
記住我
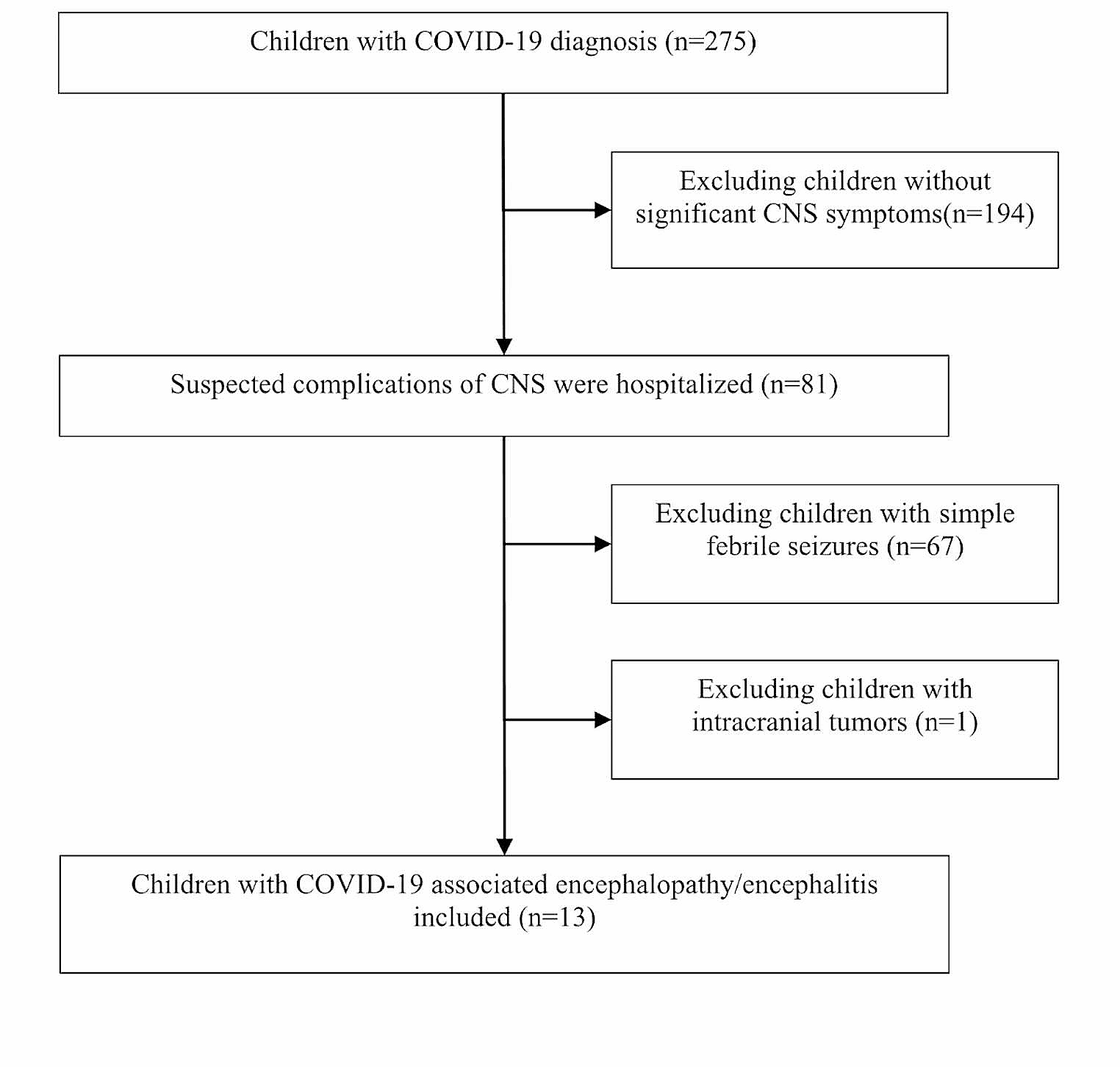

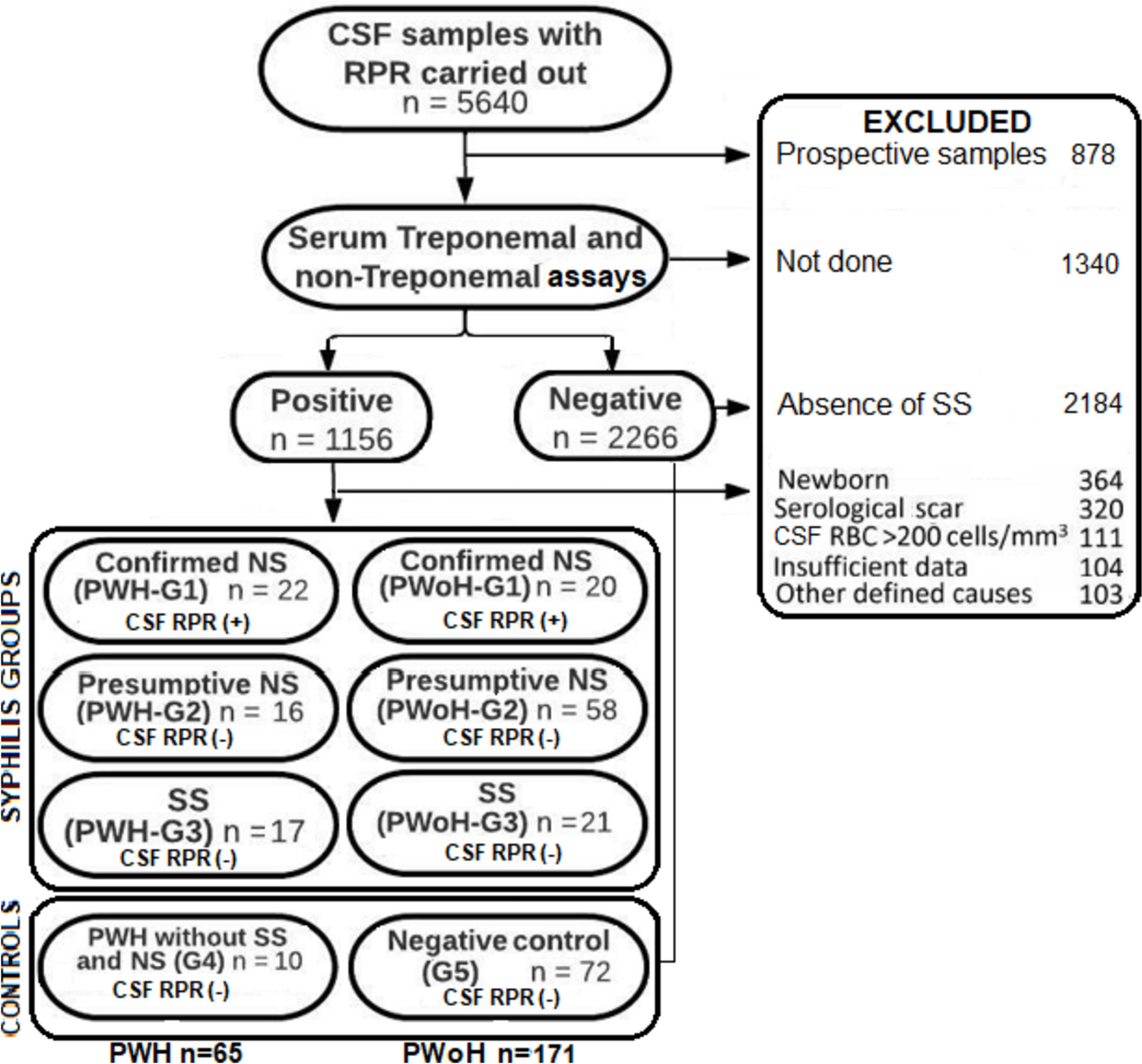
We screened a total of 378 studies, 50 of which were included (see Fig. 1): five prospective trials, one retrospective trial, seven observational studies, and 37 case reports. Two observational studies from unpublished or partially published data were added (Linz/Houston cohort).
Fig. 1
Selection of included reports. Flow chart depicting the selection process of reports included in this review according to PRISMA guideline
Case reportsThe case reports cover a total of 43 patients (20 adults, 23 children; for details see Table S1 (supplementary materials) and Table 1), 33 from single case reports, 10 from case series covering four patients or less.
Table 1 Details case reportsModalities of steroid administration varied widely. The median daily dose (dexamethasone equivalent) was 40 mg (range 8–188 mg; 22 patients). For 16 patients, the daily dose was available relative to body weight (median 2 mg/kg; range 0.1–16.9 mg/kg). For 18 patients, enough information was available to calculate the total steroid dose they received. The median total dose was 180 mg (range 24–940 mg; dexamethasone equivalent). The median start of steroid therapy was seven days after symptom onset (specified for 20 patients; range 1–26) and 3.5 days after hospital admission (specified for eight patients; range 1–7). The median duration of steroid application was four days (28 patients; range 2–25 days). For other minutiae of dosing, duration, and route of administration, see Tables S1 and 1. The authors of only two cases reported by the same group explicitly mention adverse effects (hypernatremia, hyperglycemia, and hypokalemia) [7]. On final evaluation, 12 patients had completely recovered, 22 improved, five were alive without improvement and four had died. Rankin Scale scores were available or could be estimated from the clinical data for 23 patients at discharge and for 24 patients at follow-up (median 240 days; range 30–1095 days; see Table 1).
Studies and case seriesDetails and GRADE ratings of the published trials and case series on the use of steroids in VE are specified in Table 2. Three of the trials (2 prospective, 1 retrospective) report an advantage for steroid therapy.
Table 2 GRADE assessment of the included trials and observational studiesSarkari et al. treated 737 Japanese Encephalitis (JE) patients recruited during epidemics between 1978 and 1989 with a 7-day course of dexamethasone (12 mg/day) and compared the clinical outcome to 462 controls [8]. Only after exclusion of pulmonary edema cases, who were transferred to the steroid group as a life-saving measure, do they report a significantly lower mortality (42.86% and 36.72%, p < 0.01) in the treatment group. No differences concerning adverse events are reported.
Duniewicz et al. found a more rapid normalization of elevated temperatures, headache, nausea, and dizziness in 35 patients with encephalitis caused by diverse viral pathogens treated with intravenous hydrocortisone (5–10 mg/kg/d) than in a control group (29 patients) [9]. The numbers of deceased patients are not explicitly stated; neither is the incidence of adverse event.
Kamei et al. report a more favorable clinical outcome in 22 HSV-1 encephalitis patients treated with dexamethasone or prednisolone at 40–96 mg prednisolone-equivalent per day for a heterogeneous period of time (2–42 days) [10]. The OR for complete recovery is 1.62 (95% confidence interval CI 0.45–5.78). More patients died in the treatment group. However, this odds ratio (OR) did not reach significance. Furthermore, an allocation bias is likely in this non-randomized retrospective trial. No data on adverse events is available.
The other trials report no benefit of steroids in the intervention groups:
Zhang et al. did not see a significant difference in survival between the treatment and control group. The OR for complete recovery is not significant at 0.73 (95% CI 0.15–3.49). The authors describe a significantly higher heart rate, respiratory rate, white blood cell counts, and blood glucose in the patients treated with steroids [11].
Karelitz et al. reported no deaths in their cohort of children with encephalitis [12]. A total of 9 out of 14 treated with steroids and 2 out of 6 non-treated children were asymptomatic at discharge (OR 3.6; 95% CI 0.48–27.11). Adverse effects were not reported.
Rathi et al. describe a trend toward higher mortality in the steroid group [13]. An allocation bias is likely as steroid treatment was not randomized and only applied in those without clinical recovery at three weeks; hence, steroid-treated patients were presumably more affected. The OR for complete recovery was 0.63 (95% CI 0.26–1.51). No data are given for adverse events.
There may be an overlap in the patient cohorts reported by Johnson et al. and Hoke and al, as these were recruited in the same time period in the same hospital [14, 15]. Survival did not differ significantly in the treatment and non-treatment groups. Neither of the two groups describe relevant differences in the occurrence of adverse events.
For the Houston and Linz cohorts (details see Table 3), we found a non-significant tendency toward higher mortality in the treatment group (OR 4.27; 95% CI 0.98–18.69 and OR 6.25; 95% CI 0.22–190.85). As these are retrospective data, we assume that this trend is due to an allocation bias of more severely diseased patients to the treatment group.
Table 3 Details of the Houston and Linz cohortThe outcome of the case series was heterogeneous: full recovery in 10 children with measles encephalitis [16], death or severe sequelae in 4 out of 7 patients with HSV encephalitis in the pre-acyclovir era [17], two fatalities and 19 full recoveries in 21 patients with rubella encephalitis [18], and full recovery in five adults with encephalitis due to diverse pathogens (JE, HSV, and unknown) [19]. All patients received steroid treatment. Sauer described six patients with St. Louis Encephalitis virus, three of which received steroid treatment [20]. One of the non-treated patients died, one of the treated patients recovered fully. The remainder improved with sequelae. Only two groups reported steroid-associated adverse events [17, 19].
Analysis of individual study dataIncluding the Linz and Houston cohorts, we reviewed 15 studies covering 1836 patients. Group data were available for 1555 patients covered in five studies. Individual data were available for 281 persons (* in Table 2). 26 were immunosuppressed (no data for 118 patients). For causative pathogens, see Fig. 2. Data on the CSF cell count were available for 211 patients. The median cell count was 72 cells/µl (range 0–1376 cells/µl). The median GCS score at admission was 12 (n = 129; range 3–15). 82 out of 183 patients received intensive care treatment (missing data n = 98).
Fig. 2
Pathogens in the patient cohort extracted from studies providing individual data
A total of 120 (43%) out of 279 patients received steroids (missing data: n = 2). The substances most commonly used were dexamethasone (n = 69), cortisone (n = 16), and methylprednisolone (n = 15). Route of application was intravenously in 37 patients, intramuscular in 16, and orally in eight patients (missing data: n = 220). 162 patients had one, ten patients two, and 26 patients no further antiviral therapy (missing data: n = 83). The most frequently used antiviral therapy was acyclovir (n = 135), other substances included ACTH, interferons, intravenous immunoglobulins, (val-)ganciclovir, and vidabirine.
The median daily steroid dose (dexamethasone equivalent) was 16 mg (range 3–188 mg; 51 patients) and 0.6 mg/kg (range 0.6–0.8 mg/kg; 27 patients). The median total dose was 44 mg (range 10–1880 mg; 43 patients) and 1.8 mg/kg (range 1.8–4.6 mg/kg; 27 patients). Steroid therapy was started at a median of five days after symptom onset (range 1–1060; 53 patients). The median duration of steroid application was four days (range 1–30 days; 65 patients). Side effects were reported for six patients (hyperglycemia, leukopenia, elevated liver function parameters, polyuria, and thrombopenia; missing data: n = 190).
On final evaluation, 106 patients had completely recovered, 75 improved, eight were alive without improvement and 26 had died. 61 patients survived; however, no further data as to their clinical outcome were available. Outcome data were missing for five patients. The time from onset to final evaluation was available for 72 patients: median 19 days, range 4–116 days.
127 patients had a follow-up with a median of 180 days (last follow-up; range 44 days– > 13 years). 13 additional patients had died in the meantime. 66 patients showed no and 17 patients minor symptoms (modified Rankin Scale (mRS) score 0 or 1), 54 patients had a mRS score between 2 and 5 (missing data n = 131).
For the meta-analysis, data by Hasbun et al., Hoke et al., Johnson et al., Kamei et al., Karelitz et al., Rathi et al., Sarkari et al., Sauer et al., Wagner et al., and Zhang et al. were included [8, 10,11,12,13,14,15, 20]. Visual inspection of the funnel plot suggests presence of a publication bias. However, only few studies have been included into the meta-analysis. With I2 = 30.2%, heterogeneity across studies seems low. For the pooled data, the null hypothesis could not be rejected (p = 0.248) using a random effects model, i.e., a beneficial or harmful effect of steroid treatment on survival in VE could not be shown (for Forest Plot see Fig. 3). The same is true for all individual virus subgroups investigated (HSV, West Nile virus, varicella zoster virus, JEV, Saint Louis encephalitis virus, Epstein–Barr virus, and cytomegalovirus).
Fig. 3
Forest Plot of the odds ratio (OR) for the risk of dying in patients who received steroids (C.P.) vs. those who did not (no C.P.)
留言 (0)