealed a slightly longer on-scene time for paediatric patients, while unadjusted on-scene time was shorter. This might be explained by statistical confounding, as paediatric patients had lower NACA scores compared to adults. However, while this finding was statistically significant, the clinical importance of a prolonged on-scene time of only 1 min might be negligible.
Modifiable variables, such as the duration of a single measure (e.g. a critical intervention), have a significantly larger impact on on-scene time than non-modifiable factors, such as age category, type and number of diagnoses, and NACA score. Thus, reducing the duration of a single measure (intervention or monitoring) in these categories or performing these measures in parallel or during the flight as in-cabin treatment may hold significant potential to reduce on-scene time.
While the measurements in our model were considered statistically independent, several measurements affect each other in clinical practice: A patient with a cardiac arrest is likely to be treated at least with chest compressions, defibrillation, intravenous or intraosseous access, vasopressors, intubation and capnography. Considering the time for all the single measurements, a cardiopulmonary resuscitation might easily last 10–15 min on-scene. For patients requiring emergency anaesthesia, baseline monitoring (SpO2, electrocardiogram, non-invasive blood pressure, and capnography), intravenous or intraosseous access, several medications (e.g. hypnotic, opioid, neuromuscular blocking agent, vasopressors), facemask ventilation, intubation and mechanical ventilation might also result in at least 10–15 min spent on-scene. In our HEMS, one medical crew member is responsible for preparing and administering medication and hemodynamic monitoring, while the other oversees airway management. These parallel performed tasks might save time spent on-scene. However, communication is important in such situations to have shared mental models within the HEMS crew; thus, an airway checklist is performed as standard operating procedure [28].
Our study has several limitations due to its retrospective and observational character. Data in some mission reports (i.e. ICD-10 diagnosis or measurement) are missing. The time of arrival on-scene is the landing time of the helicopter. Thus, the on-scene time might be slightly overestimated. We considered patients with a NACA score ≥ IV potentially time-critical. However, only the patient's most severe NACA score was recorded, which might be resolved by early on-scene treatment (e.g. airway obstruction, tension pneumothorax, anaphylactic shock). Our data may be difficult to compare with those from other topographic areas with less need for helicopter hoist operations. Unfortunately, our database lacks patient-survival and outcome data, which we realised is an important point for improvement on this study. Finally, the study took place over a long period of time which might have had influence in terms of protocols and practice.









留言 (0)