Patients
This study was a randomized, controlled, and prospective trial. A total of 177 patients scheduled to undergo thoraco-laparoscopic McKeown esophagectomy at the Cancer Center of Sun Yat-Sen University, China, were provided with written information prior to surgery. A total of 168 patients completed the study from February 2020 to December 2021. Written informed consent was obtained on the morning of surgery. Patients were randomly allocated to receive patient-controlled epidural analgesia alone (group PCEA, n = 56), patient controlled intravenous analgesia alone (group PCIA, n = 56), and TPVB combined with TAP and patient-controlled intravenous analgesia (group PVB, n = 56) group with a computer-generated randomization sequence (http://www.randomization.com).
Eligible patients were 18 years of age or older and undergoing thoraco-laparoscopic McKeown esophagectomy. Exclusion criteria were a known contra-indication to either epidural or local anesthetic, inability to give informed consent, open resections, patients with a history of chronic pain issues requiring a regular opioid analgesia sequence with concealed allocation, lack of suitability for single lung ventilation, prior lung surgery, or psychological, family, social factors, and patient refusal that led to an absence of informed consent.
Ethics
Ethical approval for this study (B2019-163) was provided by the Ethics Committee of Cancer Center of Sun Yat-Sen University, Guangzhou City, Guangdong Province, China. The trial was registered in the Chinese Clinical Trial Registry (ChiCTR2000029588, Principal investigator: Renchun Lai, Date of registration: 2020-02-16). The study was in accordance with the Declaration of Helsinki and its later amendments.
Randomization
According to a computer-generated random sequence, once eligibility was confirmed, the patients were randomly assigned in a 1:1:1 ratio into 1 of the 3 groups by using the block randomization method by anesthetists who did not perform the anesthesia protocol for this study. Sequentially numbered, opaque sealed envelopes were used to maintain allocation concealment. Postoperative assessment was performed by the nursing staff who were blinded to the patients’ group.
Analgesic Technique
For the PCEA group, an epidural catheter was inserted between T6 and T9 using a standard technique according to institutional practices. Before the surgical incision was made, 10–20 ml of 0.2% ropivacaine was administered incrementally through the epidural catheter to establish a block. The epidural analgesia regimen for the PCEA group was 0.15% ropivacaine and 0.12 mg/kg morphine with normal saline (NS) to 100 ml, 2 ml/h with a 4-ml bolus, and a lockout time of 60 min.
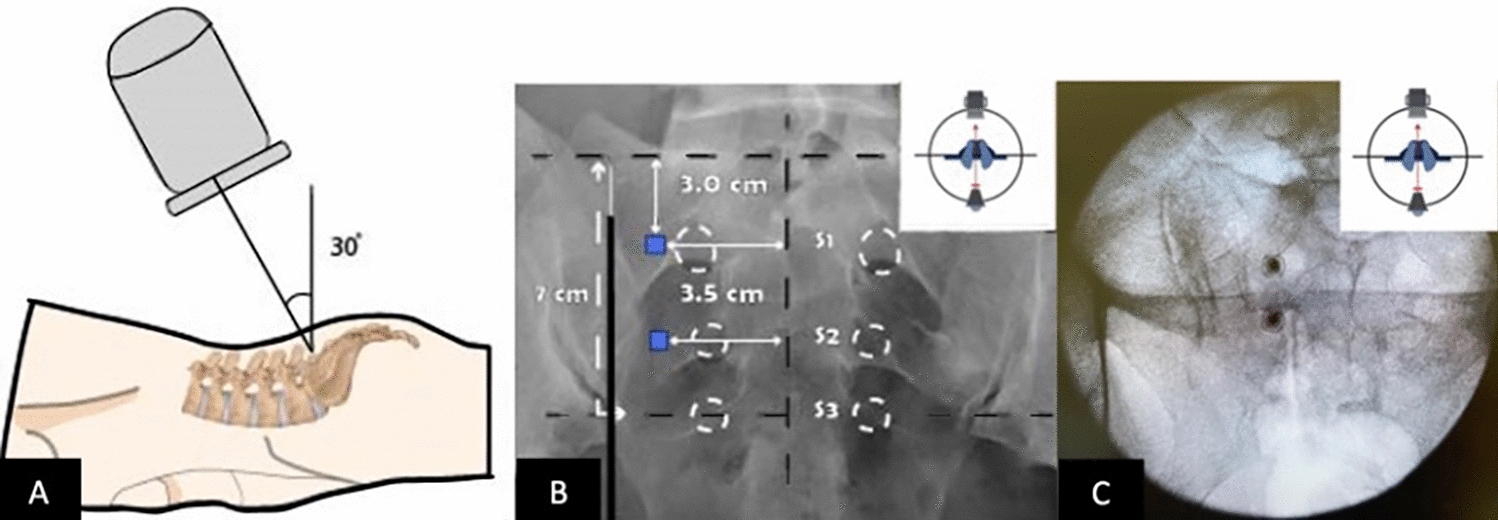
All patients randomized to the PVB group received ultrasound-guided TPVB before the operation. With the patient in a lateral decumbent position and the skin sterilized, we performed T4 and T7 PVB with 0.33% ropivacaine 15 ml at each level, respectively, with a L38 linear ultrasound probe (Sonosite Micromaxx, Bothell, WA, USA) in a sagittal plane from medial to lateral at the mid-thoracic level.
The TAP blocks included both a lateral approach and subcostal TAP blocks placed according to the New York Society of Regional Anesthesia for bilateral TAP blocks [16]. Before the abdominal operation, with patients in the supine position, by using an in-plane approach, a broadband linear array probe (Sonosite Micromaxx) with a frequency of 5–10 MHz was placed in the clavicle midline, a 22-G 100-mm needle was inserted between the internal oblique and the transverse abdominis muscle. After careful negative aspiration, 20 ml of 0.25% ropivacaine was injected into the fascial plane on each side of the abdomen and was observed to spread between the two layers on either side.
Perioperative Care and Anesthesia
All patients received a standard anesthetic by a team of experienced anesthetists. All patients were provided analgesia for 48 h postoperatively. The intravenous analgesia regimen for the PCIA and PVB groups was 100 mg oxycodone with NS to 100 ml, 1 ml/h with a 2-ml bolus, and a lockout time of 5 min. All patients were given oxycodone if they were in pain after removing the analgesic pump.
In all patients, general anesthesia was induced using 0.4–0.5 µg/kg sufentanil, 1.5–2 mg/kg propofol, and 0.2 mg/kg cisatracurium to facilitate endotracheal intubation. Anesthesia was maintained with oxygen and an inhalational agent (sevoflurane/desflurane), cisatracurium, and remifentanil. Patients were monitored by electrocardiogram, pulse oximetry, arterial blood pressure, arterial blood gas, and urethral catheterization. The need for intravenous fluids and vasopressors was determined by the anesthetists.
Patients were transferred from the operating room to the intensive care unit (ICU), where they remained until the criteria for discharge to ward were met. Similarly, patients remained on the ward until the criteria for discharge home were fulfilled.
Outcomes
The primary outcome was the pain score on movement during the first 48 h after surgery. Pain scores were recorded at rest and movement on a visual analogue scale (VAS) from 0 to 10 in the postoperative anesthesia care unit (PACU) and at 24 h, 48 h, 72 h, 96 h, and 120 h postoperatively. Scores were recorded by nursing staff independent from the study. Secondary endpoints were the opioid consumption on 48 h postoperatively, intervention-related side effects (nausea and vomiting), intraoperative blood loss, fluid requirements, need for vasoactive medication, time in operating room and PACU, surgical complications (hemorrhage, stress ulcer, anastomotic fistula, wound infection, recurrent nerve injury, and pulmonary complications), and length of ICU and hospital stay. According to recommendations by the European Perioperative Clinical Outcome Taskforce [17], the presence of postoperative pulmonary complications was defined as the presence of 1 or more of the following criteria: respiratory infection, atelectasis, respiratory failure, pleural effusion, pneumothorax, bronchospasm, or aspiration pneumonitis.
Data Collection
Every patient’s data were prospectively collected in real time. Collected variables included patient demographics, pain scores, perioperative clinical information, and complications. Patient-reported pain assessment began in the PACU by the nursing staff, once a day after the operation, who were unaware of the experimental group .
Statistical Analysis
Based on a review of the literature, we expected a difference in mean VAS score between the intervention groups (the noninferiority limit) of < 1 on a scale from 0 to 10. Previous studies [18,19,20] have suggested that, for a VAS, a difference of 0.9–1.6 cm is clinically significant. Using a power of 80% for the noninferiority test, a significance level of < 5%, and a mean margin in VAS score of 1 (SD 2) [21], we calculated that a sample of 153 patients would be needed. With a supposed dropout rate of 10%, we planned to include 168 patients, 56 in each group. The distribution of each continuous variable was summarized by its mean standard deviation and/or median with range/interquartile range. The distribution of each categorical variable was summarized in terms of its frequency and percentage. Continuous variables which satisfied normal distribution and homogeneity of variance were compared for three treatment groups using Analysis of Variance, and further pairwise comparison was conducted by a least-squares difference test. Shapiro–Wilk tests and Levene tests were used to test for normal distribution and homogeneity of variance, respectively. For variables which do not satisfy normal distribution and homogeneity of variance, Kruskal–Wallis tests were conducted for comparison of the three treatment groups and the further pairwise comparison with Bonferroni correction, and the 95% confidence interval for difference of the median was calculated by the Hodges–Lehman method. For categorical variables, Chi-square test was utilized for comparison of the three treatment groups and Fisher's exact test was used for further pairwise comparison with Bonferroni correction, with the Wilson method used to calculate the difference of rate between the treatment groups. A linear mixed model was used to analyze the effects of different treatment groups, times, and their interactions, and, in the meanwhile, control the effects from confounding factors. We used the Bonferroni method for correcting p values. Statistical analyses were performed using SPSS Statistics 21 (IBM, Armonk, NY, USA). All the tests were two-sided, and the confidence interval was 95%. A bilateral p value of < 0.05 was considered statistically significant.










留言 (0)