
記住我

The incidence of gastrointestinal (GI) neuroendocrine tumors (NETs) has continued to increase over the past several decades. Among these, rectal and small bowel NETs are the most common (1). Because NETs are frequently diagnosed incidentally on endoscopy or cross-sectional imaging or can present with GI symptoms, it behooves gastroenterologists to be able to recognize, diagnose, stage, and treat these increasingly common tumors.
ESTABLISHING A NET DIAGNOSIS Exercise caution in obtaining and interpreting NET markersChromogranin A (CgA) is the most common marker in the management of NETs but has limited sensitivity and specificity (2). It is not meant to be a screening test and is more appropriate after a confirmed NET diagnosis and in patients with measurable disease (metastases). CgA can be normal in patients with small and limited tumors (3). It is also frequently elevated in patients without NETs; while proton pump inhibitor use is by far the most common reason for false positive CgA, renal or hepatic insufficiency, and autoimmune atrophic gastritis are also associated with elevated CgA.
Endoscopic characteristics and considerationsGastroduodenal and rectal NETs are often incidentally found on routine endoscopy; most of them are not associated with a hormonal syndrome. Importantly, tumors with low malignant potential cannot be differentiated endoscopically from higher grade, more aggressive tumors. GI NETs may be firm, nonmobile, and polypoid or round with either a smooth overlying mucosa or central erosion or depression. They may also have an underlying red or yellow hue (Figure 1). Endoscopic ultrasound (EUS) characteristically demonstrates a hypoechoic, well-defined lesion within the deep mucosal and submucosal layers. Because NETs arise from enterochromaffin-like cells in the mucosal layer and infiltrate into the submucosa, biopsies with endoscopic forceps often establish a NET diagnosis, unlike other subepithelial lesions for which mucosal biopsies fail to obtain diagnostic tissue (4).
 Figure 1.:
Figure 1.: Endoscopic appearance of NETs. (a) Gastric NET (type III, grade 1). (b) Duodenal NET (grade 2). NET, neuroendocrine tumor.
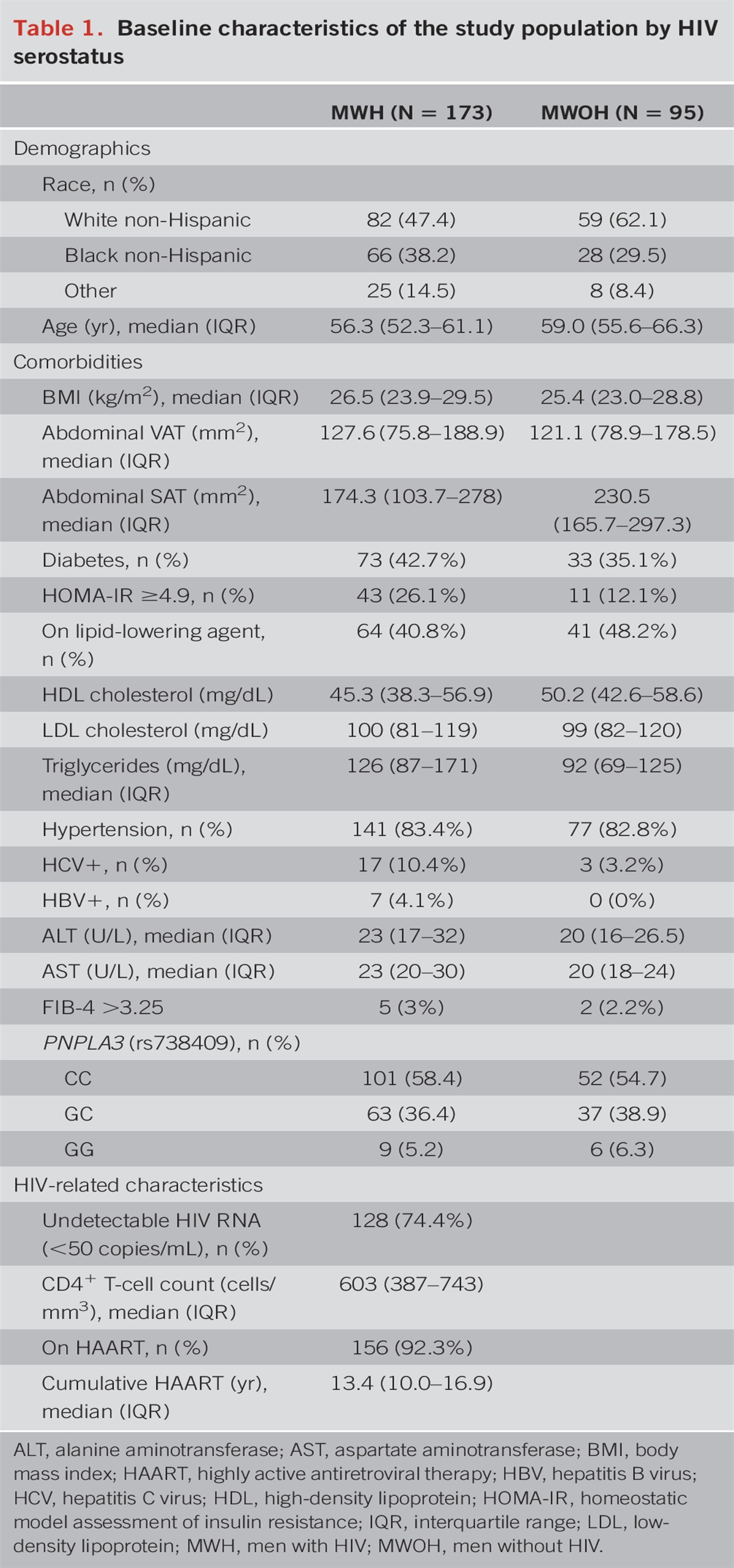
OBTAINING NET STAGE AND GRADEThe initial management of NETs is similar to that of any cancer. Because all NETs have malignant potential (i.e., the ability to invade or develop metastases), it is critical to adequately stage these tumors using the Tumor-Node-Metastasis classification (5). Tumor grade is also important to understand NET biology, which ultimately translates to how patients will fare. The World Health Organization classification identifies tumor grade using the mitotic index and Ki67 proliferation index (Table 1) (6), where increased mitotic rate and high Ki-67 index are associated with a more aggressive clinical course and worse prognosis.
 Table 1.: WHO NET grading classification (6)INITIAL NET MANAGEMENT
Table 1.: WHO NET grading classification (6)INITIAL NET MANAGEMENT
Accurate staging of NETs should be performed, as detailed in consensus guidelines (7,8). Locoregional staging is often adequate for most gastric, duodenal, and rectal lesions, whereas jejunal and ileal NETs should always be staged with cross-sectional and functional imaging. EUS allows for locoregional staging and assessment of endoscopic resection feasibility. Computed tomography or MRI should be performed for all jejunal and ileal NETs regardless of size because even subcentimeter lesions have a propensity to metastasize. Synchronous primary tumors, distant lymph nodes (LN), and secondary changes of desmoplastic, fibrotic reactions in adjacent tissue (Figure 2) can also be determined. Gallium‐68 Dotatate positron emission tomography (PET) scans have largely replaced the older octreotide scans with sensitivity and specificity of 91% and 94% for initial NET diagnosis (9). Computed tomography, MRI, and PET all have the ability to rule out distant metastatic disease, informing prognosis and management. However, diagnostic accuracy can be limited by size and morphology of the tumor, whereby subtle subcentimeter primary or metastatic lesions can be missed.
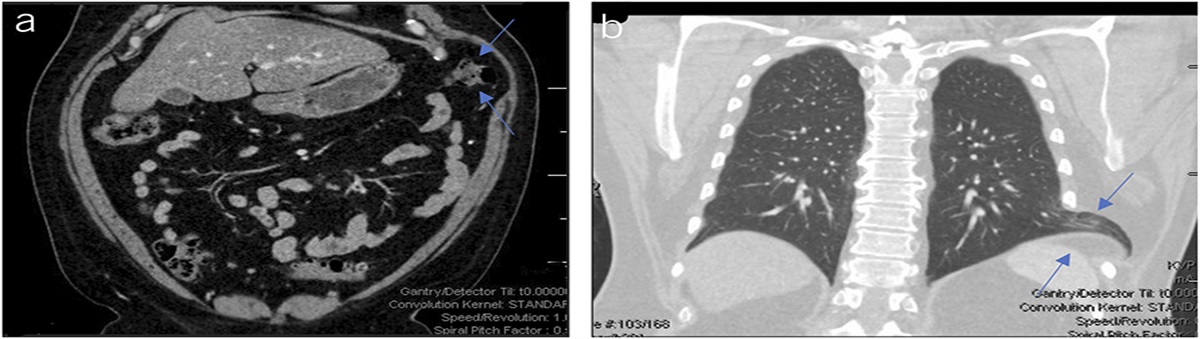
 Figure 2.:
Figure 2.: CT demonstrating desmoplastic reaction (tethering of adjacent bowel) by ileal NET. Image supplied courtesy of Dr. Calvin Sy. CT, computed tomography; NET, neuroendocrine tumor.
Given the correlation between tumor grade and prognosis, we strongly recommend referral of G2 and G3 NETs to a specialty center. In addition, a multidisciplinary tumor board discussion should also be considered. Genetic testing (Multiple Endocrine Neoplasia 1, Von Hippel Landau, Neurofibromatosis 1) may also be relevant.
ENDOSCOPIC MANAGEMENT OF NETSThe only definitive therapy of any NET is complete resection of the tumor, whether surgical or endoscopic. For most NETs (excluding those of the midgut), resection method depends on tumor size because this factor affects the likelihood of LN metastases.
Gastric NETsThe presence of normal gastrin or hypergastrinemia (whether acidic or achlorhydric) determines the subtype of gastric NET (Table 2). Type I gastric NETs have low potential for metastasis with 5- and 10-year survival equivalent to that of the general population (10). Type II gastric NETs are intermediate in metastatic potential; lesions >2 cm in size are associated with 10%–30% LN metastases and 5-year survival rate of 60%–75% (11). Type III gastric NETs are generally more aggressive than types I and II and are frequently metastatic at diagnosis with overall 5-year survival < 50% (12).
 Table 2.:
Table 2.: Gastric NET subtypes
Endoscopic resection may be considered for types I and II gastric lesions <2 cm, with surgery often warranted for larger lesions or lesions with deep invasion and nodal disease. Type III gastric NETs should be managed surgically, given the high incidence of LN metastases, although small (<1 cm) and intermediate (1–2 cm) type III, well-differentiated tumors without nodal disease may be considered for endoscopic resection (4,13). Given more advanced endoscopic resection techniques beyond endoscopic mucosal resection, including endoscopic submucosal dissection and full thickness resections, in addition to combined endoscopic and minimally invasive surgical techniques, future studies are needed to clarify the most appropriate technique and type of lesions appropriate for endoscopic resection. Conventional polypectomy techniques, however, are not recommended, given the high likelihood of incomplete resection of these subepithelial neoplasms. If endoscopic resection does not achieve negative margins (even microscopic positive margins) and/or there are more worrisome characteristics (lymphovascular invasion [LVI], G2/3), further management is warranted including multidisciplinary tumor board discussions.
Small intestinal NETsNETs should be assessed based on embryologic origin (foregut [duodenal] vs midgut [jejunal, ileal]). Duodenal NETs are often solitary and well-differentiated and can be managed endoscopically. Although there are no specific guidelines, resection is based on tumor size, which correlates with regional LN metastasis. Small (<1 cm), nonampullary, well-differentiated tumors without involvement of the muscularis propria can be endoscopically resected because the risk of LN involvement is low (2%) (14). Tumors 1–2 cm in size are associated with 4.7% risk of nodal involvement, whereas the risk increases to 20% in duodenal tumors >2 cm (15). Of note, it is difficult to obtain an R0 resection, which is estimated to be 50%–60% (14,16). After endoscopic resection, if pathology demonstrates positive margins, LVI, or G2/3, surgery referral is appropriate.
Surgical resection is recommended for all jejunal and ileal NETs, regardless of size because of the high potential for metastasis; in addition, they are often multicentric (20%) (17). It is often challenging to make the diagnosis of midgut NETs at an early stage because the primary tumors tend to be small and difficult to identify on cross-sectional imaging. Symptoms of partial obstruction, abdominal pain, and bleeding portend an advanced stage. Furthermore, carcinoid syndrome generally represents the development of metastases, which is the initial presentation in 35% of midgut NET cases in large population-based studies (15) and >60% of cases at tertiary referral centers (18).
Rectal NETsRectal NETs are commonly discovered incidentally during colon cancer screening, and most are small (<1 cm). The key is to have a high index of suspicion and to properly biopsy for tissue diagnosis yet leave enough tumor and/or mark with tattoo to aid a future curative resection. Staging with either EUS or MRI should be considered (19). Subcentimeter rectal NETs without muscularis propria invasion, LVI, or nodal disease can be endoscopically resected with a 98.9%–100% 5-year survival rate (20). Endoscopic resection can also be considered for carefully selected NETs 1–2 cm in size if there are a lack of nodes and deep invasion on either EUS or MRI. Surgery is recommended for tumors >2 cm in size, given the high propensity for metastatic disease (4). However, as with gastroduodenal NETs overall, optimal management should be individualized.
CONCLUSIONGiven the increasing incidence and prevalence of NETs, gastroenterologists will encounter NETs during their careers. Because we often diagnose NETs, the importance of our role in this disease cannot be overstated. A high index of suspicion is needed when encountering these lesions on routine endoscopy. Obtaining accurate NET stage and grade is critical to patient assessment and management and understanding overall prognosis. Many NETs can be managed successfully by gastroenterologists but may also require assistance from advanced endoscopists.
CONFLICTS OF INTERESTGuarantors of the article: Julie Yang, MD, Michelle Kang Kim, MD, PhD.
Specific author contributions: J.Y.: first author. M.K.K.: senior author.
Financial support: None to report.
Potential competing interests: None to report.
REFERENCES 1. Dasari A, Shen C, Halperin D, et al. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol 2017;3(10):1335–42. 2. Tseng C-M, Cheng T-Y, Chen T-B, et al. Low accuracy of chromogranin A for diagnosing early stage pancreatic neuroendocrine tumors. Oncol Lett 2018;15(6):8951–8. 3. Arnold R, Wilke A, Rinke A, et al. Plasma Chromogranin A as marker for survival in patients with metastatic endocrine gastroenteropancreatic tumors. Clin Gastro Hep 2008;6(7):820–7. 4. ASGE Standards of Practice Committee, Faulx AL, Kothari S, Acosta RD, et al. The role of endoscopy in subepithelial lesions of the GI tract. Gastrointest Endosc 2017;85(6):1117–32. 5. Amin MB, Edge SB, Greene FL, et al. AJCC Cancer Staging Manual. 8th edn. Springer: New York, 2017. 6. Nagtegaal ID, Odze RD, Klimstra D, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology 2020;76(2):182–188. 7. Shah MH, Goldner WS, Benson AB, et al. Neuroendocrine and adrenal tumors, version 1.2022, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2021;19(7):839–68. 8. Howe JR, Cardona K, Fraker DL, et al. The surgical management of small bowel neuroendocrine tumors: Consensus guidelines of the north American neuroendocrine tumor society. Pancreas 2017;46(6):715–31. 9. Singh S, Poon R, Wong R, et al. 68Ga PET imaging in patients with neuroendocrine tumors: A systematic review and meta-analysis. Clin Nucl Med 2018;43(11):802–10. 10. Borch K, Ahren B, Ahlman H, et al. Gastric carcinoids: Biologic behavior and prognosis after differentiated treatment in relation to type. Ann Surg 2005;242(1):64–73. 11. Scherubl H, Cadiot G, Jensen RT, et al. Neuroendocrine tumors of the stomach (gastric carcinoids) are on the rise: Small tumors, small problems? Endoscopy 2010;42(8):664–71. 12. Modlin IM, Sandor A. An analysis of 8305 cases of carcinoid tumors. Cancer 2000;79(4):813–29. 13. Deprez PH, Moons LMG, OʼToole D, et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European society of gastrointestinal endoscopy (ESGE) guideline. Endoscopy 2022;54(4):412–29. 14. Matsueda K, Kanesaka T, Kitamura M, et al. Favorable long-term outcomes of endoscopic resection for nonampullary duodenal neuroendocrine tumor. J Gastroenterol Hepatol 2021;36(12):3329–36. 15. Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35, 825 cases in the United States. J Clin Oncol 2008;26(18):3063–72. 16. Gincul R, Ponchon T, Napoleon B, et al. Endoscopic treatment of sporadic small duodenal and ampullary neuroendocrine tumors. Endoscopy 2016;48(11):979–86. 17. Niederle B, Pape UF, Costa F, et al. ENETS consensus guidelines update for neuroendocrine neoplasms of the jejunum and ileum. Neuroendocrinology 2016;103(2):125–38. 18. Norlen O, Stalberg P, Oberg K, et al. Long-term results of surgery for small intestinal neuroendocrine tumors at a tertiary referral center. World J Surg 2012;36(6):1419–31. 19. Gleeson FC, Levy MJ, Dozois EJ, et al. Endoscopically identified well-differentiated rectal carcinoid tumors: Impact of tumor size on the natural history and outcomes. Gastrointest Endosc 2014;80(1):144–51. 20. Soga J. Early-stage carcinoids of the gastrointestinal tract: An analysis of 1914 reported cases. Cancer 2005;103(8):1587–95.
留言 (0)