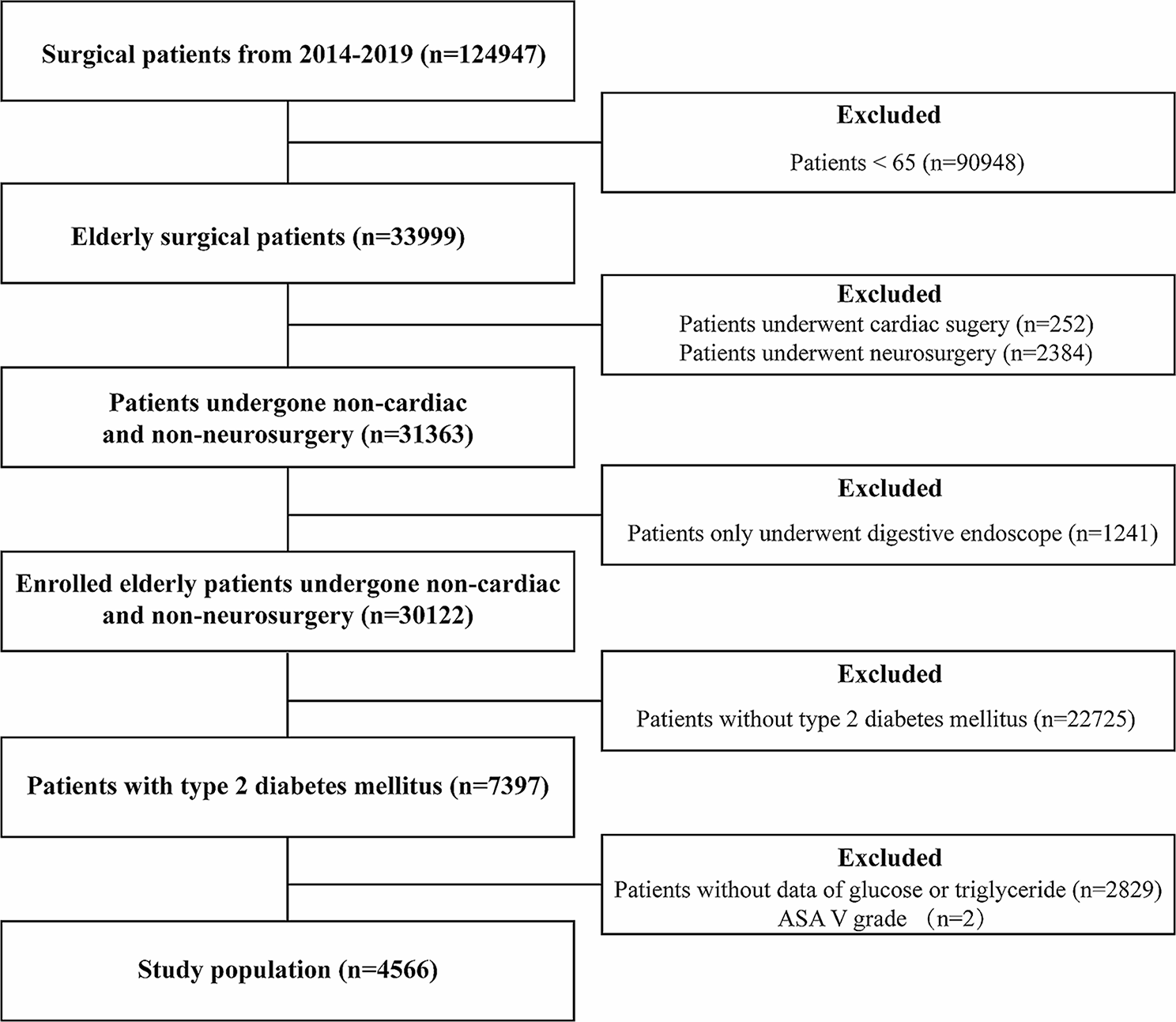
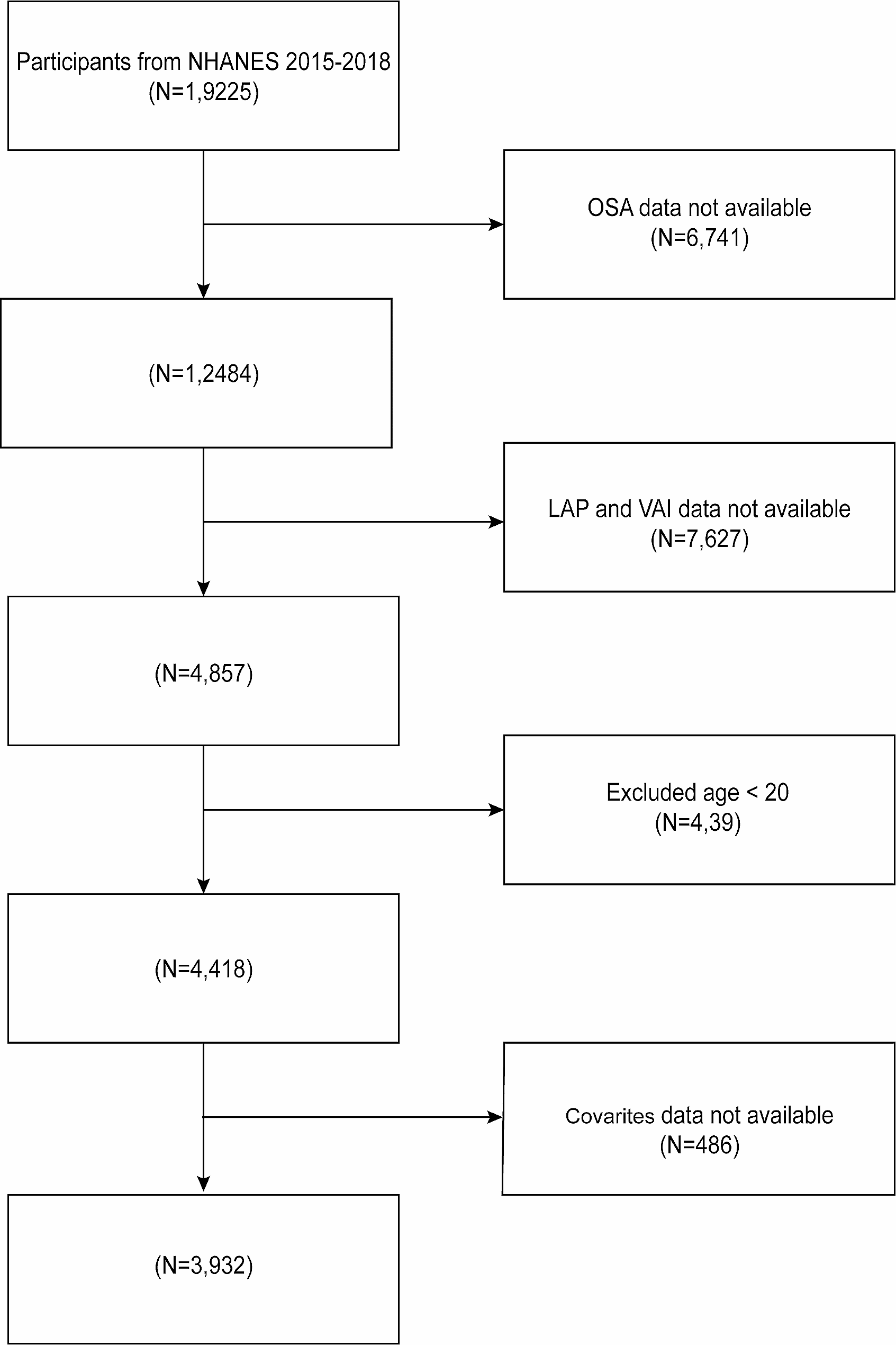
We described a screening program for severe HTG in Colombia. Figure 1 shows that 40 patients with elevated APOB and/or LDL levels suggesting mixed dyslipidemia were excluded according to a multivariate analysis in two published works that have been to be the best predictors of FCS [17, 24]. On the other hand, patients with CVD were also excluded because in real life, most patients are treated with statins that alter lipid metabolism. It is worth mentioning that the samples obtained for this study were taken in the city of Pereira, Colombia, with 477,027 habitants. Therefore, it constitutes a representative sample for the Risaralda Region.
Although HTG has a frequent presentation in clinical practice, severe HTG has a prevalence of only 1.7% in the United States [25], and FCS represents 1–3% of severe HTGs [12]. The prevalence of severe HTG in the present study was 3% (95% credible interval: 2.9–3.2) (n = 2415), with FCS representing a lower prevalence of 0.062% (95% credible interval: 0.0000657–0.16) of those severe HTGs, most likely due to a different cutoff point. Furthermore, the vast majority of these patients have MCS. Although the clinical suspicion could be somewhat simple (when the TG levels are extremely high), the low prevalence of the disease and the lack of knowledge and awareness might lead many patients to remain underdiagnosed. Moreover, patients can remain misdiagnosed or be diagnosed in advanced stages when they have already had complications derived from the disease [10, 16, 20, 26,27,28].
Between 2011 and 2013, a higher prevalence of HTG was identified in Russia in men ranging from 40 to 49 years old (42.8%) and women from 60 to 69 years old (34.4%) [29]. In the present study performed in a fourth-level care center in Pereira, Colombia, in the period between 2010 and 2020, 64.19% of patients with HTG were men, with a larger proportion between 45 and 55 years old, and in comparison, 35.81% were women, with a higher proportion between 50 and 60 years old. This is in concordance with the higher proportion of men in the SIMETAP-HTG study, which showed a prevalence of 34,6% for men and 21,4% for women [23]. The clinical manifestations of HTG are similar to those of both MCS and FCS, with symptoms extending from eruptive xanthomas, lipemia retinalis, and hepatosplenomegaly to recurrent episodes of AP. In this study, we found recurrent AP in 3 patients with no other signs or symptoms related to CS.
It is estimated that up to 85% of patients with severe HTG of any etiology will develop AP at some point in their life [30]. According to Retterstøl, K., et al., the prevalence of a history of AP is 17% in patients with severe HTG [18]. AP as a consequence of HTG represents the third leading cause of pancreatitis after biliary and alcoholic etiologies. Therefore, severe HTG constitutes a therapeutic challenge due to the possibility of developing hyperlipidemic acute pancreatitis, especially when TG levels exceed 1000 mg/dL, as the risk increases up to 5% [31]. In our study, the prevalence of pancreatitis in patients with FCS score ≥ 8 was significantly higher (6.9%) compared to those with a score < 8 (0.5%) (Table 4). A recent meta-analysis showed that pancreatitis caused by HTG is associated with higher levels of severity, mortality, and hospitalizations in intensive care units than other etiologies [14].
Table 4 Comparative analysis for the identification of factors associated with a probable case of familial chylomicronemiaThong et al. found in a study that in a population with very severe HTG, 13.4% of patients with HTG-induced acute pancreatitis had dyslipidemia, 15.9% presented hypertension and 28% had type 2 diabetes mellitus [30]. In the present study, 49.28, 32.43, and 19.6% of patients were identified with dyslipidemia, hypertension, and DM2, respectively. In addition, a prevalence of obesity of 12.9% was found, a figure lower than the data observed in the Norwegian study, which was 41.6% [18]. On the other hand, Pedragosa et al. found that 10.2% of patients with very severe HTG presented some episode of pancreatitis, 54% of patients had hepatic steatosis, 4.2% had gallstones, 3.4% had ischemic heart disease, 2.3% had cerebrovascular disease and 2.7% had peripheral artery disease [32]. These findings suggest that although pancreatitis is a major complication, it is important to be aware of cardiovascular outcomes as well. Goldberg et al. proposed that patients with FCS are younger and less likely to have any of the aggravating factors for HTG than those with MCS but are more likely to develop pancreatitis, probably because of life-long, sustained chylomicronemia [33]. They are less likely to have cardiovascular disease than those with MCS because of the severe reduction in LPL activity, which reduces atherogenic chylomicron and VLDL remnant formation and accumulation that may occur in MCS [33].
FCS results from mutations in one or more genes involved in lipolysis or the removal of circulating chylomicrons. In approximately 30% of patients, it is not possible to identify a specific causal variant. In this study, the presence of a variant (c.694 T > C, p. Ser232Pro) in the APOA5 gene (NM_052968.4), of uncertain significance associated with hyperlipoproteinemia-type disease 1D (MIM # 615947)/autosomal recessive in the carrier state was identified. When analyzing the clinical and paraclinical characteristics of these patients, 3 presented pancreatitis, overweight, or obesity with no other pathologies. It was confirmed through MLPA that 1 patient had an additional c. (?_50–1)_(161 + 1_162–1)dup duplication in the APOA5 gene, which makes the patient a compound heterozygote, whereby it would be the only confirmed diagnosis for familial chylomicronemia within the cohort at clinical evaluation that only had pancreatitis of the typical clinical picture of chylomicronemia.
APOA5 is a lipoprotein secreted in the liver, with concentrations of 150–400 ng/mL in plasma, which corresponds to 10,000 times less than the secretion of APOA1. Its structure is composed of 4 exons that encode 366 amino acids, similar in 27% to APOA4 in humans, located on chromosome 11q23 [34]. This gene is one of those responsible for facilitating the metabolism of triglycerides through the hydrolysis of LPL [34]. Several gene changes have been found to cause increased cardiovascular risk and severe HTG [35]. VUS, identified as common according to databases, is frequent in patients in this region.
There is evidence for several genes that act in the modulation and homeostasis of triglycerides. One of them is the GPIHBP1 gene, which encodes a glycoprotein of the lymphocyte antigen 6 family that is produced in the endothelium [36]. This glycoprotein is responsible for transporting LPL from the interstitium to the capillary lumen and subsequently to the capillary for LPL activation. Its structure consists of 4 exons and 228 amino acids with an N-terminal sequence followed by a C-terminal hydrophobic region similar to a glycosylphosphatidylinositol anchor [37].
One of the patients also had a variant in the GPIHBP1 gene (c.523G > C, p. Gly175Arg), also of uncertain clinical significance, associated with hyperlipoproteinemia type 1D (MIM # 615947) plus the variant in APOA5 already described in the carrier state for both genes, without a typical phenotype for familial chylomicronemia. Other variants in the same genes have been seen in other studies, such as in Singapore, where Loh et al. described a case report of a patient with a homozygous variant in APOA5 and a heterozygous common variant in GPIHBP1 who presented with subarachnoid hemorrhage with lactescent appearance [38]. In addition, in Norway, Retterstøl et al. diagnosed 2 female patients with primary HTG and a history of recurrent AP who had a homozygous mutation in exons 3 and 4 of the GPIHBP1 gene, and Lin et al. found a homozygous mutation in the same gene in a patient with a history of recurrent AP without mutations in the APOA5 gene [18, 36].
We only identified VUS in this study, making a diagnosis of FCS highly difficult to establish. We highlight the fact that these VUS were analyzed for cost-effectiveness in order to be able to characterize the clinical and biochemical parameters of the FCS, in which we compared the subgroups of score > 8 vs <8. Future studies should analyze enzymatic APOA5 levels to confirm the pathogenesis of this VUS.
Treatments for both FCS and MCS are almost different, constituting an important challenge for an adequate early diagnostic strategy. Most MCS patients have a good response to modifications in lifestyle, treatment of secondary factors, and triglyceride-lowering pharmacotherapies [16]. On the other hand, FCS patients have a poor response to triglyceride-lowering therapies such as fibrates, highlighting the need for other therapeutic strategies such as an extremely severe diet that restricts the consumption of long-chain fatty acids. Fortunately, there are recent studies with novel therapies such as inhibitors of apolipoprotein C-III under development to lower triglycerides in FCS subjects [16].
It is important to screen not only FCS patients but also MCS patients since those with some rare variants might be predisposed to worse phenotypes. Paquette et al. suggest genetic screening in patients with TGs ≥10 mmol/L to identify those at higher risk for AP [39]. However, this was not the purpose of this study. We aimed to describe a screening program for FCS with a stepwise approach, in which scores >8 or < 8 allowed us to analyze two subgroups of patients with FCS and MCS.
Study strengths and limitations
The strengths of this study are the sample size, and the fact that this was the first study exploring familial chylomicronemia syndrome in this region, proved that the unique variant we found has some degree of association in pancreatitis or death. In regard with limitations, the VUS found in this study needs further confirmation by enzyme levels. In addition, data was extracted by text mining using regular expressions, which could have not detected some conditions due to the writing methods because of its natural language. This could have affected the frequencies of signs and symptoms that might not have been written in the clinic histories, resulting in a possible subregistry.





留言 (0)