
記住我









This two-blind randomized comparison of medial-term clinical outcomes and benefits between US-guided repeated TPVB using TSA approach and POS approach for the treatment of thoracic HZ was conducted in our department of anesthesiology and pain in the First People’s Hospital of Chongqing Liang Jiang New Area from June 2021 to June 2022 (Fig. 1), and registered in the Chinese Clinical Trial Registry (ChiCTR2200065783). The study was performed in accordance with the Helsinki Declaration of 1964 and its later amendments. The Institutional Review Board approved the data collection and analysis (LJXQDYRMH:202114X). Written informed consent from patients was achieved before recruitment.
Fig. 1
The CONSORT diagram of patient recruitment
Inclusion criteria were (1) diagnosed as HZ in the thoracic dermatomal; (2) presented to our pain clinic within 2 weeks from the initial onset of HZ rash; (3) 50 years or older; (4) HZ-associated pain defined as a score of > 3 in the ‘worst pain’ question of the Zoster Brief Pain Inventory (ZBPI); (5) complete medical record data; (6) follow-up according to our routine protocol. Patients were excluded if they had immunity dysfunction, hepatic or renal dysfunction, coagulation disorders, systemic use of antivirals, and pregnancy/lactation.
Randomization and BlindingA total of 136 eligible patients were recruited for the study, and randomly assigned into one of the following two groups at a ratio of 1:1 (Fig. 1). Groups were the TSA group (control group): patients received the standard 7-day course antiviral treatment (famciclovir 500 mg three times daily) immediately after recruitment, and US-guided repeated TPVB by TAS approach following the antiviral therapy. POS group: patients received the same standard antiviral therapy as the control group immediately after recruitment, in addition, repeated TPVB under US guidance using POS approach was administered sequentially after completion of the antiviral therapy. Etoricoxib (60-mg tablets, once daily, Hangzhou Merck Sharp & Dohme Pharmaceutical Co. LTD, China) and oxycodone-acetaminophen (5 mg/325 mg tablets, up to four times daily, a drug named Depalgos©; Molteni Farmaceutici, Inc., Italy) were respectively available as rescue analgesics on the basis of pain severity following the established guidelines of the World Health Organization (WHO). Supplemented pain medicine such as antidepressant drugs and antiepileptic drugs was not allowed during the whole follow-up period.
The allocation sequence was produced using Stata Version 14 (StataCorp LP, College Station, TX, USA) in permuted blocks of size six according to admission order in our pain center. It would be concealed on a secure website by staff who was not involved in the study until delivered to pain physician who performed the block procedures. Patients and investigators responsible for outcomes assessment were blinding to the group allocation.
Procedure of Ultrasound-Guided Thoracic Paravertebral Block Using Two Different ApproachesAll procedures were performed in the outpatient operating room under US guidance by the same skilled pain physician who was an expert in performing regional nerve block. Electrocardiography, blood pressure, and oxygen saturation monitoring were applied. Patients were in the lateral position with the affected side upward.
For patients who received US-guided TPVB using TSA approach, a low-frequency convex array probe was applied transversely to the targeted lateral aspect of the thoracic spinous process. In the short-axis view of the thoracic paravertebral area, paravertebral muscles and the hyper-echoic transverse process were identified clearly. The black acoustic shadow in front of the transverse process completely obscured the thoracic paravertebral area. The hyper-echoic area among parietal pleura, superior costotransverse ligament (SCL), and internal intercostal membrane which represents the top of thoracic paravertebral space (TPVS) or the medial boundary of posterior intercostal space was correspondingly identified by slightly moving the transducer cranially or caudally. Subsequently, color Doppler mode was used to identify whether a vulnerable blood vessel was abnormally situated around the targeted TPVB area in order to avoid intravascular injection. A 22-gague needle was introduced under real-time US guided from lateral to medial with an in-plane technique to target the hyper-echoic TPVS top or the posterior intercostal space. After confirmation of the needle tip, 0.2–0.3 ml (ml) of 1% lidocaine was injected for testing, and patients were monitored for clinical signs such as dizziness, slurred speech, blurred vision, tinnitus, obnubilation, bradycardia, blood pressure crashes, paresthesia, muscle tremors, convulsions, and anesthesia in the affected thoracic dermatomal/HZ-associated pain alleviation for 10 min. After verification, 2 ml of block injectate (2% lidocaine 20 mg/ml + triamcinolone 5 mg/ml + normal saline) was injected under real-time US guidance for each affected thoracic nerve root every 48 h for a week. Meanwhile, the hyper-echoic pleura was moved forward, and the top of the TPVS was expanded due to the spread of the injectable suspension in the real-time ultrasonic image (Fig. 2a) [12].
Fig. 2
Paravertebral space puncture under ultrasound guidance using TSA and POS approaches
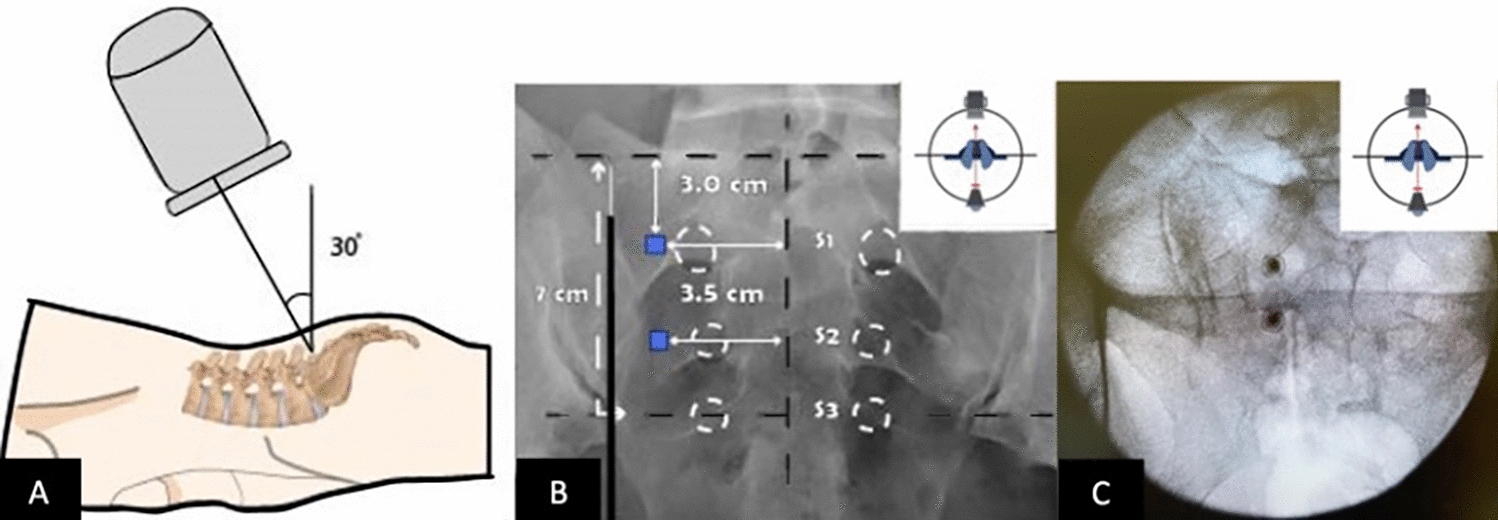
For patients who received TPVB using the POS approach, a high-resolution linear transducer was sagittally placed 2–3 cm away from the thoracic paramedian line with the probe mark toward the cephalad direction. In the sagittal-axis view, paravertebral muscles and the hyper-echoic transverse process were identified clearly. Between the two adjacent black acoustic shadows of the transverse process, the acoustic window was composed of costotransverse ligament, SCL, TPVS, and parietal pleura were clearly identified. The TPVS could be more clearly identified by slightly moving the transducer laterally. After Doppler scan, a 22-gague needle was introduced under real-time US guidance from caudal to cranial with an in-plane technique to target the TPVS. The same test dose of lidocaine was injected to monitor for the clinical signs as above. Then the same drug mixture was injected under real-time US guidance for each affected thoracic nerve root every 48 h for a week. Also, the TPVS was successfully monitored to be expanded with the hyper-echoic pleura moving forward due to the spread of the injectable suspension (Fig. 2b).
Outcome MeasuresVisual analogue scales (VAS) (range indicated on a 100-mm line: 0 mm (no pain) to 100 mm (worst imaginable pain)) were employed to rate pain intensity during block needle insertion. A four-point Likert scale derived from question 9 “The pain is difficult to endure” of Kolcaba’s General Comfort Questionnaire (GCQ) was used for scoring with 1 indicating strongly disagree and 4 indicating strongly agree to assess discomfort during block needle insertion. An 11-point scale from 0 (no pain) to 10 (pain as bad as you can imagine) derived from question 14 of the Zoster Brief Pain Inventory (ZBPI) was used to rate the ‘the worst pain’ [13]. For the assessment of burden of illness (BOI) since HZ rash onset, a severity-by-duration composite measure of pain using the area under the curve (AUC) of worst pain severity over time was employed to reflect the dynamic change of ZBPI ‘worst pain’. AUC was predefined as the area bounded by the curve and coordinate axis, taking time as the X-axis and pain severity on a 0–10 scale as the Y-axis, and calculated by multiple segment trapezoidal rule using GraphPad Prism version 5.0 (GraphPad Software Inc., San Diego, CA) [14]. QoL was evaluated by the EuroQoL 5-Dimension questionnaire (EQ-5D-3L), which was composed of five dimensions including mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension was composed of three levels: no problems, some problems, and extreme problems [15]. A designed booklet including ZBPI and EQ-5D questionnaires was completed by the patients once per week. PHN was predefined as ZBPI ‘worst pain’ score > 3 persisting at least 90 days after onset of rash [13, 16, 17]. The consumption of rescue analgesics for each patient was also recorded. Safety was assessed by adverse events.
The primary endpoint was HZ burden of illness (HZ-BOI) scores during 1 (D30) month after randomization. Secondary outcomes consisted of patients’ pain severity and discomfort degree during block needle insertion, other HZ-BOI scores, QoL scores, rescue analgesics consumption, and the incidence of PHN during follow-up.
Data CollectionData collection was conducted at baseline (D0), 1 (D30), 3 (D90), and 6 (D180) months by specially trained investigators following randomization. Questionnaire surveys were carried out through telephone or e-mail interviews on schedule.
Power AnalysisSample calculation was conducted using PASS software, version 16 (NCSS, LLC. Kaysville, UT, USA) on the basis of our pre-test composed of ten patients per group. An estimated cohort of 54 patients per group was generated for the study with 90% power and one-side type I error of 2.5% to assume that the POS approach was non-inferior to the proved TSA method (SD = 9.2) if the actual difference between two means of HZ-BOI during 1 month ranged from − 4.0 to 4.0. The acceptable non-inferiority margin (NIM) was set at − 10.0 based on the consensus after a series of clinicopathological conferences. The final sample size was 68 patients per group to compensate for 20% dropouts.
Statistically AnalysisStatistical analyses were performed by SPSS software, version 19.0 (SPSS Inc, Chicago, IL, USA). Statistical significance was set at the 5% level (two-tailed). Normal quantitative data, non-normal quantitative data, and categorical data were respectively reported as mean ± standard deviation (SD), median ± inter-quartile range (IQR), and percentage. Independent t test, Mann–Whitney U test and the chi-squared test were consequently used for comparison, respectively. HZ-BOI scores were compared using covariance (ANCOVA) model, taking the baseline values as the covariate. Analyses were conducted on the intention-to-treat (ITT) principle, missing values were dealt with multiple imputation (MI) using linear regression model, logistic regression model, and multinominal logistic regression model to impute normal distribution variable, binary variable and ordered categorical variable, respectively.
留言 (0)