
記住我

As important basic data in medicine, age is directly related to decision when surgeons consider the operation. A patient's age can affect the complication and prognosis after surgery, and the patient of elderly often suggests poor surgical outcomes (1, 2). In 2019, 617 million people are 65 years old or older; by 2050, the number will reach 1.6 billion—nearly 20% of the world's population (3). Inevitably, surgeons have to be confronted with the surgical choices of more elderly patients.
Pancreaticoduodenectomy (PD) is still burdened by high rates of complication and mortality (4). The poor outcomes of PD is primarily owing to the highly malignant periampullary neoplasms and the great trauma of operation on human body (5). Considering the potentially higher risks of age-related complication and mortality, the decision to submit elderly to PD would be challenging (6, 7). Early identification of elderly patients, combination of perioperative vigilance and proper treatment may help to reduce the incidence of serious complications and postoperative death. However, how to define the elderly in PD remains controversial. At present, the age group of patients with PD surgery is based on the aging population (8). The criteria for the elderly in some research were the aging criteria of the World Health Organization, such as 65 and 75 years old (9). In another study, regarding the age of 70 as the standard of the elderly is a subjective judgment (9, 10). There is a lack of calculation of the cut-off value of the age of patients with PD (11).
In the present study, we aimed to analyze the effect of age on short-term outcomes in patients undergoing PD and to determine the criteria for the elderly for PD. In particular, it was desired to determine whether differences exist between young and elderly people in postoperative complications and mortality. By calculating the cut-off value of age for PD, the short-term prognosis evaluation effect was calculated, which is helpful for the judgment of PD.
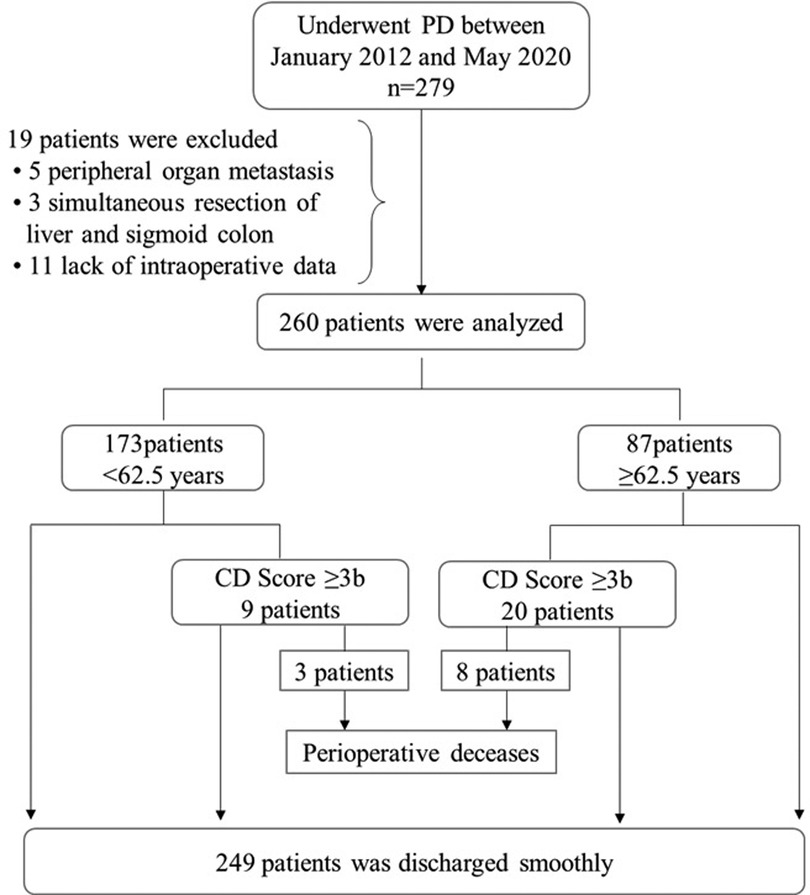
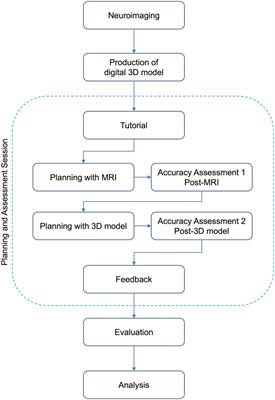
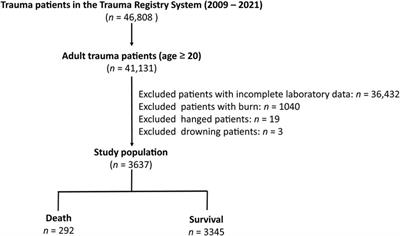
2. Methods 2.1. PatientsThe medical records of all patients who underwent PD in our center between January 2012 and May 2020 were analyzed (n = 279). 19 subjects were excluded because of lack of data or other concomitant procedures (Figure 1). The same surgical team performed all PD using the same procedure, and pathological examination was performed after operation. Age, sex, body mass index (BMI), hypertension, diabetes, hemoglobin, total bilirubin, albumin, complication, re-operation, perioperative mortality (30-day or in-hospital), hospital stay, cost, readmission (90 days of initial discharge), and tumor pathological characteristics were recorded for each participant. The study was approved by the ethics committee of the General Hospital of Western Theater Command and was conducted in accordance with the principles of the Helsinki declaration. The ethical approval number is 2021EC2-26.
Figure 1. Inclusion, exclusion and outcomes of patients. CD Score, Clavien-Dindo Score; PD, Pancreaticoduodenectomy.
2.2. Surgical technique and postoperative managementThe PD was performed by the fixed team, which was composed of five experienced pancreatic surgeons, including at least two attending surgeons. All patients were performed standard Whipple operation for side-to-side gastrojejunal anastomosis, end-to-side biliary jejunal anastomosis and end-to-side pancreatic jejunal anastomosis. The extraperitoneal drainage tube was placed behind the cholangiojejunostomy and pancreaticojejunostomy. Antibiotics were used prophylactically during operation and octreotide was used routinely after operation. The abdominal drainage tube was removed if the amylase level of drainage fluid was normal for three consecutive times after operation.
2.3. Classification of surgical complicationsGrade I: Any deviation from the normal postoperative course without the need for pharmacological treatment orsurgical, endoscopic, and radiological interventions.
Grade Il: Requiring pharmacological treatment with drugs other than such allowed for grade I complicationsBlood transfusions and total parenteral nutrition are also included.
Grade IIl: Requiring surgical,endoscopic or radiological intervention.
Grade IIla: Intervention not under general anesthesia.
Grade IIlb: Intervention under general anesthesia.
Grade IV: Life-threatening complication requiring IC/ICU management.
Grade IVa: Single organ dysfunction (including dialysis).
Grade IVb: Multiorgan dysfunction.
Grade V: Death of a patient.
2.4. Definition of complicationsPostoperative complications were defined as follows, and Clavien-Dindo Score was used to evaluate the postoperative complications (12–15):
Biliary leak: bilious drainage from intraoperatively placed drains or radiographically proven fluid collection requiring percutaneous drainage and demonstrating elevated bilirubin levels.
Postoperative pancreatic fistula (POPF): POPF is now redefined as a drain output of any measurable volume of fluid with an amylase level >3 times the upper limit of institutional normal serum amylase activity three days later after surgery, associated with a clinically relevant development/condition related directly to the postoperative pancreatic fistula.
Chyle leak: Chyle leak was defined as output of milky-colored fluid from a drain, drain site, or wound on or after postoperative day 3, with a triglyceride content ≥110 mg/dl (≥1.2 mmol/L).
Postoperative bleeding: Blood loss proved by various ways, such as hematemesis, hematochezia or melena.
Intraperitoneal infection: Intraperitoneal fluid obtained from percutaneous drainage with culture-proven bacterial organisms.
Delayed gastric emptying: radiological evidence of delayed gastric emptying or post-operative nasogastric tube decompression longer than 2 weeks.
Pulmonary infection: fever, leukocytosis, sputum with leukocytosis, on culture of sputum demonstrating a pathogen, and chest radiograph demonstrating focal infiltrates.
Incision dehiscence: any disruption of the skin closure with subcutaneous tissue exposure or a wound opening that required packing.
Pleural Effusion or Ascites: evidence of fluid collection on postoperative imaging.
Wound infection: Wound infection is defined as findings including purulent discharge, localized swelling, redness/heat, delayed wound healing, or positive wound culture results.
2.5. Statistical analysisWe report the categorical variables as absolute value and percentage value, continuous variables as average ± standard deviation, and asymmetrical distribution (Skewed distribution) continuous variables are presented as median [interquartile range]. A P-Value <0.05 was considered statistically significant. A univariate logistic regression analysis was then performed to identify preoperative variables associated specifically with perioperative complication (Clavien-Dindo Score ≥3b). Variables tested in this analysis included age, sex, BMI, comorbidities (hypertension, diabetes), and laboratory value (hemoglobin, total bilirubin, albumin). Multivariable analyses were carried out in variables with significant differences in univariate logistic analysis. The strength of the association between postoperative complications and age was evaluated by calculating the area under the respective receiver operating characteristic (ROC) curves. This is defined as Y = sensitivity + specificity −1 and ranges from 0 to 1. The dimensional cut-off maximizing the balance between sensitivity and specificity in predicting greater postoperative complications was identified through calculation of the Youden Index, and a cut-off value is picked based on the highest Youden Index. According to the cut-off value, the age groups were divided, and the short-term outcomes which included complications, perioperative deceases, readmission, hospital stay (length of stay after operation), and cost were analyzed. Comparison between the frequencies of the categorical variables (complications, perioperative deceases, readmission,) was assessed using the Chi-square test. The Mann-Whitney U test was used to compare the differences between hospital stay, cost, and in pairs of group. The variables which significant differences in univariate logistic with Clavien-Dindo score were analyzed by ordinal logistic analysis. Calculating the coefficient of regression, the OR value was calculated by SPSS data transformation. All statistical analyses were performed using SPSS version 25.0 software (SPSS Inc. Chicago, IL, United States).
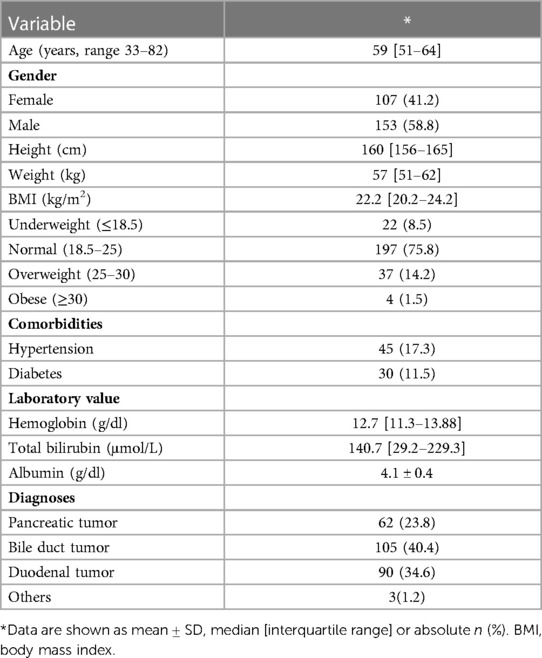
3. Results 3.1. Patient characteristicsPatient characteristics: During the study period, 279 patients underwent PD with the same procedure by the same surgical team. The cases from 19 subjects were excluded from the analysis due to insufficient medical record, and the final index population was composed of 260 subjects. 62 PD were performed for pancreatic tumor, 109 patients underwent PD for bile duct tumor, 90 patients underwent PD for Duodenal tumor, and 3 patients underwent PD for others. The details of these patients are represented in Table 1. Among the continuous variables, only albumin was in normal distribution (average ± standard deviation), and the rest were expressed as median [interquartile range].
Table 1. Patient characteristics (n = 260).
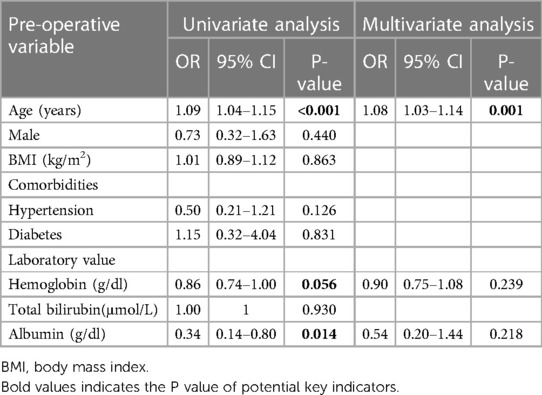
3.2. Univariate and multivariate logistic analysesThe age, sex, BMI, comorbidities (hypertension, diabetes), and laboratory value (hemoglobin, total bilirubin and albumin) were used to evaluate the occurrence of Clavien-Dindo Score ≥3b after operation in univariate logistic regression analysis. Age (OR = 1.09, P = 0.002), hemoglobin (OR = 0.86, P = 0.056) and albumin (OR = 0.34, P = 0.014) were significantly correlated with postoperative complications. Multivariable analyses were carried out in age, hemoglobin, albumin, and patients who evaluated Clavien-Dindo Score ≥3b. Only Age (OR = 1.08, P = 0.01) was significantly correlated with postoperative complications (Table 2).
Table 2. Univariate and multivariate analyses of preoperative predictors associated with the occurrence of Clavien-Dindo Score ≥3b.
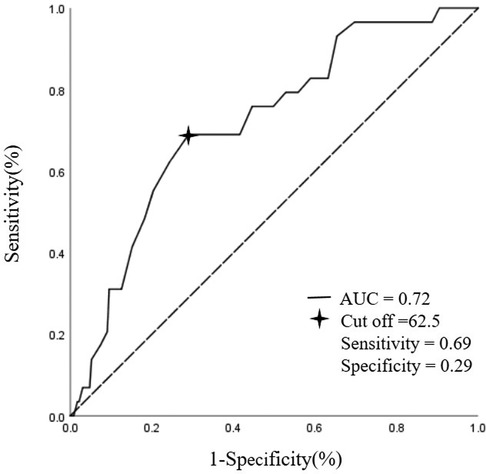
3.3. ROC curve analysisAt ROC curve analysis, age correlated with prediction of Clavien-Dindo Score ≥3b (AUC of 0.71, 95%CI 0.62–0.81, P < 0.001).Point-by point analysis of the ROC curve identified 62.5 years as the cut-off value maximizing the balance of sensitivity and specificity in the prediction of Clavien-Dindo Score ≥3b (Figure 2). According to the cut-off point of 62.5 years old, patients were divided into two groups: group I (<62.5 years) and group II (≥62.5 years). The short-term outcomes (complications, reoperation perioperative deceases, readmission, hospital stay, and cost) were analyzed in Table 3.
Figure 2. Age correlated with prediction of clavien-dindo score ≥3b in ROC curve analysis. AUC, area under curve.
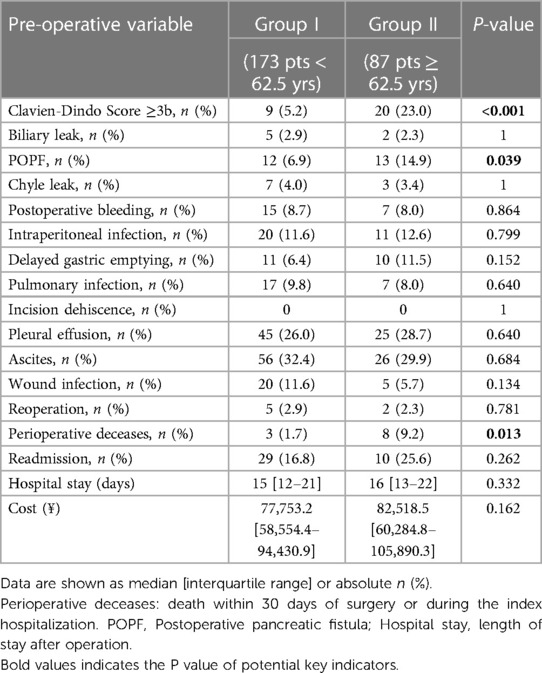
Table 3. Short-term outcomes of two groups who had undergone pancreaticoduodenectomy.
3.4. Short-term outcomes of two groupsThere were 173 (66.5%) patients in group I and 87 (33.5%) in group II. Complications are reported in Table 3: no significant differences were reported for biliary leak, postoperative bleeding, intraperitoneal infection, delayed gastric emptying, pulmonary infection, incision dehiscence, pleural effusion, ascites, wound infection, reoperation, readmission hospital stay, and cost. Perioperative deceases were 11 (4.2%), including 8 (9.2%) from among the group II (P = 0.013). Rates of complications with grade ≥3b, according to the Clavien-Dindo Score, were significantly different between the two groups, as well as incidence of POPF (6.9% in group I vs. 14.9% in group II; P = 0.039).
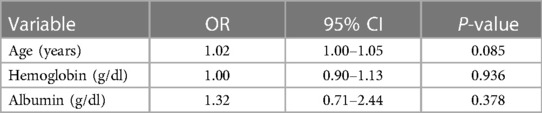
3.5. Ordinal logistic analysisThe age, hemoglobin and albumin that had influence on Clavien-Dindo ≥3b status were included in the preoperative variables, and then the ordinal logistic analysis was used to analyze the influence on the grade of Clavien-Dindo Score (Table 4). It can be seen that age (OR = 1.02, P = 0.085), hemoglobin (OR = 1.00, P = 0.936) and albumin (OR = 1.32, P = 0.378) have no significant effect on the level of Clavien-Dindo Score.
Table 4. Ordinal logistic analysis of predictors of Clavien-Dindo score in patients who underwent PD.
4. DiscussionThe world's population is aging rapidly. In parallel, the rate of neoplastic diseases and the number of surgical operations is rising steeply. Despite the poor outcomes, PD is the best choice for the treatment of periampullary neoplasms. The high risk of outcomes are mainly owing to the high postoperative morbidity and mortality rates. Consequently, careful selection before surgery is the key to excellent outcomes. The top factor which attracts the attention of surgeons was age, and the advanced age of patients tends to be closely related to higher postoperative complications. However, the definition of the “old patient” in terms of age varies across the studies is not worldwide accepted and different age cut-off, such as 65, 70, 75, and 80 years have been used in the studies of PD (3, 16).There is a lack of age grouping based on postoperative complications of PD. As an operation with huge trauma, defining the cut-off of elderly patients in PD can be conducive to predicting poor prognosis.
In the present study, we calculated the influence of preoperative and pathological data of 260 PD patients on Clavien-Dindo ≥3b status. In univariate logistic regression analysis, age, hemoglobin and albumin had significant effect on Clavien-Dindo ≥3b status. Age (OR = 1.09, P = 0.002) is a risk factor for postoperative complications, while hemoglobin (OR = 0.86, P = 0.056) and albumin (OR = 0.34, P = 0.014) are protective factors. Nutritional status before surgery is regarded as one of the key factors that influence outcomes after operation, several studies on PD have indicated the importance of maintaining normal preoperative albumin levels (17, 18). Subsequent multivariate logistic regression analysis showed that age was significantly correlated with prognosis (OR = 1.08, P = 0.01). Consistent with other studies, old age is an independent risk factor for complications after PD, but there is no clear cut-off point for the division of age. At ROC curve analysis, age correlated with Clavien-Dindo ≥3b status (AUC = 0.72, cut-off = 62.5). Sensitivity, and specificity of possible cut-offs for age are displayed in Figure 2. This is different from the cut-off value of aging in developed countries (65 years), which may be due to the consumption of body by malignant tumor and the larger injury of PD (19–21).
Although elderly patients were not the absolute contraindication of PD, the incidence rate of postoperative complications was higher in elderly patients. In our research, the patients were divided into two groups according to 62.5 years old: group I (<62.5 years) and group II (≥62.5 years). The short-term outcomes (complications, perioperative deceases, readmission, hospital stay, and cost) were analyzed. Among the complications, only Clavien-Dindo >3b status (5.2% in group I vs. 23.0% in group II; P < 0.001) and POPF (6.9% in group I vs. 14.9% in group II; P = 0.039) had significant differences between the two groups, and the incidence rate of the second group was significantly higher than that of the first group. The Clavien-Dindo grade and POPF showed the same trend because the main complication requiring intervention after PD was pancreatic fistula and the pancreatic anastomosis carries the highest risk of leak and cause of morbidity and mortality (22, 23). Elderly patients were prone to POPF for the following reasons: firstly, elderly patients were complicated with more basic diseases, and anastomotic edema was vulnerable to cause POPF; Second, postoperative infection increased the incidence of pancreatic fistula because of poor immunity; Third, weak physical conditions were often not conducive to the recovery of anastomotic stoma, resulting in anastomotic failure. Due to the high incidence rate of POPF and the weakness of the elderly, the perioperative mortality of the group I was significantly higher than the group II (1.7% in group I vs. 9.2% in group II; P = 0.013).
In terms of postoperative management, there were no significant difference in reoperation readmission, hospital stay and cost. The ordinal logistic analysis was used to analyze age (OR = 1.02, P = 0.085), hemoglobin (OR = 1.00, P = 0.936) and albumin (OR = 1.32, P = 0.378) on the grade of Clavien-Dindo Score, while all of them had no significant effect on this grade. We speculate that the number of high-grade of Clavien-Dindo Score is less leading to unclear judgment.
With the development of surgical technology and neoadjuvant therapy, the elderly have no longer been the forbidden area of PD surgery (7, 24, 25). However, compared with the young, the postoperative complications and mortality of the elderly have significantly increased (26, 27). Elderly patients were more likely to develop POPF and Clavien-Dindo Score ≥3b than younger ones, probably as a result of the poor recovery of pancreaticojejunostomy, frailty, and the decrease of physical tolerance in the elderly (28–30). Our research further supports the above view.
The difference is that the age group used in our study is not the commonly used 65 year old age limit in developed countries, or 75 and 80 years old in other PD prognosis studies, but the best cut-off value of 62.5 years old selected after calculating the dimensional cut-off maximizing the balance between sensitivity and specificity by analyzing the characteristics of PD patients in our hospital. Surgeons can refer to this cut-off value before making surgical decisions, and be vigilant for elderly patients to reduce postoperative complications.
The main limitation of this study is the retrospective nature and the resulting selection bias, because the cases extracted from our center were used to represent the analyzed population. Additionally, due to the difficulty of long-term follow-up, we cannot collect the long-term outcomes after PD. Therefore, further multicenter prospective studies or basic research will be needed to understand the influence of age on the short-term and long-term outcomes of PD patients.
In conclusions, age, hemoglobin and albumin were significantly correlated with postoperative Clavien-Dindo Score ≥3b in preoperative variables. According to 260 cases in our center, the cut-off value of elderly patients with PD was 62.5 years old and there were significant differences in postoperative Clavien-Dindo Score ≥3b, pancreatic fistula, and perioperative death between the elderly and young group. However, age, hemoglobin and albumin were no significant differences in predicting the grade of Clavien-Dindo Score.
Data availability statementThe original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statementThe studies involving human participants were reviewed and approved by the ethics committee of General Hospital of Western Theater Command. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributionsZZ: Conceptualization; data curation; formal analysis; writing–original draft; writing—review and editing. ZS: Data curation; formal analysis; investigation; project administration; writing—review and editing. TY: Data curation; writing—review and editing; formal analysis. ZL: software; writing—original draft; writing—review and editing. JH: Conceptualization; formal analysis; methodology; writing—review and editing. TZ: Conceptualization; formal analysis; methodology; writing—review and editing. DR: project administration; resources; writing—original draft; writing—review and editing. All authors contributed to the article and approved the submitted version.
FundingThis work was supported by the Management of the General Hospital of Western Theater Command (2021-XZYG-B16), the key research and development program of Sichuan Provincial Science and Technology Department (2022YFS0195), and Pancreatic injury and repair Key laboratory of Sichuan Province (Grant no. 41732152).
Conflict of interestThe authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's noteAll claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References2. Pearse RM, Harrison DA, James P, Watson D, Hinds C, Rhodes A, et al. Identification and characterisation of the high-risk surgical population in the United Kingdom. Crit Care. (2006) 10(3):R81. doi: 10.1186/cc4928
PubMed Abstract | CrossRef Full Text | Google Scholar
3. Dzau VJ, Inouye SK, Rowe JW, Finkelman E, Yamada T. Enabling healthful aging for all—the national academy of medicine grand challenge in healthy longevity. N Engl J Med. (2019) 381(18):1699–701. doi: 10.1056/NEJMp1912298
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Paiella S, De Pastena M, Pollini T, Zancan G, Ciprani D, De Marchi G, et al. Pancreaticoduodenectomy in patients ≥75 years of age: are there any differences with other age ranges in oncological and surgical outcomes? Results from a tertiary referral center. World J Gastroenterol. (2017) 23(17):3077–83. doi: 10.3748/wjg.v23.i17.3077
PubMed Abstract | CrossRef Full Text | Google Scholar
5. Oh HM, Yoon YS, Han HS, Kim JH, Cho JY, Hwang DW. Risk factors for pancreatogenic diabetes after pancreaticoduodenectomy. Korean J Hepatobiliary Pancreat Surg. (2012) 16(4):167–71. doi: 10.14701/kjhbps.2012.16.4.167
PubMed Abstract | CrossRef Full Text | Google Scholar
6. Sukharamwala P, Thoens J, Szuchmacher M, Smith J, DeVito P. Advanced age is a risk factor for post-operative complications and mortality after a pancreaticoduodenectomy: a meta-analysis and systematic review. HPB. (2012) 14(10):649–57. doi: 10.1111/j.1477-2574.2012.00506.x
PubMed Abstract | CrossRef Full Text | Google Scholar
7. Khan S, Sclabas G, Lombardo KR, Sarr MG, Nagorney D, Kendrick ML, et al. Pancreatoduodenectomy for ductal adenocarcinoma in the very elderly; is it safe and justified? J Gastrointest Surg. (2010) 14(11):1826–31. doi: 10.1007/s11605-010-1294-8
PubMed Abstract | CrossRef Full Text | Google Scholar
8. Scurtu R, Bachellier P, Oussoultzoglou E, Rosso E, Maroni R, Jaeck D. Outcome after pancreaticoduodenectomy for cancer in elderly patients. J Gastrointest Surg. (2006) 10(6):813–22. doi: 10.1016/j.gassur.2005.12.010
PubMed Abstract | CrossRef Full Text | Google Scholar
9. Barbas AS, Turley RS, Ceppa EP, Reddy SK, Blazer DG 3rd, Clary BM, et al. Comparison of outcomes and the use of multimodality therapy in young and elderly people undergoing surgical resection of pancreatic cancer. J Am Geriatr Soc. (2012) 60(2):344–50. doi: 10.1111/j.1532-5415.2011.03785.x
PubMed Abstract | CrossRef Full Text | Google Scholar
10. Faraj W, Alameddine R, Mukherji D, Musallam K, Haydar A, Eloubiedi M, et al. Postoperative outcomes following pancreaticoduodenectomy: how should age affect clinical practice? World J Surg Oncol. (2013) 11:131. doi: 10.1186/1477-7819-11-131
PubMed Abstract | CrossRef Full Text | Google Scholar
11. Gruppo M, Tolin F, Franzato B, Pilati P, Spolverato YC, Zingales F, et al. Impact of age on short- and long-term outcomes after pancreatoduodenectomy for periampullary neoplasms. Gastroenterol Res Pract. (2020) 2020:1793051. doi: 10.1155/2020/1793051
PubMed Abstract | CrossRef Full Text | Google Scholar
12. Besselink MG, van Rijssen LB, Bassi C, Dervenis C, Montorsi M, Adham M, et al. Definition and classification of chyle leak after pancreatic operation: a consensus statement by the international study group on pancreatic surgery. Surgery. (2017) 161(2):365–72. doi: 10.1016/j.surg.2016.06.058
PubMed Abstract | CrossRef Full Text | Google Scholar
13. Bassi C, Marchegiani G, Dervenis C, Sarr M, Abu Hilal M, Adham M, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. (2017) 161(3):584–91. doi: 10.1016/j.surg.2016.11.014
PubMed Abstract | CrossRef Full Text | Google Scholar
14. Panwar R, Pal S. The International Study Group of Pancreatic Surgery definition of delayed gastric emptying and the effects of various surgical modifications on the occurrence of delayed gastric emptying after pancreatoduodenectomy. Hepatobiliary Pancreat Dis Int. (2017) 16(4):353–63. doi: 10.1016/S1499-3872(17)60037-7
PubMed Abstract | CrossRef Full Text | Google Scholar
15. Gagnière J, Le Roy B, Veziant J, Pereira B, Narayan RR, Pezet D, et al. Pancreaticoduodenectomy with right gastric vessels preservation: impact on intraoperative and postoperative outcomes. ANZ J Surg. (2019) 89(4):E147–52. doi: 10.1111/ans.14956
CrossRef Full Text | Google Scholar
16. Noba L, Rodgers S, Chandler C, Balfour A, Hariharan D, Yip VS. Enhanced recovery after surgery (ERAS) reduces hospital costs and improve clinical outcomes in liver surgery: a systematic review and meta-analysis. J Gastrointest Surg. (2020) 24(4):918–32. doi: 10.1007/s11605-019-04499-0
PubMed Abstract | CrossRef Full Text | Google Scholar
17. Thomas MN, Kufeldt J, Kisser U, Hornung HM, Hoffmann J, Andraschko M, et al. Effects of malnutrition on complication rates, length of hospital stay, and revenue in elective surgical patients in the G-DRG-system. Nutrition (Burbank, Los Angeles County, Calif). (2016) 32(2):249–54. doi: 10.1016/j.nut.2015.08.021
PubMed Abstract | CrossRef Full Text | Google Scholar
18. Novelli IR, Araújo BAD, Grandisoli LF, Furtado ECG, Aguchiku EKN, Bertocco MCG, et al. Nutritional counseling protocol for colorectal cancer patients after surgery improves outcome. Nutr Cancer. (2021) 73(11–12):2278–86. doi: 10.1080/01635581.2020.1819345
PubMed Abstract | CrossRef Full Text | Google Scholar
19. Lobo V, Patil A, Phatak A, Chandra N. Free radicals, antioxidants and functional foods: impact on human health. Pharmacogn Rev. (2010) 4(8):118–26. doi: 10.4103/0973-7847.70902
PubMed Abstract | CrossRef Full Text | Google Scholar
21. Ye H, Adane B, Khan N, Alexeev E, Nusbacher N, Minhajuddin M, et al. Subversion of systemic glucose metabolism as a mechanism to support the growth of leukemia cells. Cancer Cell. (2018) 34(4):659–73.e6. doi: 10.1016/j.ccell.2018.08.016
PubMed Abstract | CrossRef Full Text | Google Scholar
22. Takano S, Ito Y, Watanabe Y, Yokoyama T, Kubota N, Iwai S. Pancreaticojejunostomy versus pancreaticogastrostomy in reconstruction following pancreaticoduodenectomy. Br J Surg. (2000) 87(4):423–7. doi: 10.1046/j.1365-2168.2000.01395.x
PubMed Abstract | CrossRef Full Text | Google Scholar
23. Frigerio I, Bannone E, Trojan D, Montagner G, Bergamaschi G, Butturini G. Implantation of amniotic membrane over pancreatic anastomosis after pancreaticoduodenectomy: report of the first case. J Surg Case Rep. (2019) 2019(5):rjz097. doi: 10.1093/jscr/rjz097
PubMed Abstract | CrossRef Full Text | Google Scholar
24. Tani M, Kawai M, Hirono S, Ina S, Miyazawa M, Nishioka R, et al. A pancreaticoduodenectomy is acceptable for periampullary tumors in the elderly, even in patients over 80 years of age. J Hepatobiliary Pancreat Surg. (2009) 16(5):675–80. doi: 10.1007/s00534-009-0106-6
PubMed Abstract | CrossRef Full Text | Google Scholar
25. Kow AW, Sadayan NA, Ernest A, Wang B, Chan CY, Ho CK, et al. Is pancreaticoduodenectomy justified in elderly patients? Surgeon. (2012) 10(3):128–36. doi: 10.1016/j.surge.2011.02.005
PubMed Abstract | CrossRef Full Text | Google Scholar
26. Lu Q, Lu JW, Wu Z, Liu XM, Li JH, Dong J, et al. Perioperative outcome of elderly versus younger patients undergoing major hepatic or pancreatic surgery. Clin Interv Aging. (2018) 13:133–41. doi: 10.2147/CIA.S153058
PubMed Abstract | CrossRef Full Text | Google Scholar
27. van der Geest LG, Besselink MG, van Gestel YR, Busch OR, de Hingh IH, de Jong KP, et al. Pancreatic cancer surgery in elderly patients: balancing between short-term harm and long-term benefit. A population-based study in The Netherlands. Acta Oncol. (2016) 55(3):278–85. doi: 10.3109/0284186X.2015.1105381
PubMed Abstract | CrossRef Full Text | Google Scholar
28. Brahmbhatt B, Bhurwal A, Lukens FJ, Buchanan MA, Stauffer JA, Asbun HJ. Pancreatic surgery in the older population: a single institution's experience over two decades. Curr Gerontol Geriatr Res. (2016) 2016:8052175. doi: 10.1155/2016/8052175
PubMed Abstract | CrossRef Full Text | Google Scholar
30. Bagshaw SM, Stelfox HT, McDermid RC, Rolfson DB, Tsuyuki RT, Baig N, et al. Association between frailty and short- and long-term outcomes among critically ill patients: a multicentre prospective cohort study. CMAJ. (2014) 186(2):E95–102. doi: 10.1503/cmaj.130639
留言 (0)