
記住我



Presbyopia-correcting intraocular lens (PC-IOL) technology has been available for over a decade. Historically, PC-IOL lens designs have included refractive (eg, Johnson & Johnson ReZoom), apodized diffractive (eg, Alcon AcrySof ReSTOR), nonapodized diffractive (eg, Alcon AcrySof PanOptix), accommodating (Bausch & Lomb Crystalens), and diffractive extended depth-of-focus (EDOF; eg, Johnson & Johnson Symfony) technology. Despite their ability to provide higher levels of spectacle independence than monofocal IOLs, PC-IOLs are not without drawbacks.1,2 Any IOL that splits light to deliver distinct distance and near foci creates the potential for photic phenomenon, which patients may perceive as glare, halos, starbursts, or hazy vision.3,4
The Vivity (DFT015, Alcon Laboratories, Inc.) is a nondiffractive EDOF (ND-EDOF) IOL that has a high magnitude of negative spherical aberration in the center to deliver an extended range of vision. When targeted for emmetropia, eyes implanted with this ND-EDOF IOL have been reported to have excellent intermediate vision, improved near vision, and comparable photic phenomena profiles when compared with monofocal IOLs such as the Alcon AcrySof SN60WF IOL.5 However, the SN60WF contains negative spherical aberration, which may decrease the depth of focus when paired with the cornea's naturally positive spherical aberration (SA). On the other hand, the enVista (MX60E, Bausch & Lomb, Inc.) is a neutral aspheric monofocal IOL that may allow the cornea's naturally positive SA to act unperturbed, thereby delivering a small amount of pseudoaccommodation when compared with other monofocal IOLs. In fact, in a previous ASCRS paper presentation, Stephenson reported that patients implanted with the enVista IOL had monocular uncorrected intermediate (UCIVA) and near (UCNVA) visual acuities of 0.17 ± 0.14 (≈20/30) and 0.44 ± 0.3 (≈20/55) logMAR, respectively.6 To the authors' knowledge, there is no additional literature on the intermediate or near vision performance of this monofocal IOL.
The purpose of this study was to compare the objective visual and patient-reported outcomes of the aforementioned Vivity ND-EDOF and enVista monofocal IOL in patients bilaterally implanted with 1 of these 2 IOLs and targeted for emmetropia.
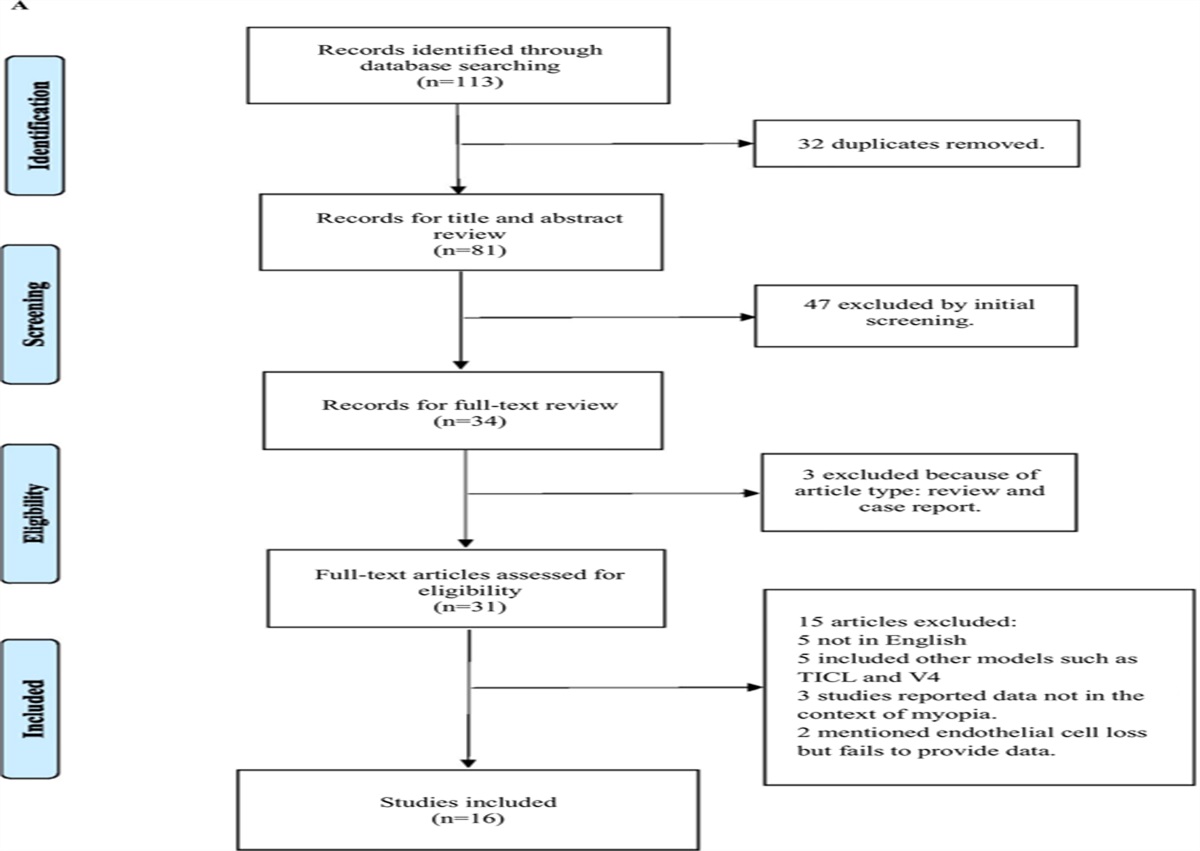
METHODSThis was a prospective, single-center, patient- and assessor-masked, double-arm, randomized controlled trial. Before enrollment of study patients, the protocol and study-specific informed consent was approved by the Penn State College of Medicine Institutional Review Board. The study adhered to the tenets of the Declaration of Helsinki and was registered at ClinicalTrials.gov (NCT# 04591054) before any patients were enrolled.
Eligible patients included patients aged 18 years or older with visually significant cataract, an anticipated postoperative visual acuity of 0.2 logMAR (≈20/32) or better, calculated spherical equivalent (SE) power targeted for emmetropia, calculated IOL power between +10 diopters (D) and +25 D inclusive, and measured against-the-rule astigmatism less than 0.5 D or with-the-rule/oblique astigmatism less than 1.0 D, in both eyes. If the patient was a contact lens wearer, they must have had a willingness to discontinue lens wear for ≥21 days before preoperative biometry. Exclusion criteria included hypermature cataract, visually significant intraocular media opacity other than cataract, abnormal cornea findings, anterior segment pathology (eg, poor pupil dilation and pseudoexfoliation), retinal pathology (eg, macular degeneration), or history of other ocular disease that could, in the investigator's opinion, alter postoperative visual prognosis. Patients planned to undergo other concomitant ocular procedures at the time of cataract surgery were also excluded.
Patients who gave written consent to participate underwent preoperative testing including optical biometry (IOLMaster 700, Carl Zeiss Meditec AG) and corneal topography (Galilei G4, Ziemer Ophthalmic Systems AG). Patients also completed 2 questionnaires that sought to elucidate the presence and severity of visual disturbances and how bothersome they are (Questionnaire for Visual Disturbances [QUVID], Alcon Laboratories, Inc.), spectacle usage at various distances and lighting conditions, and patient satisfaction (Intraocular Lens Satisfaction [IOLSAT], Alcon Laboratories, Inc.). They were then randomized to receive either the Vivity (DAT015) or enVista (MX60E) IOL in both eyes, targeted for emmetropia. Randomization was performed using a block design by randomizing 40 patients to 2 study groups using 10 blocks of 4 group assignments (2 for each group) within each block. The order of those blocks was randomized as well. The Barrett Universal II formula and lens factor (LF) of 1.99 were used in all cases to determine the appropriate IOL power. This LF was chosen because it correlates with an A-constant of 119.2, which is the manufacturer's suggested starting point for both of these IOLs.7 Surgery was performed using phacoemulsification through a temporal 2.4 mm corneal incision. Postoperatively, patients were seen 1 day and 1 week after each procedure by the surgeon and then 1 month and 3 months after the second-eye procedure by an examiner who was masked to the IOL implanted. Only after all study-related assessments were completed was both the patient and assessor unmasked as to the IOL implanted in both eyes.
At both 1- and 3-month study visits, manifest refraction, uncorrected distance (UDVA), intermediate (UIVA), and near (UNVA) visual acuities, as well as corrected distance (CDVA), distance-corrected intermediate (DCIVA), and distance-corrected near (DCNVA) visual acuities were evaluated both monocularly and binocularly. All visual acuity testing was performed under photopic conditions using the standard ETDRS chart (4 m) and Sloan letter intermediate (66 cm) and near (40 cm) cards. At the 3-month study visit, binocular defocus curve testing was performed, as were the same 2 validated questionnaires to assess for the presence and severity of visual disturbances (QUVID) and spectacle independence (IOLSAT).
Before commencing the study, a sample size calculation was performed. The U.S. Food and Drug Administration Summary of Safety and Effectiveness Data on the Vivity IOL compared the Vivity with the AcrySof IQ SN60WF IOL.8 It demonstrated a binocular DCIVA of 0.054 ± 0.09 logMAR and 0.196 ± 0.113 logMAR units, respectively (difference of 0.142). We hypothesized that the neutral asphericity of the enVista IOL would result in a slightly improved DCIVA compared with that of the SN60WF IOL. As such, we assumed that the mean difference in the DCIVA between the 2 IOLs would be ≥0.12 logMAR units and that the SD on these measurements would be approximately 0.10. Based on a difference in binocular DCIVA of 0.12 logMAR units and a SD of 0.10, an α of 0.05, and power of 0.80, it was determined that 22 bilaterally implanted patients would be required in each group. Enrollment was thus anticipated to include 28 per group (56 in total) to more closely approximate a normal distribution and ensure adequate numbers after accounting for screen failures and a lack of follow-up.
All data were stored in REDCap (Vanderbilt University), and SAS software v. 9.4 (SAS Institute, Inc.) was used to facilitate statistical analysis. Descriptive statistics (mean ± SD or n [%]) were used to summarize demographics, refractive outcomes, and postoperative visual acuities of the study groups. The normality of the data was evaluated using the Kolmogorov-Smirnov test. A 2-sample t test (parametric), Wilcoxon sum-rank test (nonparametric), or chi-square test (proportions) was used to compare outcome measures between the 2 groups of patients. A linear mixed effects model for means or a generalized estimating equation model for proportions was used to make comparisons between study groups for outcomes measured on eyes rather than on patients to account for the correlation between eyes from the same patient.
RESULTSA total of 56 patients were enrolled, 28 in each group. In the Vivity group, 4 patients never completed the study; 1 patient did not meet inclusion/exclusion criteria after signing the consent, a second patient was lost to follow-up after signing consent and never scheduled surgery, a third voluntarily withdrew before the 1-month follow-up visit because of transportation limitations and the loss of a spouse, and the last patient never scheduled for their second-eye surgery because of a high deductible health insurance plan. In the enVista group, 1 patient was lost to follow-up after the 1-month visit. Thus, 24 patients in the Vivity group and 27 patients in the enVista group completed all study-related visits and were included in the final analysis. All the surgeries were uneventful and were completed without complication. Adverse events recorded included 2 corneal abrasions, 2 cases of cystoid macular edema, 1 case of increased ocular pressure, 2 cases of prolonged corneal edema, and 1 case of breakthrough inflammation, all treated and resolved without sequelae. In addition, 2 eyes from 1 patient developed early posterior capsular opacification, both of which were treated with YAG laser capsulotomy before their 3-month study visit. Table 1 displays demographics of the 2 groups. There were no differences with regard to relevant demographic or biometric variables (P > .05), except for a slightly more myopic predicted spherical equivalent in eyes implanted with the enVista IOL (P = .022).
Table 1. - Patient demographics Parameter Vivity enVista P value Patients/eyes (N) 24/48 27/54 Age (y) Mean ± SD 68.45 ± 6.53 68.34 ± 6.48 .952 Sex (% M) 16.7 29.6 .276 Race (%) .590 White 87.5 92.6 Black/African American 8.3 3.7 Asian 4.2 0 Others/not reported 0 3.7 Ethnicity (% Hispanic) 4.2 14.8 .352 Biometric variables AL (mm) 24.11 ± 1.06 23.87 ± 1.12 .438 Average K (D) 43.63 ± 1.52 43.92 ± 1.56 .500 Keratometric astigmatism (D) 0.53 ± 0.32 0.53 ± 0.29 .943 ACD 3.33 ± 0.39 3.19 ± 0.37 .178 Implanted IOL power 19.69 ± 2.73 20.18 ± 3.37 .577 Predicted postop SE −0.13 ± 0.10 −0.18 ± 0.11 .022*ACD = anterior chamber depth; AL = axial length; K = keratometry; SE = spherical equivalent
*Statistically significant
Table 2 displays the monocular refractive outcomes at 3 months. Refractions were performed while patients looked at the standard ETDRS charts at 4 m, but lens constants (LF) are typically optimized for 6 m. The lane length–adjusted monocular prediction errors were −0.10 ± 0.33 for Vivity and −0.03 ± 0.28 D for enVista (P = .326). There were no significant differences between groups with regard to the monocular absolute prediction error or the proportion of eyes within ±0.25 D, ±0.50 D, ±0.75 D, or ±1.0 D of the predicted SE.
Table 2. - Monocular refractive outcomes at 3 months postoperatively Parameter Vivity enVista P value Patients/eyes 24/48 27/54 Relative to emmetropia Spherical equivalent (D) −0.15 ± 0.32 −0.13 ± 0.28 .782 Proportion (%) ±0.25 D 68.8 74.1 .568 ±0.50 D 91.7 94.4 .568 ±0.75 D 95.8 100 N/A ±1.00 D 100 100 N/A Relative to predicted SEa Prediction error (D) −0.10 ± 0.33 −0.03 ± 0.28 .326 Absolute prediction error (D) 0.26 ± 0.22 0.22 ± 0.17 .274 Proportion (%) ±0.25 D 58.3 61.1 .773 ±0.50 D 87.5 92.6 .405 ±0.75 D 95.8 100 N/A ±1.00 D 100 100 N/AN/A = not available; SE = spherical equivalent
*Prediction error, absolute prediction error, and the proportion of eyes within target are reported based on using the Barrett Universal II formula and a lens factor of 1.99 and after accounting for lane length
Vision outcomes are illustrated in Figure 1. One patient in the Vivity group did not obtain an UDVA of 20/40 or better, and even after correction, their bilateral CDVA was ≈20/35. This patient was found to have cystoid macular edema and was treated beyond the study period, with the CDVA ultimately reaching 20/25 + 2. A similar proportion of patients in both groups obtained 20/20 (P = .214) or 20/25 (P = .106) binocular CDVA, but a significantly higher proportion of patients in the Vivity group obtained 20/20 (P < .001) or 20/25 (P < .001) binocular DCIVA. Patients implanted with the Vivity or enVista IOLs had a similar binocular UDVA (0.02 ± 0.13 [≈20/21] vs −0.03 ± 0.07 [≈20/19]; P = .393) and CDVA (−0.01 ± 0.10 [≈20/20] vs −0.05 ± 0.07 [≈20/18]; P = .188). However, the Vivity group had a significantly better binocular UIVA (0.01 ± 0.14 [≈20/20] vs 0.16 ± 0.11 [≈20/29]; P < .001), DCIVA (−0.02 ± 0.13 [≈20/19] vs 0.19 ± 0.14 [≈20/31]; P < .001), UNVA (−0.03 ± 0.14 [≈20/19] vs 0.16 ± 0.14 [≈20/29]; P < .001), and DCNVA (0.03 ± 0.12 [≈20/21] vs 0.17 ± 0.19 [≈20/30]; P = .004). This information is further summarized in Supplemental Figure 1 (https://links.lww.com/JRS/A777).
 Figure 1.:
Figure 1.: Cumulative binocular (a) UDVA, (b) CDVA, (c) UIVA, (d) DCIVA, (e) UNVA, and (f) DCNVA Snellen visual acuity cutoffs at 3 months postoperatively. ND-EDOF = nondiffractive EDOF IOL (Alcon AcrySof Vivity); monofocal (Bausch & Lomb enVista)
Figure 2 depicts binocular defocus curves for patients in the 2 groups. Patients in both groups performed similarly at emmetropia and with induced myopia up to 1.5 D (P > .053 in all cases). However, with increasingly higher levels of induced hyperopia, binocular distance visual acuity deteriorated more quickly in the enVista group. Differences between groups became significant at 1.0 D of induced hyperopia and maintained significance at +1.5 D, +2.0 D, and +2.5 D.
 Figure 2.:
Figure 2.: Defocus curve 3 months after bilateral implantation of a nondiffractive EDOF (ND-EDOF, Alcon AcrySof Vivity) or neutral aspheric monofocal (Bausch & Lomb enVista) IOL.
Table 3 summarizes patients' responses to the questionnaire evaluating for the presence, severity, and bothersomeness of visual disturbances (QUVID). There were no differences in the proportion of patients reporting the presence of starbursts (P = .26), halos (P = .37), glare (P = .23), hazy vision (P = .70), blurred vision (P = .41), double vision (P = .60), or negative dysphotopsias (P = 1.0). Among those who did report visual disturbances, there were no differences in the bothersomeness, except in regard to hazy vision (P = .03). In the Vivity group, 4 patients (16%) reported they were a little bothered, whereas in the enVista group, one patient (3.7%) reported they were somewhat bothered and another one patient (3.7%) reported being “quite a bit bothered.”
Table 3. - Comparison of photic phenomena for Vivity and enVista groups at 3 months postoperatively (after second-eye implantation) Patients reporting on the presence and severity of photic phenomena Vivity (N = 24) enVista (N = 27) Visual disturbance None (%) A little (%) Mild (%) Moderate (%) Severe (%) None (%) A little (%) Mild (%) Moderate (%) Severe (%) Starbursts 91.7 0 4.2 4.2 0 77.8 3.7 7.4 7.4 3.7 Halos 62.5 12.5 8.3 12.5 4.2 74.1 7.4 7.4 7.4 3.7 Glare 54.2 8.3 16 16 4.2 70.4 7.4 14.8 7.4 0 Hazy vision 83.3 8.3 8.3 0 0 88.9 3.7 0 3.7 3.7 Blurred vision 83.3 8.3 4.2 4.2 0 92.6 3.7 0 0 3.7 Double vision 95.8 0 4.2 0 0 100 0 0 0 0 Dark area Negative dysphotopsia 87.5 8.3 4.2 0 0 88.9 7.4 3.7 0 0 Patients reporting on bothersomeness of photic phenomena Visual disturbance Not at all bothered (%) A little bit (%) Somewhat (%) Quite a bit (%) Very much (%) Not at all bothered (%) A little bit (%) Some what (%) Quite a bit (%) Very much (%) Starbursts 91.7 4.2 4.2 0 0 81.5 7.4 3.7 7.4 0 Halos 79.2 8.3 4.2 8.33 0 88.9 3.7 3.7 0 3.7 Glare 59 20.8 16 0 4.2 70.4 14.8 11.1 0 3.7 Hazy vision 84 16 0 0 0 92.6 0 3.7 3.7 0 Blurred vision 83.4 4.2 4.2 8.33 0 92.6 3.7 0 0 3.7 Double vision 95.8 4.2 0 0 0 100 0 0 0 0 Dark area Negative dysphotopsia 91.7 4.2 4.2 0 0 92.6 3.7 0 0 3.7Table 4 summarizes responses to the questionnaire evaluating dependence on spectacles at various distances and lighting conditions (IOLSAT). Patients in the 2 groups reported similar independence from spectacles at distance under bright (P = .286) and dim (P = .051) lighting conditions. However, a greater proportion of patients in the Vivity group reported spectacle independence at intermediate under bright (P = .030) and dim (P = .018) lighting conditions. A greater proportion of patients in the Vivity group also reported spectacle independence at near under bright (P = .021) and dim (P = .001) lighting conditions. Although a similar proportion of patients rated their distance visual “good” or “very good” at distance, more patients in the Vivity group did so at intermediate and near than in the enVista group, regardless of lighting condition.
Table 4. - Patient-reported dependence on spectacles by distance and lighting condition Proportion of patients rarely or never needing spectacles Condition Vivity (%) (N = 24) enVista (%) (N = 27) P value Overall 54.2 18.5 .008 Bright light Distance (far away) 87.5 96.3 .286 Intermediate (at arm's length) 95.8 44.4 .030 Near (up close) 79.2 33.3 .021 Dim light Distance (far away) 87.5 77.8 .051 Intermediate (at arm's length) 87.5 33.3 .018 Near (up close) 58.3 7.4 .001 Proportion of patients reporting “good” or “very good” vision without spectacles Bright light Distance (far away) 95.8 85.2 1.00 Intermediate (at arm's length) 91.7 59.3 .020 Near (up close) 33.3 25.9 .007 Dim light Distance (far away) 70.8 74.1 .456 Intermediate (at arm's length) 83.3 40.7 .009 Near (up close) 41.7 11.1 .019To the authors' knowledge, this is the first study to compare visual outcomes of the Vivity with a monofocal IOL, besides what was performed for the Vivity's U.S. registration trial.8 We felt this worthwhile because of the enVista's different optical profiles (neutral aspheric as opposed to negative aspheric) and anecdotal data from Dee Stephenson reporting some intermediate and near vision with enVista.6 There is also a paucity of literature on the refractive outcomes and visual performance of the enVista monofocal IOL; to our knowledge, only 2 older papers exist.9,10 Furthermore, because Bausch & Lomb, Inc. does not, as of this writing, have a multifocal or EDOF IOL on the market, there has been limited opportunity for their monofocal IOL to act as a comparator in a controlled trial that evaluated intermediate or near vision endpoints. Thus, there is a dearth of literature on the enVista's intermediate and near visual performance.
Refractive outcomes with the Vivity IOL in this study were similar to those obtained in other postmarket approval studies. Herein, the proportion of eyes implanted with Vivity that achieved a residual refractive error of ±0.5 D of emmetropia was 91.7%, whereas in studies by Gundersen et al. and Kohnen et al. those proportions were 90% and 90.6%, respectively.11,12 Refractive outcomes with the enVista IOL in this study were significantly improved compared with those reported in the previous literature. Herein, the proportion of eyes implanted with enVista that achieved a residual refractive error of ±0.5 D of emmetropia was 94.4%, whereas in a study by Heiner et al., this proportion was about 65%.10 We believe this difference is due to (1) the fact that the study by Heiner was conducted over 8 to 10 years ago, before widespread adoption of modern formulas such as Barrett Universal II, and (2) the multicenter study design, leading to greater heterogeneity.
Herein, we have also presented the refractive results of the 2 study IOLs in relation to predicted SE because no prior study has published on this for either IOL. For the Vivity and enVista IOLs, the lane length–adjusted prediction errors were −0.10 ± 0.33 D and −0.03 ± 0.28 D, respectively. This suggests that surgeon-optimized Vivity and enVista IOLs' LFs/A-constants may be closer to 1.84/119.13 and 1.96/119.18, respectively, as calculated using adjustment formulas proposed by Cooke.13 Note that the optimized lens constant for the Vivity IOL in this study is similar to the A-constant proposed on IOLcon.org (119.08), based on clinical data on 211 results.7 The optimized lens constant for the enVista IOL in this study is also very close to the A-constant proposed for use by Graham Barrett on his Barrett Universal II calculator (119.15).14
In this study, both acuity measurements and defocus curve testing showed that the Vivity IOL produced similar distance vision but nearly 2 lines of improvement in intermediate and near when compared with the enVista neutral aspheric monofocal IOL. However, there were some differences in this study when compared with those obtained in the Vivity's U.S. registration trial.5 In patients bilaterally implanted with the Vivity IOL, the binocular CDVA (−0.01 ± 0.10 [≈20/20] vs −0.028 ± 0.084 [≈20/19]) and DCIVA (−0.02 ± 0.13 [≈20/19] vs 0.054 ± 0.093 [≈20/23]) were similar.8 However, the DCNVA was 2 lines of vision better in this study (0.03 ± 0.12 [≈20/21]) than that in the U.S. registration trial (0.253 ± 0.118 [≈20/36]).8 In this study, patients bilaterally implanted with the enVista IOL had a similar CDVA (−0.05 ± 0.07 [≈20/18] vs −0.071 ± 0.086 [≈20/17]) and DCIVA (0.19 ± 0.14 [≈20/31] vs 0.196 ± 0.113 [≈20/31]) to those bilaterally implanted with the Alcon AcrySof SN60WF in the Vivity registration trial. However, the DCNVA (0.17 ± 0.19 [≈20/30] vs 0.391 ± 0.135 [≈20/49]) was 2 lines of vision different. It is plausible that the neutral aspheric profile of the enVista IOL is allowing for the cornea's positive spherical aberration to act unperturbed, thereby creating a small amount of pseudoaccommodation over and above what might be realized with an AcrySof SN60WF IOL (negative aspheric). However, the fact that the Vivity group also had different near acuities in our trial than that reported elsewhere suggests that there may have been differences in how the near testing was completed across trials. Further work is needed, in the form of head-to-head trials comparing the intermediate and near performance of different monofocals, to further elucidate any differences.
Patients implanted with Vivity or enVista IOLs in this study had similar photic phenomena severity profiles to those in the Vivity registration trial (Table 3). There was a slight tendency toward less severe starbursts, halos, and glare with enVista than with the Vivity IOLs. However, these differences were not statistically significant, and our clinical experience has been that patients with either IOL rarely bring up unsolicited concerns such as these. We also found it interesting to compare photic phenomena of the enVista MX60E IOL from this study with those of the AcrySof SN60WF IOL reported in the Vivity registration trial (Supplemental Table 1, https://links.lww.com/JRS/A778). Comparing across studies, patients implanted with the AcrySof SN60WF IOL reported slightly more starbursts and blurred vision. We caution against drawing meaningful conclusions from this though, given the small sample size in this study.
With regard to spectacle independence, a fraction of patients implanted with enVista IOLs reported good uncorrected intermediate vision. These proportions were comparable with those that received the AcrySof SN60WF monofocal IOLs in the Vivity registration trial (Supplemental Table 2, https://links.lww.com/JRS/A778). This is despite the fact that the enVista IOL is known to have a neutral aspheric optic design with a SA of zero, and the AcrySof IOL is known to have a negative aspheric optic design with a SA of approximately −0.20 μm. The key to understanding why these 2 IOLs produce similar intermediate and near vision results despite their differences in optic design has to do with pupil size. The reported values above are based on a pupil size of 6 mm; however, the difference in the SA value between the 2 IOLs over a much smaller pupil, that is, 2 mm or 3 mm, is likely less than 0.1 μm. Thus, differences in aspheric profiles between these monofocal IOLs may not contribute in a clinically meaningful way to depth of focus.
One strength of this study is its prospective double-masked randomized design. On the other hand, the small sample size and the fact that all procedures were performed by a single surgeon and all postoperative visits were performed by a single masked examiner could be considered limitations that stem generalizability. The study's sample size calculation was based on detecting a difference in DCIVA, not patient-reported outcomes from the questionnaires. Therefore, it is possible that the study was not appropriately powered to investigate differences in proportions reported in Tables 3 and 4, which might have been significant in a larger study. Other variables, such as pupil size, can play an important role in pseudoaccommodation but were not studied or controlled for in the present investigation. We also did not investigate relative contrast sensitivity but expect that they would be similar, given the previous work comparing the Vivity with other monofocal IOLs.
Although a fraction of patients will achieve spectacle independence at intermediate with an aspheric monofocal IOL, a more effective way of ensuring such outcomes is to use a light-splitting multifocal/EDOF, or nondiffractive EDOF IOL. The Vivity IOL is one such device that allows for this, all the while with a favorable photopsia profile.WHAT WAS KNOWN The Alcon AcrySof Vivity IOL provides equivalent distance and improved intermediate and near vision when compared with negative aspheric monofocal IOLs. Pseudoaccommodation might be realized when spherical aberration (SA) remains in an optical system. Pairing the cornea's naturally positive SA with a neutral aspheric monofocal IOL might produce such a scenario.
WHAT THIS PAPER ADDS The Alcon AcrySof Vivity IOL provides equivalent distance and nearly 1 to 2 lines of improved intermediate and near vision when compared with a neutral aspheric monofocal IOL (Bausch & Lomb enVista). Patients implanted with the Vivity IOL were twice as likely to report good intermediate vision and nearly 4 times as likely to report good near vision. To the authors' knowledge, this is the first literature to describe the intermediate and near visual performance of Bausch & Lomb enVista monofocal IOLs. A third of these patients reported spectacle independence at near under well-lit conditions. REFERENCES 1. Alió JL, Tavolato M, De la Hoz F, Claramonte P, Rodríguez-Prats JL, Galal A. Near vision restoration with refractive lens exchange and pseudoaccommodating and multifocal refractive and diffractive intraocular lenses: comparative clinical study. J Cataract Refract Surg 2004;30:2494–2503 2. Allen ED, Burton RL, Webber SK, Haaskjold E, Sandvig K, Jyrkkio H, Leite E, Nystrom A, Wollensak J. Comparison of a diffractive bifocal and a monofocal intraocular lens. J Cataract Refract Surg 1996;22:446–451 3. Calladine D, Evans JR, Shah S, Leyland M. Multifocal versus monofocal intraocular lenses after cataract extraction. Cochrane Database Syst Rev 2012:CD003169 4. Courouve L, Cochener B, Lafuma A, Khoshnood B, Berdeaux G. Comparison of outcomes with multifocal intraocular lenses: a meta-analysis. Clin Ophthalmol 2011;5:45–56 5. McCabe C, Berdahl J, Reiser H, Newsom TH, Cibik L, Koch D, Lemp-Hull J, Jasti S. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg 2022;48:1297–1304 6. Stephenson P. Objective and subjective assessment of functional-range-of-vision in patients implanted with aberration-free monofocal IOL. Presented at: ASCRS, San Diego, California, 2019 7. IOL Con: Intraocular Lenses. Available at: http://www.iolcon.org. Accessed July 3, 2022 8. PMA P930014/S126: FDA Summary of Safety and Effectiveness Data. Silver Spring, MD: FDA; 2020 9. Garzón N, Poyales F, de Zárate BO, Ruiz-García JL, Quiroga JA. Evaluation of rotation and visual outcomes after implantation of monofocal and multifocal toric intraocular lenses. J Refract Surg 2015;31:90–97 10. Heiner P, Ligabue E, Fan A, Lam D. Safety and effectiveness of a single-piece hydrophobic acrylic intraocular lens (enVista): results of a European and Asian-Pacific study. Clin Ophthalmol 2014;8:629–635 11. Gundersen KG, Potvin R. Clinical outcomes and quality of vision associated with bilateral implantation of a wavefront shaping presbyopia correcting intraocular lens. Clin Ophthalmol 2021;15:4723–4730
留言 (0)