
記住我



A DSC study was performed on ITOP and the excipients to elucidate any physicochemical interaction that might affect the activity of drug. As shown in Fig. 1, the drug showed a significant sharp endothermic peak at 192.84 °C, corresponding to its reported melting temperature [11, 43]. No significant changes occurred to the melting peak of ITOP with pectin gum, LAGG, XG, and Avicel 102, while only a slight non-significant shift in the peak of ITOP occurred with PVP k30, and SA gum, which may be attributed to the mixing process, which lowers the concentration of each component in the mixture, thus resulting in slightly broader and lower melting points, but not truly representing any incompatibility [43].
Fig. 1
DSC thermograms of a ITOP, b ITOP:HM pectin gum, c ITOP:LAGG, d ITOP:PVPK30, e ITOP:XG, f ITOP:SA, g ITOP:Avicel 102
Regarding the powder flow properties, all prepared powder mixtures exhibited good to excellent flow properties, with angle of repose values ranging from 21.8o to 28.39°, C.I.% ≤ 18, and H.R.% of < 1.25 except for pectin powders which exhibited only fair flowability, which may be attributed to the irregular shape of pectin particles resulting in low particles rearrangement and hence fair flowability [44, 45].
Post-compression ParametersDetermination of %F, Hardness, Thickness, Diameter, and Weight Variation of TabletsAs shown in Table 1, for the formulations G1-G10 prepared using LAGG, all tablets displayed %F less than 1% except for G1 and G2, which may be attributed to the absence of binder in G1 and its low percent in G2. Concerning formulations P1–P10 prepared using HM pectin, the majority of the formulations displayed %F > 1%, which may be attributed to the high percent of gum in (P1–P5) which consolidates by elastic deformation (temporary deformation) [44], and the inherent poor compactibility of pectin, with lack of plastic deformation in direct compression [46]. P6 formulation lacking PVP k30 gave a loosely bound tablet with high %F, and P7 formulation contained low percentage of binder, which was not sufficient for the formation of coherent tablets. Only formulations P8–P10 containing low percentage of pectin and high percentage of binder were found to be of good appearance and cohesiveness, with %F less than 1%. For SA gum containing formulations (A1–A10), the %F results were > 1% in the formulations containing no PVP k30 (A1, A6), or low amount of PVP k30 (A2), or no Avicel 102 (A10). The absence of binder or diluent resulted in high friability, which may be attributed to the high elastic recovery of alginate matrix associated with capping and lamination [47]. The remaining SA containing formulations showed %F < 1%. Similar to pectin containing tablets, XG containing formulations displayed %F > 1% in the formulations X1–X5, which could be attributed to the higher percentage of XG which exhibits low compactibility and brittle fracture behavior during compression [48], and the absence of PVP k30 in X6 may have hindered the formation of compact tablets [48, 49]. The low %F in formulations X7-X10 could be attributed to the lower percent of XG. The aforementioned results suggest that Avicel 102 and PVP k30 were important in enhancing the compression behavior of tablets and preserving their integrity, hence providing compact tablets with lower friability.
The hardness results of all prepared tablet formulations ranged from 2.56 to 24 Kp despite being compressed at the same force, which is attributed to the different percentage of polymers, binder, and diluent used [32]. All prepared tablets showed uniform thickness and diameter ranging from (3.90–4.26 mm) and (12.05–12.26 mm) respectively, and the weight variation for all the prepared tablets was found to be within the limit of 550 mg ± 5% (data not shown).
Based on the aforementioned data, the formulations with %F exceeding 1% were excluded from further characterization experiments.
In Vitro Drug Release StudiesFigure 2 shows the release profiles of ITOP from the different tablets’ formulations passing the friability test. From the data, it was found that the polymer type was the main factor affecting the drug release from the matrix, which was in the following order: LAGG > HM pectin > SA gum > XG. The fastest release obtained with LAGG tablets (100% release in less than 6 h) concurred with ElZahaby et al. [19] who reported similar release profile of tablets containing 60% w/w LAGG. Moreover, Elmowafy et al. [30] reported that a formulation containing 62.5%w/w of LAGG was completely released within 30 min. This was attributed to the ionization of the polysaccharide in 0.1N HCL which leads to electrostatic repulsion hindering gel formation along with tablet disintegration [50]. It was also reported that the high hydrophilicity of LAGG resulted in instant swelling, high disintegration tendency, and lower gelling ability [51, 52].
Fig. 2
Release profiles of ITOP from different expanding tablets containing a LAGG, b HM pectin, c SA, d XG
All pectin formulations (P8–P10) exhibited early disintegration and could not maintain their physical integrity during the period of the release experiment, which may be attributed to tablet erosion and disintegration that occurs at pH 1.2 with low swelling ability of pectin in this acidic medium owing to the interconversion of carboxylate anion to the carboxyl group, hence converting it into pectinic acid [53,54,55,56].
The SA containing tablets showed sustained release behavior, approaching 100% release after 20 h, with no significant difference in the cumulative percent released of ITOP from the formulations (p > 0.05). The sustained release nature of the SA matrix was reported before in several studies, owing to its swellable nature and formation of a continuous gel layer [19, 57,58,59]. The release of ITOP from XG containing formulations was even more sustained than SA formulations, as shown by the significantly lower (p < 0.05) percent of ITOP release from the former at similar polymer concentration 45%w/w (SA formulations released ≈ 88% at 12 h and XG formulations released ≈ 51% at the same time interval). The drug release from XG matrices is believed to occur by a combination of two mechanisms: diffusion through the swollen matrix and disintegration from the eroded matrix layers [60,61,62,63,64]. Table 2 shows the kinetic data of ITOP release from different tablets matrices. From the data, it was observed that the release data for all tablet formulations except G4 fitted Korsmeyer-Peppas equation; implying diffusion-controlled release, in which the water is expected to diffuse into the tablet’s polymeric matrix, leading to its swelling and consequent diffusion of ITOP through the swollen gel layer [19, 25, 53, 57].
Table 2 The values of the coefficient of determination for the release of ITOP from different tablets matrices by fitting into different equations for release kineticsWorthy to note is that we have loaded 50 mg of ITOP in the tablets, similar to the commercially available tablets. As shown in Fig. 2, we have achieved almost 100% release from the tablets over duration of 24 h during their expected residency in the stomach, which is expected to provide clinically meaningful results. Interestingly, other authors who have formulated ITOP in microballons [11] and effervescent floating tablets [12, 16] have also achieved almost 100% release over a period of 24 h.
Based on the aforementioned results, the formulations prepared using SA (A3-A9) and xanthan gum (X7-X10) were selected for further characterization.
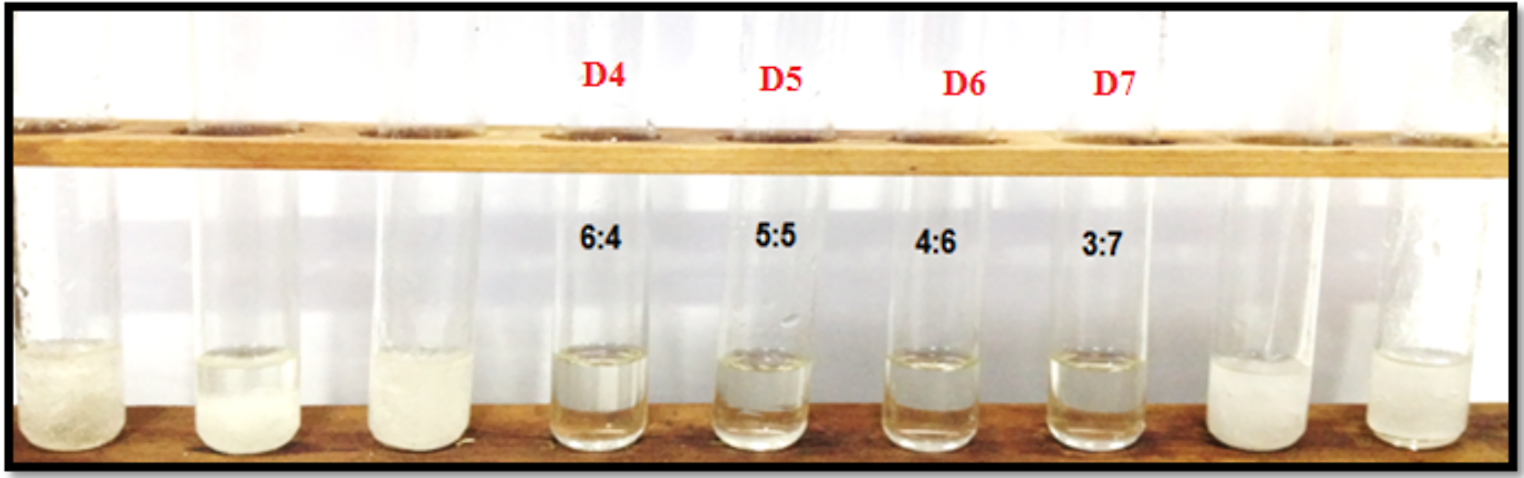
Swelling StudyAs shown in Supplementary 1, 2, and Fig. 3, all formulations containing SA or XG displayed a swelling behavior (presented by % water uptake). SA-containing tablets were hydrated at low pH and formed a gel matrix due to intermolecular binding, which led to an increase in their weight upon contact with the medium [65]. Visual inspection showed that the morphology of the gel around the tablet matrix was neither viscous nor adhesive but tough and rubbery texture which is in agreement with Sriamornsak et al. [57]. The swelling of XG-containing tablets proceeded till 6 h, while in SA-containing tablets, the swelling took place till 3.5 h for tablets A4–A9 and till 4 h for tablet A3, after which they lost their integrity. SA-containing tablets were distorted upon swelling, forming a cracked laminated tablet due to the pressure build up in acidic media and rupture of surface which encouraged tablet erosion [26], as demonstrated in Fig. 3.
Fig. 3
Swelling percentage of ITOP expanding tablets at pH 1.2 for a SA and b XG containing tablets, with representative morphology of tablets showing cracking in the former, and maintenance of integrity in the later
On the other hand, for XG-containing tablets, rapid swelling occurred which was attributed to the formation of a gel layer with no lag time, through hydration of XG particles, preventing the tablet disintegration [66,67,68], coinciding with the results of other authors [62, 66, 69]. The in vitro drug release was inversely correlated with the swelling behavior of the XG-containing formulations, which was also previously reported by other authors [30]. As shown in Fig. 3, XG-containing tablets maintained their shape and integrity. The water uptake study showed that XG formulations exhibited more swelling percentage than SA formulations at similar polymer concentration 45%w/w, as SA formulations reached ≈ 116%w/w at 3.5 h and, on the other hand, XG formulations ≈ 245%w/w at the same time interval. Therefore, the SA-containing tablets were excluded from further characterization.
Based on the previous results, formulation X7 containing XG (45%w/w) in addition to Avicel 102: PVPK30 3:1 was selected for further analysis, since it exhibited sustainment of drug release accounting for 58.53% at 12 h and 94.37% in 24 h and maintained the physical integrity of the matrix throughout the whole 24 h duration, which met our target compared to its counterparts. Using the same procedure and conditions of the swelling test, X7 tablet diameter was measured initially and at 6, 8, 12, and 24 h after immersion in 0.1N HCL, and they were found to increase progressively from 12.01 ± 0.15 mm at 0 h to 16.66 ± 0.33, 17.08 ± 0.46, 17.57 ± 0.54, and 17.45 ± 0.54 mm at 6, 8, 12, and 24 h respectively, while still maintaining their integrity. This was advantageous in our case, since it was reported by other authors that a diameter of about 12–18 mm could achieve gastric retention for several hours by hindrance of the passage through the pyloric sphincter and allowing the retention of the drug formulation inside the stomach [17, 70].
Stability Study and Content UniformityTo indicate the stability of the selected formulation (X7) under accelerated storage conditions, drug assay and in vitro release tests were performed after storage for 3 months at 40 °C/ 75% RH. The assay results before (T0) and after stability were 100.06 ± 2.39 and 98.82 ± 1.17%, respectively, which proved the stability of formulation, shown by the insignificant change in drug content (p > 0.05), and which also complied with USP 42, in which the drug content should be within 90–110% of the label claim.
For the in vitro release test, four selected points in the release profile were selected and compared with the original profile (USP42), as shown in Fig. 4. The difference factor F1 was calculated to be 4.58%, indicating no significant difference between the compared profiles, and the similarity factor F2 was calculated to be 68.28%, indicating high similarity between the two profiles, which further indicates the stability of the formulation.
Fig. 4
Comparative release profiles of formulation X7 before and after accelerated stability storage
In Vivo StudyThe X-ray radiographic technique has been used in many GRDDS studies to determine the gastric residence time of tablets despite its inability to give detailed images of the body, owing to its ability to track the position of tablets with time [42, 71, 72]. The study was carried out on volunteers in fed and fasting state, and from the X-ray radiographic images in Fig. 5, it is demonstrated that the residence time varied from the fasting to the fed state. In the fasting state, the selected tablet formulation X7 was observed in the stomach at 0.5 h and appeared in the small intestine after 1.5 h and then disappeared at 4 h. The rapid emptying of the tablet from the stomach at the fasted state may be attributed to the sweeping wave evacuating the upper GIT through migrating motor complex (MMC) pattern occurring every 1.5–2 h [42, 73]. On the other hand during the fed state, the selected tablet formulation X7 was observed in stomach at 0.5, 1.5, 4, and 6 h, which could be attributed to the slower gastric motility in fed state comparing to fasting state, as the presence of food delayed the evacuation of the stomach hence enhanced the gastric residence of selected formulation [74,75,76]. The X-ray photographs demonstrated that the tablets increased in size after 4 h, and at 6 h, the tablets appeared to be in the expanded form. These results were in agreement with Meka et al. [42] who reported that the tablets appeared in the small intestine after 3 h and disappeared at 6 h in the fasted state, while they remained in the stomach for 6 h in the fed state. This expansion caused by the swelling of the matrix in contact with the gastric fluid is assumed to help in the plugging of the pyloric sphincter and in preventing the tablets’ passage to the small intestine, hence leading to the increased retention time of tablets in the stomach [70]. It is worthy to note that regarding gastric emptying rate, it was proven to depend on the dosage form itself and the state of the stomach (fed or fasted state). The reported gastric emptying time ranges from 2 min to 2 h. The GIT motility involves two modes: the first one is called inter-digestive motility which takes place during the fasting state to evacuate the upper GIT, and the second one is the digestive motility which occurs during the fed state. The GIT motility during the fasting state is controlled by a pattern called migrating motor complex (MMC), which is a pattern of movement and silence controlled by motilin hormone and subdivided into four phases. The presence of food stops the MMC cycle and starts the digestive phase, and the food intake with an oral dosage form is known to increase its gastric retention. However, a factor of paramount importance is the size of the dosage form, in which the gastric residence time is directly proportional to the size of the dosage form. As the size increases the gastric residence time increases, since the relatively large size prevents the dosage form from passing through the pyloric sphincter. However, as observed from the results, despite the swellability of the tablets, the gastric retention was only physiological and not attributed to the swelling of the tablets, as it was not achieved in the fasting state.
Fig. 5
X-ray photographs of gastric expanding tablets X7 in a representative volunteer. a Fasting state (I) 0.5 h (II) 1.5 h (III) 4 h. b Fed state (I) 0.5 h (II) 1.5 h (III) 4 h (IV) 6 h
While the results of this study suggest that expanding tablets could be promising delivery system for itopride, further optimization studies are still needed, especially in terms of establishing tablet compression profile, testing the swelling ability of the selected formulation across a pH range, and to further prepare tablets from xanthan gum of different molecular weights and viscosity values. Moreover, the inclusion of experimental controls in the in vivo study such as administration of tablets prepared without xanthan gum could have highlighted the gastric retention ability of the formulation. Moreover, since the in vivo study was only conducted on two volunteers for the proof of concept, a more extensive clinical study will be attempted in the future, to assess the retention as well as the pharmacokinetic parameters of the selected itopride tablet formulation and its therapeutic efficacy in treatment of gastroesophageal reflux.
留言 (0)