
記住我




This single-center case series prospectively included consecutive patients who underwent SO removal from June to December 2019 at Chongqing Aier Eye Hospital. Patients who underwent SO removal combined with phacoemulsification and intraocular lens implantation were included. The inclusion criteria were (1) intravitreal SO tamponade in one eye for primary macula-off rhegmatogenous retinal detachment and normal macular morphology of the attached retina, (2) PVR grade A or B, (3) macular involvement, (4) hole size < 2 PD, (5) best-corrected visual acuity (BCVA) in the eye administered SO tamponade > 0.1 using the international standard visual acuity chart, (6) no SO emulsification, (7) clear media in both eyes, (8) without hypotony, (9) without viral retinitis, and (10) without chronic uveitis. The exclusion criteria were: (1) keratopathy, severe cataract, or diabetic retinopathy, (2) macular edema or hole, (3) giant retinal tear, (4) high myopia or retinal atrophy caused by high myopia, (5) glaucoma, (6) secondary epiretinal membrane (ERM), (7) retinal redetachment during follow-up, (8) optical media opacity overtly interfering with OCT imaging, or (9) pediatric retinal detachment. Patients with suspected drug toxic side effects were not excluded because the causality could not be determined with certainty. Eyes with SO tamponade that met the above criteria were selected as the SO tamponade eye group. Contralateral eyes with BCVA (LogMAR) < 0.1 and OCTA signal strength above 8 were selected as control eyes.
When the current study was first designed, there was no perfluoropropane (C3F8) supply in China, which became available in January 2020, when our hospital began using C3F8. Thus, the patients who underwent pars plana vitrectomy (PPV) and C3F8 gas tamponade from February to June 2020 at Chongqing Aier Eye Hospital were also selected as controls. In order to avoid bias, the same eligibility criteria described above for patients with SO tamponade were applied to patients with C3F8.
The study was performed according to the Declaration of Helsinki. It was approved by the Ethics Committee of Chongqing Aier Eye Hospital (EC approval number: IRB2019009). All participants provided signed informed consent. Clinical trial registration: Registration date: May 22, 2019; Registration number, ChiCTR1900023322; Registration site, Chinese Clinical Trial Registry (ChiCTR).
Surgical proceduresSO removal was performed under retrobulbar anesthesia by associate chief physicians (L.L. and G.W.) using the 23-G Constellation device (Alcon, Fort Worth, TX, USA) and trocars in the inferotemporal and superior quadrants 3.5 mm from the limbus. Infusion liquid was used for oil exchange. An infusion line was inserted into the inferotemporal port, and all the SO was removed using a supratemporal approach with the vacuum set at 450–600 mmHg. Phacoemulsification and intraocular lens implantation through a 2.75-mm micro-coaxial incision were performed when needed (n = 3 patients in the SO group). SO removal was carried out by the pars plana approach upon confirmation of retinal attachment. Following silicone oil removal, the trocars were removed, and the sclerotomies were closed with an 8 − 0 vicryl suture. After SO removal, the patients did not need to follow any position.
Among the 50 patients treated with high-density SO (5000 centistokes, Carl-Zeiss, Germany), three also underwent cataract surgery; none of the patients administered C3F8 were involved. The time taken for surgery was about 30 min. The type of illumination included microscope illumination by an OPMI LUMERA 700 (Carl-Zeiss, Germany) and illumination by the 23-G Constellation device (Alcon, Fort Worth, TX, USA). Postoperative treatment consisted of routine topical antibiotics and anti-inflammatory agents for 1 month. The patients were routinely followed up at 1 day, 7 days, 1 month, and 3 months postoperatively. BCVA, intraocular pressure, OCTA (in the C3F8 group, data on OCTA were recorded after complete disappearance of the gas), and complications were routinely monitored during outpatient visits before and after SO removal.
ExaminationsThe diagnosis of retinal detachment was initially confirmed by slit lamp biomicroscopy and indirect ophthalmoscopy. Perioperative data were obtained from the medical records, including age, sex, axial length, and duration of SO tamponade. BCVA (LogMAR) and intraocular pressure (IOP) in every patient were measured daily during hospitalization. The Lens Opacities Classification III System (LOCS III system) was used to specify cataract classification.
Assessment of visual acuityThe BCVA assessment was performed using an international standard visual acuity chart, and data were transformed into the logarithm of the minimum angle of resolution (LogMAR) units.
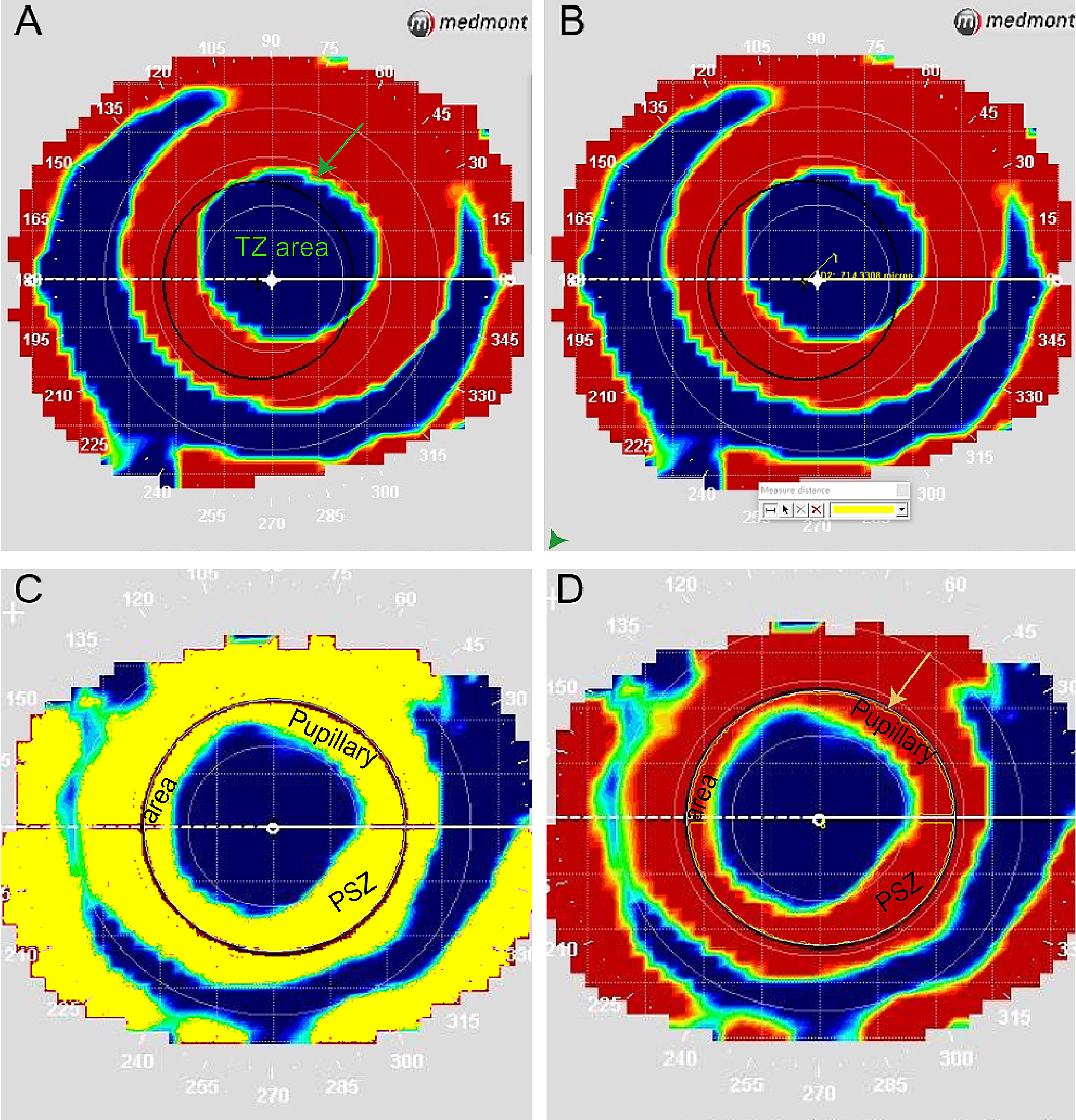
OCTA and analysisIn this study, 6 × 6 mm2 OCTA (Zeiss HD-OCT 5000 with AngioPlex; Carl Zeiss Meditec, Oberkochen, Germany) scans were used for determining SVD and SPD in the macular and peripapillary regions. All scans were obtained by skilled examiners with at least 5 years of OCTA experience and were proficient in conducting OCTA. The SCP comprises the capillaries from the internal limiting membrane (ILM) to the inner plexiform layer (IPL). Scans showing signal strengths > 6 and without motion artifacts or segmentation errors were evaluated [19]. Scan analysis was performed automatically with Cirrus OCTA (AngioPlex 10.0; Carl Zeiss Meditec). VD (in mm− 1) and perfusion density (PD; in % converted to decimals) were assessed as previously reported [20]. PD was defined as the total perfused vasculature per unit area in a measurement region. VD was defined as the total length of perfused vasculature per unit area in a measurement region. SVD and SPD were analyzed in the central region (1-mm diameter circle), inner ring between the 1-mm and 3-mm circles, outer ring between the 3-mm and 6-mm circles, and full area (6-mm diameter circle) (Fig. 1), preoperatively, and at 1 day, 7 days, 1 month, and 3 months after SO removal. OCTA was measured in patients with C3F8 when the C3F8 had completely disappeared.
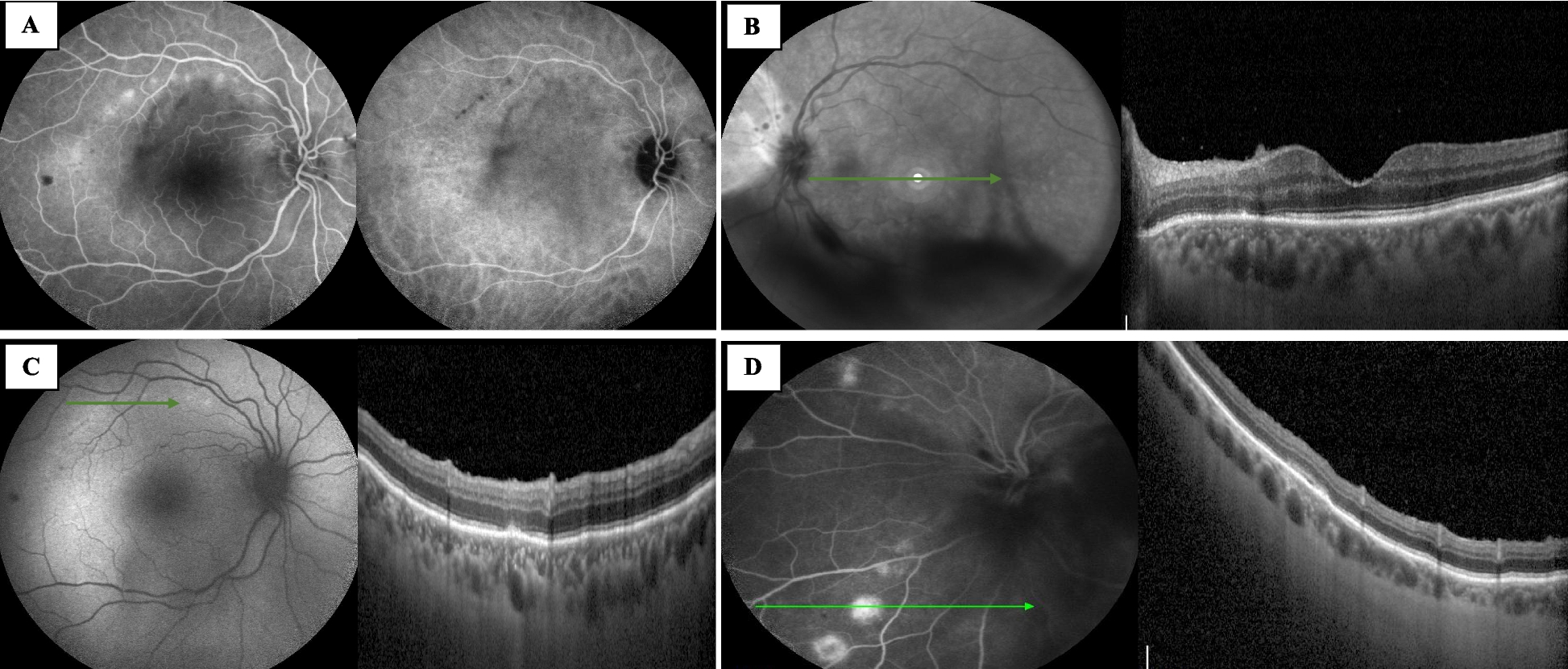
Fig. 1
OCT angiography (OCTA) in a 50-year-old male with an eye administered silicone oil (SO) tamponade. The central area (1-mm diameter central circle), the mean and sector values of the inner ring between the 1-mm and 3-mm diameter circles, the outer ring between the 3-mm and 6-mm diameter circles, and the full area (6-mm diameter outer circles) were assessed. Superficial vessel density (SVD) of the macular and peripapillary regions (A and C) and superficial perfusion density (SPD) of the macular and peripapillary regions (B and D) were automatically determined
Statistical analysisData are shown as means ± standard deviation (SD). Data analysis was performed With SPSS 23.0 (SPSS, USA). One-way analysis of variance (ANOVA) followed by the Bonferroni post hoc test was performed to analyze the differences among multiple independent samples. SVD, SPD and BCVA before and 1 day, 7 days, 1 month, and 3 months after SO removal were compared using repeated measures analysis of variance. Correlations between BCVA and SVD or SPD were assessed using Pearson’s correlation test. P < 0.05 indicated statistical significance.
留言 (0)