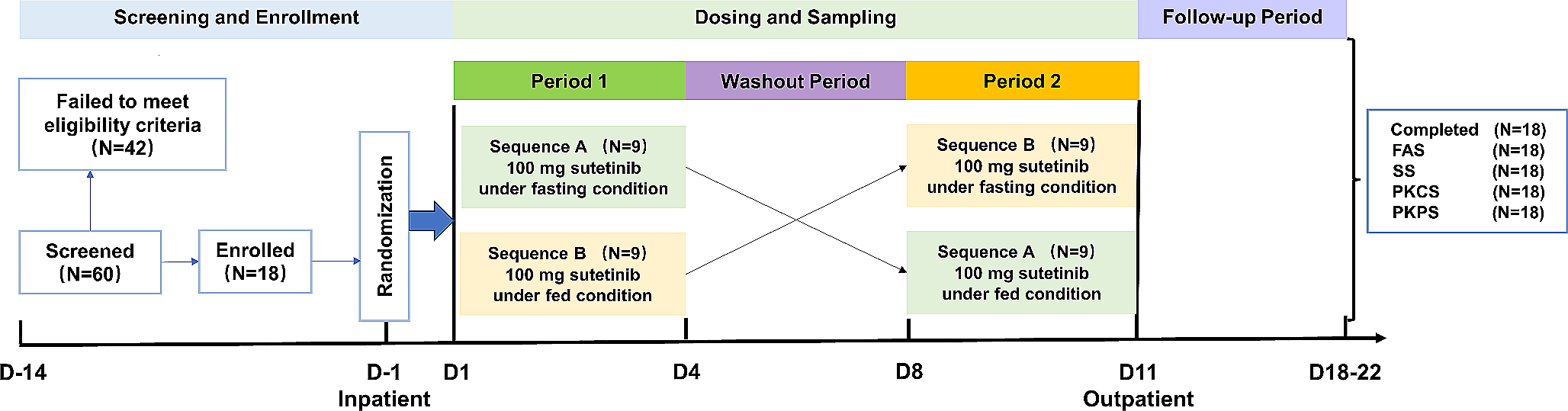
Study design
This open-label, parallel-group, inpatient, nonrandomized study was performed at 1 clinical study site, the Orlando Clinical Research Center (Orlando, FL, USA), and evaluated the PK of brigatinib after administration of a single oral 90-mg dose in participants with chronic hepatic impairment and in healthy participants with normal hepatic function. The study consisted of a screening period of up to 22 days and a single treatment and assessment period that included a 10-day (9-night) inpatient stay (Day −1 to Day 9). On the morning of Day 1, each participant received a single oral dose of 90 mg brigatinib under fasting conditions with approximately 240 mL of water. Fasting was required for approximately 10 hours before study drug dosing, for approximately 4 hours postdose, and for at least 8 hours before clinical laboratory tests. Meals were standardized for all participants. Water was permitted ad libitum except for the period between approximately 1 hour before and 1 hour after dosing. Participants remained in the clinic through 192 hours postdose for PK sample collection and were discharged from the clinical research site on Day 9.
Participants
Prior to study initiation, approval was obtained from the institutional review board of the study site and all participants provided written informed consent. This study was conducted in accordance with current Good Clinical Practice, the Declaration of Helsinki, the International Council for Harmonisation guidelines, and all applicable regulatory requirements.
Eligible participants included men or women of nonchildbearing potential, aged 18–70 years, body mass index (BMI) of 18.0–39.0 kg/m2, and a minimum weight of 50.0 kg at screening. Participants who smoked were eligible provided they did not exceed 5 cigarettes per day during the inpatient stay. Participants with hepatic impairment were classified according to Child-Pugh categories of mild (Child-Pugh A; total score of 5–6), moderate (Child-Pugh B; total score of 7–9), or severe (Child-Pugh C; total score of 10–15) hepatic impairment [16] based on physical examination findings and laboratory results assessed at screening. Permitted hepatic impairment etiology included chronic alcoholism, chronic viral hepatitis B or C, nonalcoholic steatohepatitis, autoimmune hepatitis, Wilson disease, alpha-1 antitrypsin deficiency, glycogen storage diseases, or galactosemia. Healthy participants with normal hepatic function were matched with participants with chronic hepatic impairment by age (± 10 years), sex, BMI (± 15% at screening), and if possible, comparable smoking habits. One healthy participant was to be matched by these criteria for approximately every 2 participants with hepatic impairment in all 3 categories combined. Healthy participants with normal hepatic function were free from clinically significant abnormalities based on medical history, vital signs, physical examination, 12-lead electrocardiogram, and laboratory evaluations at screening, per investigator assessment.
Investigational or prescription drugs were not permitted within 30 days before study drug administration except for chronic stable medications taken by participants with hepatic impairment. Use of over-the-counter drugs or herbal supplements was prohibited, except for acetaminophen (≤ 2000 mg/day) and vitamins (≤ 100% of the recommended daily allowance), within 72 hours before study drug administration. Participants were required to abstain from alcohol, caffeine-containing products, grapefruit and grapefruit-containing products, pomegranate, pomelo, star fruit products, Seville oranges, quinine-containing food or drink, and poppy seeds from 72 hours before study drug administration until the end of the inpatient confinement period. Healthy participants with a surgical or medical condition (other than cholecystectomy) that could have potentially interfered with the absorption, distribution, metabolism, or excretion of brigatinib were excluded from study participation.
Assessments
Blood samples were collected before brigatinib administration (predose) and at 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 12, 24, 36, 48, 72, 96, 120, 144, 168, and 192 hours following brigatinib administration to measure brigatinib plasma concentrations. Samples to assess brigatinib plasma protein binding were collected at 2, 8, and 24 hours postdose.
Bioanalytical methodsPlasma protein binding assay
Free fractions of brigatinib in plasma samples were determined as previously reported [17]. Briefly, free brigatinib was separated from protein-bound brigatinib by rapid equilibrium dialysis of plasma samples against warm (37° C) phosphate-buffered saline using the Thermo Scientific Single-Use Rapid Equilibrium Dialysis kit (Thermo Fisher Scientific, Waltham, MA) according to the manufacturer’s specifications. The semipermeable dialysis membrane had an 8000-dalton molecular weight cutoff. After incubation, samples were analyzed for brigatinib concentrations using liquid chromatography with tandem mass spectrometry as previously reported [14] using a dual-range assay with a lower limit of quantitation of 0.100 ng/mL and an upper limit of quantitation of 500 ng/mL.
Pharmacokinetics assay
Plasma samples were analyzed for brigatinib concentrations using a previously reported dual-range assay with a lower limit of quantitation of 0.100 ng/mL and an upper limit of quantitation of 2500 ng/mL [14].
Safety
All enrolled participants who received brigatinib were included in the safety population. Adverse event (AE) monitoring occurred throughout the study. Physical examination was conducted at screening with additional symptom-directed physical examinations performed at the investigator’s discretion on study Days −1 and 9. Height, weight, and BMI were recorded at screening. Vital signs were recorded at screening; on Day −1; predose and at 0.5, 1, 2, 3, 4, 6, 8, 12, 24, 36, 48, 72, 96, 120, 144, and 168 hours postdose; and on Day 9. Electrocardiograms were conducted at screening, on Day −1, predose and at 3 and 48 hours postdose, and on Day 9. Clinical laboratory evaluations were performed at screening and on Days −1 and 9 and were reviewed by the investigator for clinical significance.
Pharmacokinetic data analysis
The PK-evaluable population was defined as participants who received the single dose of brigatinib, had no major protocol deviations that affected the PK analyses, and had sufficient data to calculate PK parameters. Individual participant brigatinib plasma concentration-time profiles were analyzed via noncompartmental analysis using Phoenix WinNonLin version 6.4 (Certara, Inc., Princeton, NJ) to calculate plasma PK parameters. Plasma PK parameters calculated for brigatinib included maximum observed plasma concentration (Cmax), time to first maximum observed plasma concentration (Tmax), area under the plasma concentration-time curve from time 0 to the time of the last measurable concentration (AUC0−last), area under the plasma concentration-time curve from time 0 to infinity (AUC0−∞), terminal elimination half-life (t1/2), apparent oral clearance (CL/F), and apparent volume of distribution during the terminal disposition phase (Vz/F). The fraction of unbound brigatinib in plasma was calculated using the following formula: % free (unbound) = [free brigatinib concentration measured in buffer after dialysis] / [total brigatinib concentration measured in plasma] × 100. Unbound brigatinib PK parameters were derived from the following formula (except for the unbound CL/F and unbound Vz/F, which were calculated as total CL/F or total Vz/F divided by the individual participant’s overall mean fraction unbound): unbound PK parameter = (PK parameter based on total concentrations) × (individual participant’s overall mean fraction unbound value).
Statistical analysis
Descriptive statistics, including mean, standard deviation (SD), percent coefficient of variation (%CV), and median, minimum, and maximum values, were calculated for each time point for plasma brigatinib concentrations for the healthy participant and each Child-Pugh group. Arithmetic means, SD, %CV, median, minimum, and maximum values, and the number of observations were calculated for the PK parameters. Geometric mean and geometric %CV were derived for all parameters, except Tmax, which was reported as median (minimum–maximum). Statistical comparisons of unbound brigatinib PK parameters were made among the hepatic function groups (ie, healthy participants, Child-Pugh classes A, B, and C) using an analysis of variance. The geometric least-squares mean ratio (GMR) and 90% CIs were calculated for the comparison of Cmax,u, AUC0 − last,u, and AUC0−∞,u between each Child-Pugh group and the healthy participants with normal hepatic function group. Safety outcomes were summarized using descriptive statistics.

留言 (0)