Despite reports on the ocular effects of COVID-19 vaccination being limited until now, certain studies have observed diverse manifestations of ocular phenomena following COVID-19 vaccination. These studies cover a wide range of presentations, including anterior uveitis [14, 15], posterior uveitis [16], multifocal choroiditis [17], panuveitis, Vogt–Koyanagi–Harada syndrome (VKH) [18], and white dot syndromes[19] (Table 2). Nevertheless, most reports have insufficient evidence other than the temporal association to prove the causality between the described ocular inflammation and COVID-19 vaccination. Presumed cases of uveitis related to COVID-19 vaccination reported in the literature include new presentations of onset bilateral juvenile idiopathic arthritis (JIA)-associated anterior uveitis, unilateral anterior uveitis, bilateral choroiditis, and bilateral panuveitis, in addition to the recurrence of VKH syndrome [14,15,16,17].
Table 2 Summary of the literature studiesClinical presentations of vaccine-associated uveitis
Among the literature describing ocular inflammatory events following COVID-19 vaccination, most reports noted the occurrence of anterior segment inflammation. Recently, a large-scale study including 1094 cases of vaccine-associated uveitis from different countries was reported, summarizing the results from adverse event reporting system; anterior uveitis remained as the most common observed vaccine-associated uveitis (VAU) [23]. Similar to our report, a female predominance was observed in the reported VAU cases. Another large case series for anterior segment inflammation was reported by Testi et al. in a multicenter study of 70 patients. In this series, the most common postvaccination inflammatory events were anterior uveitis (58.6%), followed by posterior uveitis (12.9%) and scleritis (10%). Most patients were managed with topical corticosteroids, with vision remaining the same for 92.9% of cases [24].
Posterior segment involvements in vaccine-associated uveitis
On the other hand, a few reports revealed potential retinal layer or posterior segment involvement following COVID-19 vaccination, suggesting neurological tissue inflammation. In Israel, Rabinovitch et al. reported 21 cases of uveitis following COVID-19 vaccination, of which two cases also developed multiple evanescent white dot syndrome (MEWDS) affecting the retina [22]. Pichi et al. described seven patients presenting with uveitis, along with two instances of rare clinical entities, namely, acute macular neuroretinopathy (AMN) and paracentral middle maculopathy (PAMM) [25]. Similar to the multicenter report by Testi et al. [24], most of the ocular inflammatory events observed by Pichi et al. occurred after patients received the Pfizer-BioNTech vaccine.
Several mechanisms have been suggested to explain ocular inflammatory responses following COVID-19 vaccination. Among them, the most generally accepted theories include the activation of antigens generated secondary to molecular mimicry resulting from similarities between vaccine and uveal peptides, type III hypersensitivity reactions, and other innate immune reactions induced by vaccination [26, 27]. In sum, our study reported the temporality of COVID-19 vaccination and the onset of ocular inflammatory events, observing relatively short intervals between these two events. Causality is possible given current understanding of uveitis events following other vaccinations, as well as generally accepted proposals for biological responses following vaccination.
Newly observed uveitis entities in our series
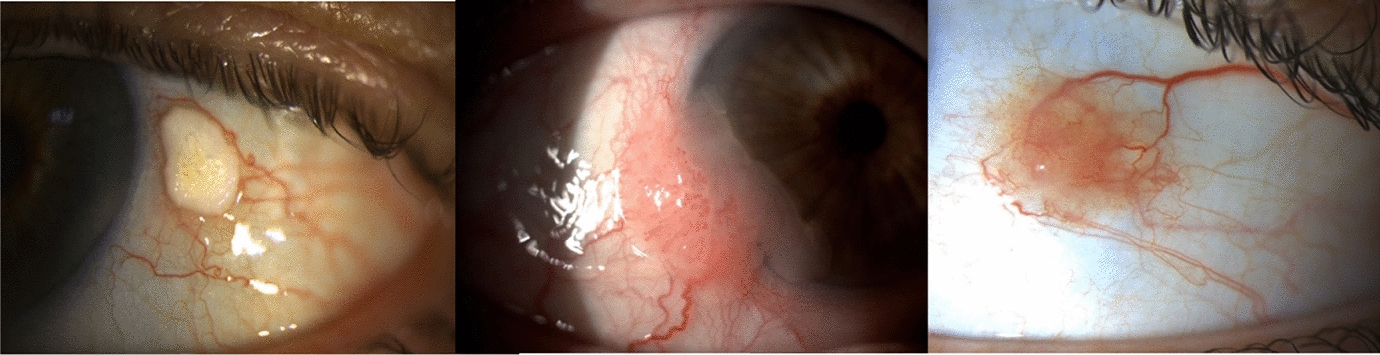
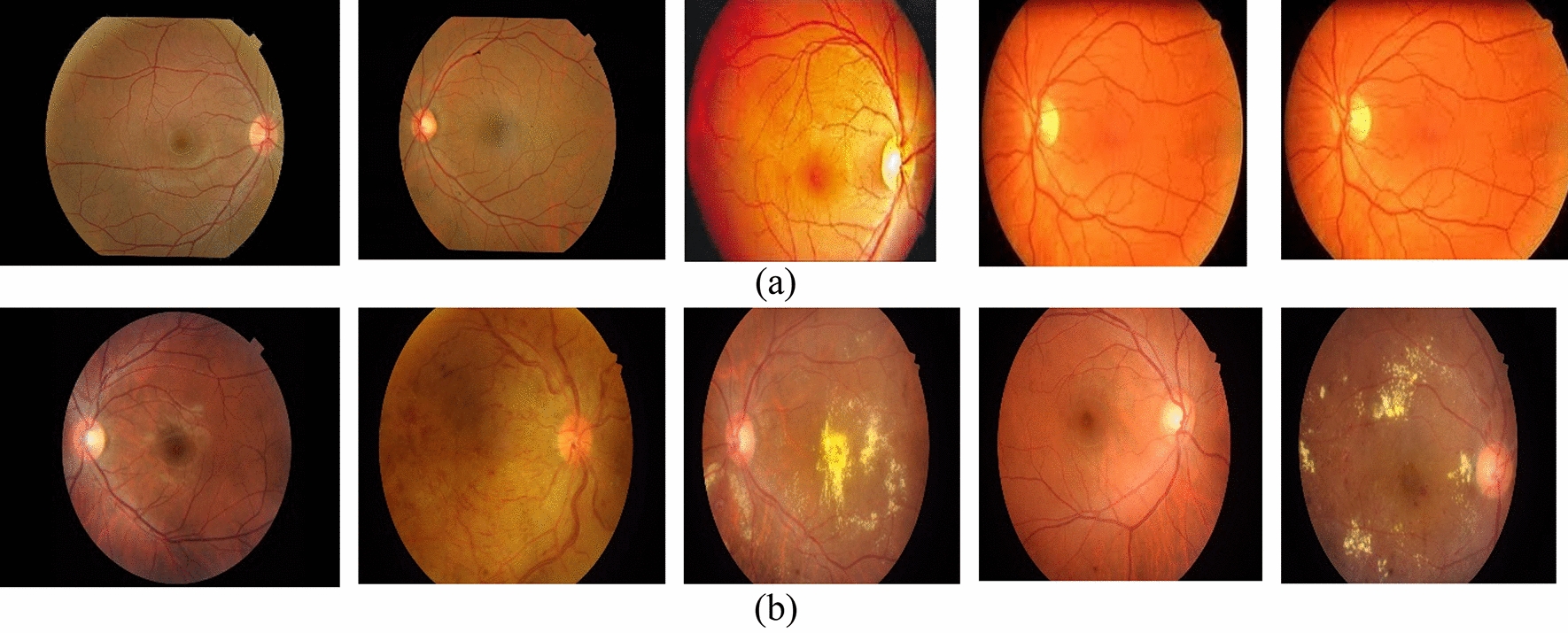
In our case series, we also report a new entity of frosted branch angiitis, choroiditis, and outer retinal inflammation, which mimics a mixed picture of widespread retinal vasculitis and choroiditis, following the administration the CoronaVac inactivated whole-virus vaccine. Formulating from harvested, inactivated, and purified whole particles of the SARS-CoV-2, the CoronaVac vaccine is generally expected to induce a broader immune response compared to mRNA vaccines that only target spike proteins [28, 29]. Neutralizing antibodies and/or activated T-helper cells may cross-react with proteins and antigens in multiple ocular tissue layers, including parts of the retinal vessels, outer retinal layers, retinal pigment epithelial cells, and the choroid. So far, retinal vasculitis has only been reported following COVID-19 infection [30]. This case in our series illustrated the potential for COVID-19 vaccines to induce similar vascular inflammatory events, albeit to a milder extent than infection.
In our series, most patients presenting with anterior uveitis (six out of seven patients) experienced uveitis attacks after receiving the Comirnaty vaccine, whereas only one patient developed ocular inflammation involving multiple layers of chorioretinal tissue after receiving the CoronaVac vaccine. The differences in the technologies used by both vaccines may imply distinct immunogenicity mechanisms specific to each vaccine platform. Considering the low occurrence rates of vaccine-related uveitis, continued data collection and future research are warranted to evaluate the safety profiles of each vaccine, including ocular side effects. Nevertheless, given that nearly all uveitis cases following vaccination with the Comirnaty vaccine could be resolved rapidly and completely following a short course of topical steroids, the benefits of vaccination still far outweigh the potential risk of ocular adverse events.
Clinical course of the available VAU case series
Within the current literature, anterior uveitis is the most prevalent presentation of uveitis flare-ups after various vaccination regimens, followed by intermediate uveitis. The literature also observes that most reported cases resolve rapidly following one course of topical steroids. In the most comprehensive review of vaccine-induced uveitis yet, Benage and Fraufelder identify a median time range from vaccination to uveitis onset of 16 days (range: 1 day–6 years) [4]. For our case series, the median date of anterior and intermediate uveitis presentations was 15 days (range: 0–6 weeks) following vaccination with the Comirnaty vaccine. Our series did not include specific antibody tests and titrations for the SARS-CoV-2. Nevertheless, factors including the temporal sequence of vaccination and disease events, the absence of identifiable alternative causes from accessory examinations, the transience of severe ocular inflammation symptoms, and good treatment responses to steroids all strongly suggest that uveitis can be a vaccine-induced immune response.
Potential mechanisms for vaccine-associated uveitis
Of the two available vaccines in Hong Kong, the Comirnaty mRNA vaccine uses lipid nanoparticle encapsulated mRNA to encode a full-length spike protein of the SARS-CoV-2, which is also locked down by two proline mutations to avoid integration into the host cell genome [31]. This vaccine induces strong activation of the cellular and humoral immune responses, exhibiting dose-dependent side effects [32]. Because of the similarities between the SARS-CoV-2 spike protein and proteins in uveal tissues, molecular mimicry may cause immune cross-reactivity, triggering autoimmune diseases such as anterior uveitis [31, 33]. In accordance with available reports, most cases in our series developed uveitis following the second dose of COVID-19 vaccines, potentially because of greater, and possibly dose-dependent, reactogenicity.
Several mechanisms have been suggested to explain ocular inflammatory responses following COVID-19 vaccination. Among them, the most generally accepted theories include the activation of antigens generated secondary to molecular mimicry resulting from similarities between vaccine and uveal peptides, type III hypersensitivity reactions, and other innate immune reactions induced by vaccination [26, 27]. In sum, our study reported the temporality of COVID-19 vaccination and the onset of ocular inflammatory events, observing relatively short intervals between these two events. Causality is possible given current understanding of uveitis events following other vaccinations, as well as generally accepted proposals for biological responses following vaccination.
Potential role of vaccines in creating inflammatory reaction less than the extent of cytokine storms by SARS-CoV-2 may provide us an insight into the potential mechanisms of vaccine-associated uveitis. Coronavirus-2 (SARS-CoV-2) causes acute respiratory distress syndrome (ARDS) in 15% of COVID-19 cases. ARDS is mainly triggered by elevated levels of pro-inflammatory cytokines, referred to as cytokine storm which is induced by an excessive immune response rather than the viral load. Cytokine storm is defined as acute overproduction and uncontrolled release of pro-inflammatory markers systemically, as well as reduced macrophages functions and peripheral lymphopenia [34, 35].
Besides, recent studies suggest that excessive production of some cytokines, such as interleukin-6, interleukin-1, interleukin-17, and tumor necrosis factor-alpha, may be the leading cause of inflammatory response in COVID-19-related cytokine storms [36]. We understand that these interleukins and inflammatory factors play a crucial role in many ocular inflammatory events. Also, SARS-CoV-2 has a predilection target at organs expressing ACE2 receptor, which is abundantly expressed in the pulmonary system, and to a lesser extent, in the eye and brain. Thus, ocular tissue is also highly suspectable to SARS-CoV-2 entry and replication. These two factors may shed a light into the phenomenon of vaccine-associated uveitis.

留言 (0)