
記住我








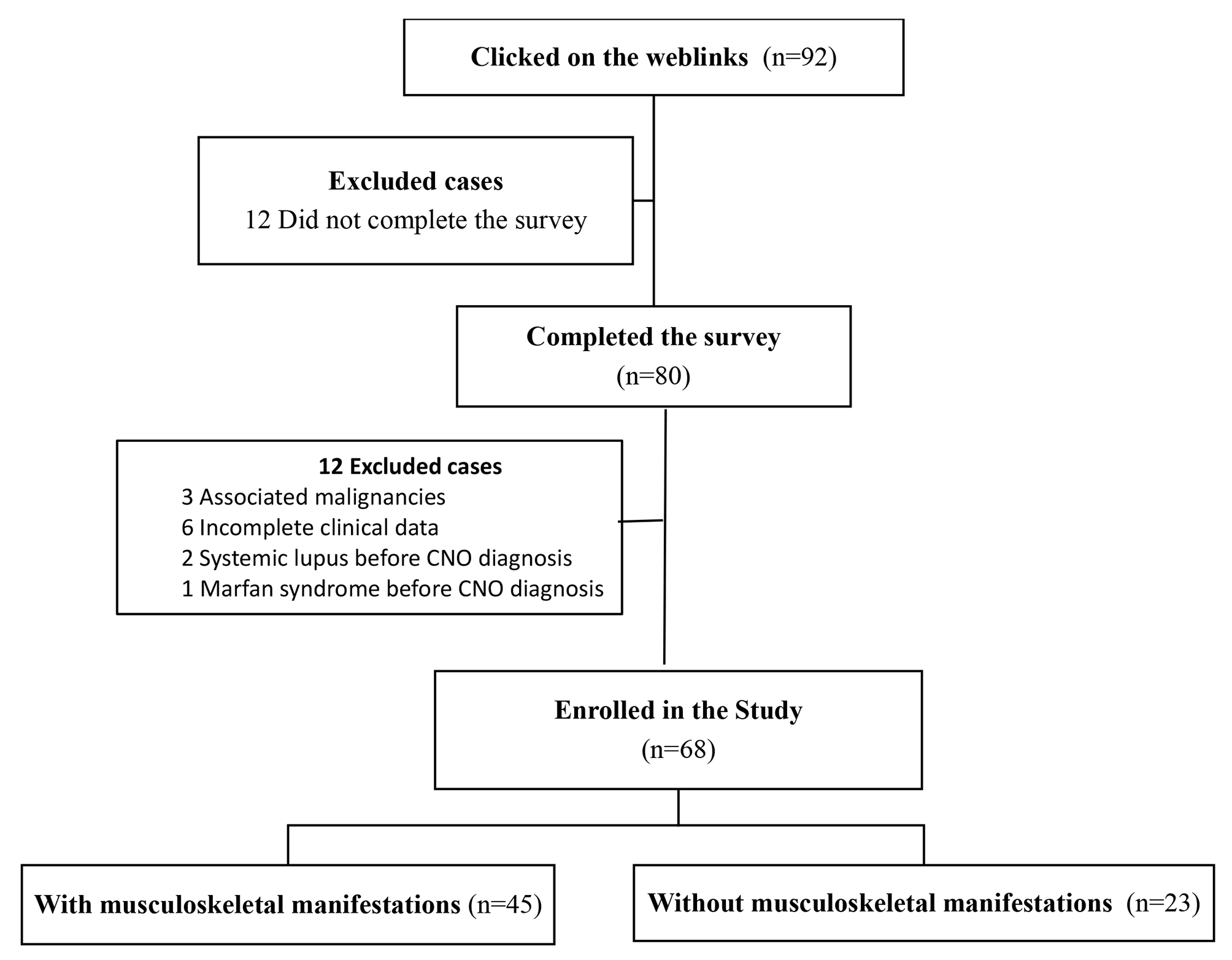
Sixty-two patients were included. Five patients were subsequently excluded based on a revised diagnosis. These diagnoses included KD, systemic-onset juvenile idiopathic arthritis, viral-induced myositis and myocarditis, inflammatory myositis of unknown origin, and bacterial sepsis with multiple epidural abscesses. Fifty-seven MIS-C patients were included in the final analysis (Table 1). The median age was 6 years (range 0–17). The majority of the patients were male (0.72) and this predominance was maintained across the different waves of the COVID-19 pandemic. Forty-seven patients (0.82) had laboratory evidence of previous SARS-CoV-2 exposure. None of the patients died during their hospitalization. Thirty patients (0.53) needed intensive care for advanced cardiovascular and/or respiratory management. Patients warranting PICU admission were older compared to those managed on the general ward (median (IQR) 7 (5–9) years versus 5 (2–8) years respectively, Mann-Whitney U value (U) = 277.5, P = 0.04), whereas there was no difference regarding sex (24 male patients (0.59) versus 6 female patients (0.38) respectively; P = 0.24). Less than 10% of the patients had a chronic comorbidity: three patients (0.05) had well-controlled asthma without maintenance treatment, two patients (0.04) had a history of attention-deficit/hyperactivity disorder. Twenty-two MIS-C patients (0.39) fulfilled the AHA diagnostic criteria for typical KD. All patients had at least one out of five principal clinical features of KD, and a vast majority (0.91) had three or more features. The most prominent KD feature in our population was bilateral conjunctivitis, occurring in 53 patients (0.93), whereas the least frequent feature was cervical lymphadenopathy (0.16). Nearly all MIS-C patients (0.97) had gastrointestinal manifestations. Fifty patients (0.88) presented with signs of circulatory shock and/or hypotension. Cardiac involvement was frequently observed with high median peak values of serum NT-proBNP (7010 ng/l) and troponin (32.0 ng/l), and approximately one third of the patients having left ventricular dysfunction on echocardiogram. Hyperinflammation was a cardinal feature of our MIS-C population with high median peak CRP (188.3 mg/l) and ferritin (482 µg/l) levels. Moreover, hypoalbuminemia (0.86), hyponatremia (0.63), and thrombocytopenia (0.51) were key laboratory findings. All patients received initial treatment with IVIG. Forty-four patients (0.77) were treated with corticosteroids, of which 40 patients (0.91) initially received intravenous pulse steroids. Eight patients (0.14) received a biologic agent, in addition to IVIG: five patients were treated with IL-1 inhibition (anakinra), two with IL-6 inhibition (tocilizumab) (of which one patient also received anakinra), and two with TNFα-inhibition (infliximab). Both patients treated with infliximab presented in the first wave, when it was unclear how to manage MIS-C. Those patients were therefore treated per KD guidelines.
Table 1 Demographic and clinical features of MIS-C patients across the COVID-19 waves Comparative analysis of MIS-C phenotypes during the COVID-19 pandemicMost differences in MIS-C clinical and laboratory features were found when comparing patients presenting during the second versus the fourth wave, and the first versus the fourth wave (Table 2). The smallest differences were observed between patients presenting during the third and the fourth wave. Only one MIS-C patient in the fourth wave fulfilled the criteria for typical KD. Moreover, three out of four patients with only one principal KD feature presented during the fourth wave. Fisher’s exact and Kruskal-Wallis tests did not observe any significant differences regarding the other MIS-features in Table 1. High ferritin and NT-proBNP values and low albumin values and platelet counts were mainly observed in MIS-C patients presenting during the third and fourth wave (Fig. 1).
Fig. 1
MIS-C patients presented with distinct laboratory features across the COVID-19 pandemic. Violin plots depicting differences in key laboratory MIS-C features in patients presenting during the four waves (panel A) and both phases (phase one is wave one and two combined, phase two is wave three and four combined; panel B) of the COVID-19 pandemic: peak ferritin values, platelet counts nadir, albumin nadir values, and peak NT-proBNP values
The above results led us to hypothesize that MIS-C patients presenting during the third and fourth wave had a distinct clinical and biochemical phenotype compared to those encountered during the prior waves. Splitting the COVID-19 pandemic into two phases (wave one and two combined versus wave three and four combined) resulted in significant differences in phenotype (Table 2; Fig. 1). Patients presenting during the second phase presented with higher ferritin, D-dimer, and NT-proBNP values, more liver enzyme abnormalities, more frequent and more severe hypoalbuminemia, and more frequent and more severe thrombocytopenia. Patients from the second phase fulfilled less frequently the KD criteria compared to the first phase (0.24 versus 0.50), but the difference lacked statistical significance (P = 0.06).
Table 2 Upper panel: MIS-C features differed between the respective COVID-19 waves. Lower panel: Distinct MIS-C features in patients presenting during the first phase of the COVID-19 pandemic (first and second wave combined) compared to those presenting during the second phase (third and fourth wave combined)The unsupervised clustering model (Kohonen’s Self-Organizing Map [15]) using age, clinical, laboratory, and imaging features as input features, without information on the respective COVID-19 wave, classified almost half of the patients (0.47) in the correct wave (eTable 1). Cluster 1 mainly consisted of patients from the third wave (5/8). This cluster was characterized by the presence of hypotension/shock, high CRP, ferritin, D-dimer and NT-proBNP levels, liver enzyme abnormalities, hypoalbuminemia, thrombocytopenia, and ventricular dysfunction. Cluster 2 comprised patients from the second (3/7), third (2/7), and fourth wave (2/7). Striking features in this cluster were younger age, coagulation dysfunction, shock/hypotension, hyponatremia, and hypoalbuminemia. Cluster 3 mainly consisted of patients from the second wave (14/22) and was characterized by the highest prevalence of KD features. Finally, cluster 4 mainly comprised patients from the second (8/20) and first (6/20) wave. This cluster was characterized by a less severe MIS-C phenotype with a lower prevalence of hypotension/shock, lower CRP, ferritin, NT-proBNP, and D-dimer levels, less hyponatremia and thrombocytopenia, no ventricular dysfunction, and few chest X-ray abnormalities compared to the other clusters. The same self-organizing map was used to categorize patients in two clusters. This model classified three quarters of the patients (0.74) in the correct phase of the pandemic (wave 1 + 2 versus wave 3 + 4) (eTable 1). Cluster 1 mainly consisted of patients from the second phase (19/28). Compared to cluster 1, striking features of cluster 2 were shock/hypotension, very high ferritin, D-dimer, and NT-proBNP levels, (severe) hypoalbuminemia, thrombocytopenia, liver enzyme abnormalities, ventricular dysfunction, and chest X-ray abnormalities.
MIS-C features associated with severe disease requiring intensive care or treatment with biologic agentsUnivariate analyses revealed that intensive care need was significantly associated with the presence of circulatory shock/hypotension, laboratory evidence of (prior) SARS-CoV-2 infection, higher CRP, ferritin, D-dimer, NT-proBNP and troponin levels, lower albumin levels, ventricular dysfunction, and chest X-ray abnormalities (Table 3). Multivariate logistic regression models assessed the associations of several variables with the need for pediatric intensive care. A model encompassing NT-proBNP, CRP, and ferritin as covariates explained 70% (Nagelkerke R [2]) of the variance and correctly classified 88% of the cases. The model exploring peak NT-proBNP levels, peak ferritin levels, and circulatory shock/hypotension explained 72% of the variance in intensive care and correctly classified 88% of the cases. Finally, the model exploring peak NT-proBNP levels, peak ferritin levels, and chest X-ray abnormalities explained 89% of the variance in intensive care and correctly classified 94% of the cases. Peak NT-proBNP was the only variable significantly associated with intensive care in all multivariate models. Several logistic regression models using different combinations of the variables depicted in Table 3 were less associated with the need for intensive care compared to the models described above (data not shown). Because peak NT-proBNP levels may occur after PICU admission, we also evaluated peak levels occurring before or at time of PICU admission. Patients warranting intensive care had significantly higher NT-proBNP levels at PICU admission compared to patients managed on the general ward (median (IQR) 2107 (582–4557) ng/l versus 6022 (3367–14,852) ng/l, U = 91.0, P = 0.014). The optimal NT-proBNP cut off for PICU admission was 2406 ng/l (area under the curve 0.74, 95% CI 0.56–0.91, sensitivity 87%, specificity 52%). We explored the association of peak NT-proBNP levels with other MIS-C features (Table 4; Fig. 2). Higher peak NT-proBNP levels were associated with the presence of clinical features of shock and/or hypotension, liver enzyme abnormalities, hyponatremia, thrombocytopenia, ventricular dysfunction, aberrant findings on chest X-ray, and non-invasive and/or mechanical ventilation. Moreover, there was a poor correlation between NT-proBNP and peak CRP, peak ferritin, peak D-dimer, sodium nadir and platelets count nadir, while a moderate to good correlation was found between NT-proBNP and peak troponin and albumin nadir, respectively. Treatment with biologic agents was significantly associated with peak CRP and ferritin levels (Table 3).
Table 3 Distinct features of MIS-C patients warranting PICU admission or treatment with biologic agents Table 4 Association of higher peak NT-proBNP levels with MIS-C clinical features reflecting severe disease and correlation with other MIS-C laboratory indices Fig. 2
N-terminal B-type natriuretic peptide (NT-proBNP) correlated significantly with several other MIS-C features reflecting severe disease. Upper panel shows scatter plots combined with logistic regression depicting the correlation between NT-proBNP levels and sodium nadir levels, platelet counts nadir, peak ferritin levels, and albumin nadir levels, respectively. Lower panel depicts violin plots quantifying NT-proBNP levels in MIS-C patients with and without liver enzyme abnormalities, hyponatremia, thrombocytopenia, and ventricular dysfunction on echocardiogram, respectively
留言 (0)