
記住我

In this observational study, forty patients with an average age of 28.53 ± 4.06 years were enrolled. Twenty patients were assigned to the concave iris group and the other 20 patients were in the control group. All surgeries were performed by one surgeon (XZ) from June 2019 to November 2020, and during that time, we had a total of 8078 patients underwent EVO ICL implantation, so the frequency of patients presenting concave iris morphology was about 20/8078. The average follow-up period was 13.3 ± 5.3 months. Table 1 outlines the baseline data of all patients.
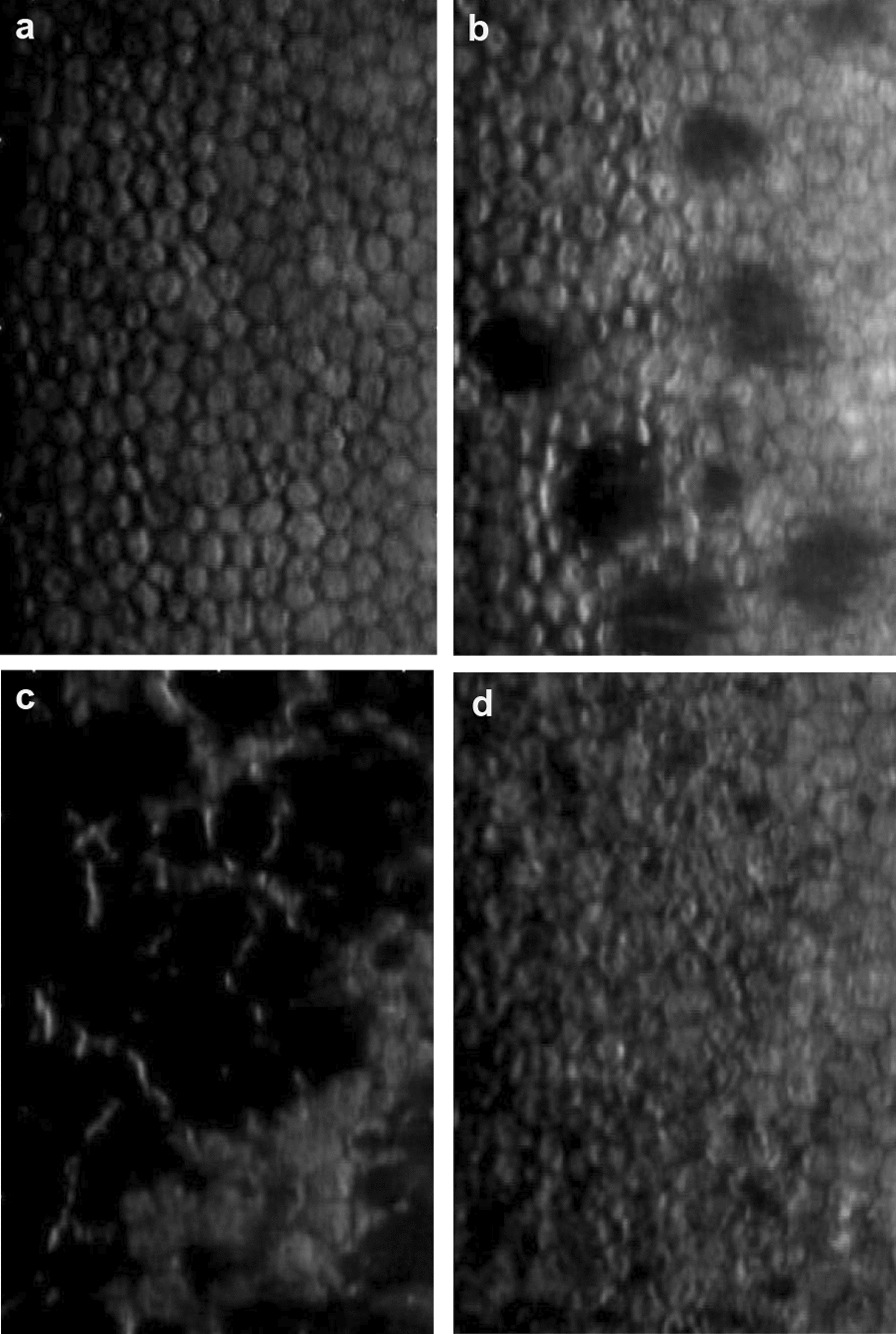
Table 1 Biometric data of subjects at baselineUBM was used to analyze the iris curvature (IC) and categorize different iris shapes [19] (Fig. 1a and b). Iris curvature was determined as the extent of posterior bowing of the iris and is measured by drawing a line from the iris root to the point of the pupil margin and then measuring the maximum perpendicular distance from the drawn line to the iris pigment epithelium [20] (Fig. 1c). The value of the iris curvature was considered positive if the iris showed a posterior deflection while "zero" or negative values were considered as belonging to the control group [21]. UBM was used to obtain the anterior segment parameters at baseline and follow-up visits.
Fig. 1
Description of iris morphology. a Typical concave iris in the concave iris group; b Typical planar iris in the control group; c Measurement of iris curvature (IC)
This observational study was approved by the Fudan University EENT Hospital Review Board (No. 2016038), and all work was carried out in accordance with the Declaration of Helsinki. All patients were fully informed of the details and potential risks of the procedure, and written informed consent was obtained.
The inclusion criteria were age 20 to 42 years, stable refractive error (≤ 0.50 D change per year in refractive error in the past two years), minimum anterior chamber depth of 2.8 mm and a minimum endothelial cell density (ECD) of 2000 cells/mm2, no contact lens use for at least two weeks. The exclusion criteria were the presence of comorbid eye disorders, suspicion of keratectasia and presence of comorbid systemic diseases.
ExaminationClinical examinationAll patients underwent preoperative and postoperative ocular examinations. The following main parameters were evaluated: uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), subjective manifest refraction, IOP (Canon, Japan), corneal topography and vault (Pentacam HR, Oculus Optikgeräte GmbH, Wetzlar, Germany) and UBM (Quantel medical, French). Anterior chamber angle pigment was observed by gonioscopy according to the five-class system developed by Scheie [22].
UBM measurementAll eyes were examined with the UBM. The patient was lying supine under standard room illumination, fixating on a target at a distance. All examinations were done by the same operator (LLN) and related parameters measured by another operator (ZZ). Topical 0.4% oxybuprocaine was instilled and an appropriately sized eye cup was inserted between the lids and filled with 2.5% methylcellulose and saline. The transducer tip was then placed in the fluid and each eye was examined at the 3-, 6-, 9-, and 12-o’clock positions. The following parameters (Fig. 2) were assessed using the linear and angular caliper provided by the instrument software, taking the average of the four directions and measuring to the second decimal position [23, 24].
Fig. 2
Ultrasound biomicroscopy (UBM) images of an eye showing the measurement of: a anterior chamber: irido-corneal angle (ICA), b posterior chamber: iris-lens contact distance (ILCD), posterior chamber angle (PCA), iris-zonule distance (IZD), ciliary process length (CPL)
Iris-lens/iris-ICL contact distance (ILCD): Determined by measuring the distance along the iris pigmented epithelium from the pupillary border to the point where the anterior lens (or EVO ICL) surface leaves the iris.
Anterior chamber angle (irido-corneal angle, ICA): Measured with the apex in the iris recess, and the arms of the angle passing through a point on the trabecular meshwork at 500 μm from the scleral spur and the point on the iris perpendicularly opposite. The size of the anterior chamber angle is given in degrees.
Posterior chamber angle (PCA): Measured with the apex in the posterior chamber recess, and the arms of the angle passing through the posterior border of iris and anterior border of the ciliary body at two points where a line extends from the corneal endothelium at 500 μm from the scleral spur. The size of the posterior chamber angle is given in degrees.
Posterior chamber distance (iris-zonule distance, IZD): This corresponds to the posterior chamber depth measured from the posterior iris surface (iris pigmented epithelium) to the first visible zonular fiber at a point just clearing the ciliary process.
Ciliary process length (CPL): Determined as the longest length in a straight line between the apex and the base of the ciliary process, as close as possible to a perpendicular from the sclera.
Surgical procedureThe surgical technique of ICL V4c implantations has described previously [25]. Briefly, pupils were dilated preoperatively. EVO ICL was implanted via a 3 mm temporal corneal incision by an injector cartridge. Then, the EVO ICL (STAAR Surgical, Nidau, Switzerland) was placed in the posterior chamber. After the surgery, a topical antibiotic (0.5% levofloxacin, Cravit, Santen, Osaka, Japan) was administered four times per day for seven days. A topical steroid (1.0% prednisolone acetate, Pred Forte; Allergan, Irvine, CA, USA) was used four times daily for four days, pranoprofen (Senju, Osaka, Japan) was used four times daily for 14 days and Natriumhyaluronat (Hycosan, Germany) was used four times daily for three months.
EVO implantable collamer lensThe power calculation of the EVO ICL was performed using a modified vertex formula based on the preoperative refractive parameters, according to the manufacturer’s instructions. The size of the EVO ICL was determined from the white-to-white and anterior chamber depth both obtained by Pentacam HR (Oculus Optikgeräte GmbH, Wetzlar, Germany).
Statistical analysesOnly data from the right eyes were included for analysis. All statistical analyses were performed using SPSS version 23 (IBM Corp, USA). The data were presented as the mean ± standard deviation. Normality of data was assessed using the Shapiro–Wilk test, and data were normal in all cases. The baseline biometric data and variables including iris curvature, ILCD, anterior and posterior chamber angle, distance of posterior chamber and ciliary process length were compared using unpaired t-test. Wilcoxon signed rank test was used to evaluate the pigment amount of the two groups. A P value of less than 0.05 was considered statistically significant.
留言 (0)