
記住我


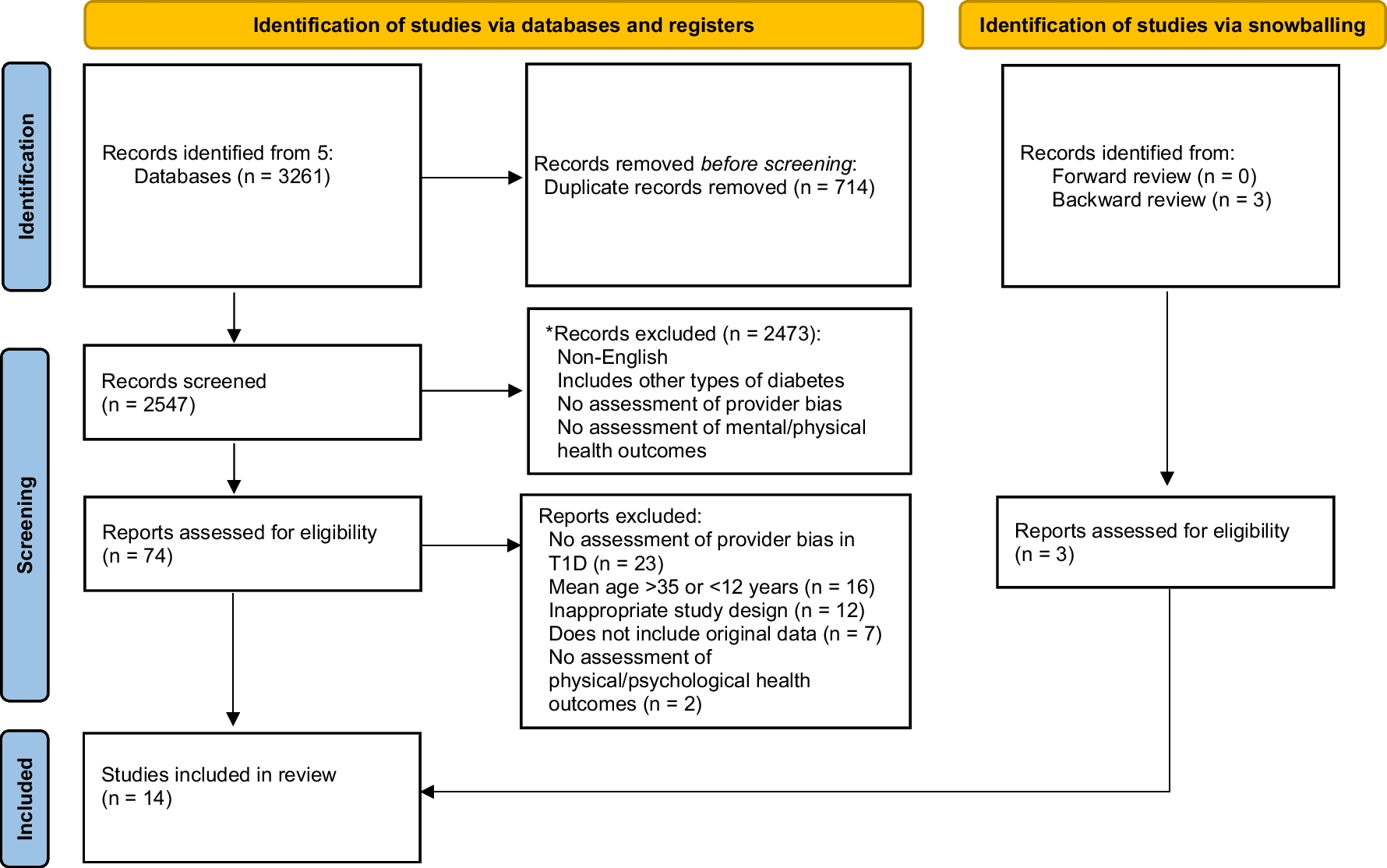

The initial search retrieved 443 manuscripts with 324 titles and abstracts reviewed after duplicates were removed (Fig. 1). Of these, 290 were excluded for not meeting initial inclusion criteria resulting in 34 articles that underwent full text review. Articles were eliminated for the follow reasons: no approaches, strategies, and/or outcomes of CGM implementation or sustainability efforts were reported (n = 12); because the research in fact did not occur in the critical care setting (n = 2); studies were not original research, implementation science, and/or QI designs (n = 2); the study used blinded CGM (n = 1); and because no outcomes were reported (n = 1). Sixteen articles were identified to meet inclusion criteria and were included in the review.
Fig. 1 Characteristics of Included Studies
Characteristics of Included StudiesAll 16 articles included in the review were original research studies. Included studies represented a wide variety of methodological approaches including: randomized controlled trial (n = 4) [14, 15, 16, 17], retrospective cohort studies (n = 7) [4•, 5•, 6•, 8, 10, 18, 19•, 20], prospective cohort studies (n = 3) [9, 21, 22], quasi-experimental (n = 1) [23], and qualitative (n = 1) designs [24]. Eight studies included implementation and clinical data collected during the COVID-19 pandemic [4•, 5•, 6•, 7, 8, 9, 10, 24]. Studies were from 2016 to 2021 and incorporated a total of 1,290 critical care patients. Most studies were conducted in medical intensive care units (MICU) (n = 11) [4•, 5•, 8, 9, 10, 14, 19•, 21, 24, 25], with other studies conducted in mixed intensive care unit (ICU) environments (n = 2) [18, 26], in the pediatric ICU (PICU) [27], and in a cardiac ICU (n = 1) [28]. Half of the studies were conducted in the USA (n = 8) [4•, 5•, 6•, 7, 8, 10, 15, 20, 24], while others were conducted in Europe (n = 5) [14, 17, 21, 22, 29], China (n = 1) [16], Korea (n = 1)[28], and Columbia (n = 1). [9] A number of different types of CGM devices were used (Table 1), with the Dexcom G6 CGM system used most frequently. [4•, 5•, 6•, 7, 8, 10, 20] Several studies featured CGM systems that are not commercially available [14,15,16,17,18, 21, 22, 28].
Table 1 Description of included studiesImplementation Approaches and StrategiesThere was wide heterogeneity in implementation approaches across the included studies (Table 2). The majority of studies (n = 10) reported at least intermittent non-adjunctive CGM use, meaning a confirmatory POC measure was not always required. [4•, 5•, 8, 10, 18, 19•, 24, 25, 26, 28] In 9 studies, the CGM value could be used to titrate insulin. [4•, 5•, 7, 9, 10, 17, 20, 24, 25, 29] Interestingly non-adjunctive use and use for insulin titration were not mutually exclusive. For example, Song 2017 reported that the CGM could be used non-adjunctively but when CGM glucose values met a threshold for insulin adjustment or dosing, then POC glucose was obtained for insulin administration. [28] Not surprisingly, the majority of articles reporting non-adjunctive use and CGM use for insulin dosing were observational studies conducted during the COVID-19 pandemic [4•, 5•, 8, 9, 10, 19•, 20, 24].
Table 2 Continuous glucose monitoring implementationIn studies describing CGM device set up and sensor insertion most indicated members of the research team performed these tasks. [14, 16,17,18, 21, 28] However, during the COVID-19 pandemic, device set-up was performed by members of the endocrinology/diabetes team [4•, 10, 24] while sensor insertion and pairing of the CGM was completed by either the endocrinology/diabetes team [6•, 10, 19•] or by members of the nursing team. [4•, 5•, 8, 9, 20, 24] Several studies described CGM glucose monitoring as performed by nurses, [5•, 20, 24]while in others, the endocrinology team[8] or research team[14] primarily performed monitoring activities. Individuals involved in CGM activities and team composition varied across included studies. Nurses were mentioned most often [5 •, 6 •, 8, 9, 10, 15, 16, 17, 18, 19•, 21, 22, 24] with only 2 studies not mentioning their involvement. [14, 28] Not surprisingly, the pre-COVID era studies all mentioned the role of research staff members, [14, 15, 16, 17, 18, 21, 28] whereas 7 of the 8-pandemic era retrospective studies reported endocrinology/diabetes (DM) team involvement [5•, 6•, 8, 9, 10, 19•, 24].
How glucose was visualized or transmitted was described in 10 studies. [5•, 6•, 8, 10, 16, 18, 19•, 24, 28, 30] Glucose was most often transmitted via Bluetooth to receivers or phones, [5•, 6•, 8, 10, 18, 19•, 20, 24] often kept outside the patient room. [5•, 6•, 8, 10, 19•, 20, 24] Davis et. al., created a glucose telemetry system in which CGM glucose data was transmitted to the Dexcom G6 app on phones kept just outside the person’s room. The Dexcom Follow app was then used to transmit glucose to the nurses’ station where values could be visualized and alarms could be heard in real-time. [5•] Several studies mentioned the use of download visualization software (i.e., Dexcom Clarity, LibreView, CoPilot Health Management System) [5 •, 6•, 9, 18, 24] with a handful specifically mentioning use by the endocrinology/DM teams [5•, 20, 24].
While none of the studies were identified specifically as implementation research, 14 of the 16 identified inpatient implementation strategies that aligned with ERIC definitions (Table 2). Only two studies did not report on any implementation strategies. [14, 28] Across the remaining studies, the frequency of specific implementation strategies used are displayed in Fig. 2. Seventeen different ERIC strategies were described and included in descending order: facilitate relay of clinical data, [4•, 5•, 6•, 8, 9, 10, 16, 17, 19•, 24, 27] educational meetings, [4•, 18, 22, 24] change in physical structure, [6•, 8, 10, 24, 25] distribute materials, [8, 9, 25] identify facilitators and barriers, [21, 24] develop educational materials, [8, 24, 25] assess for readiness,[21, 24] provide clinical supervision, [8,
留言 (0)