
記住我
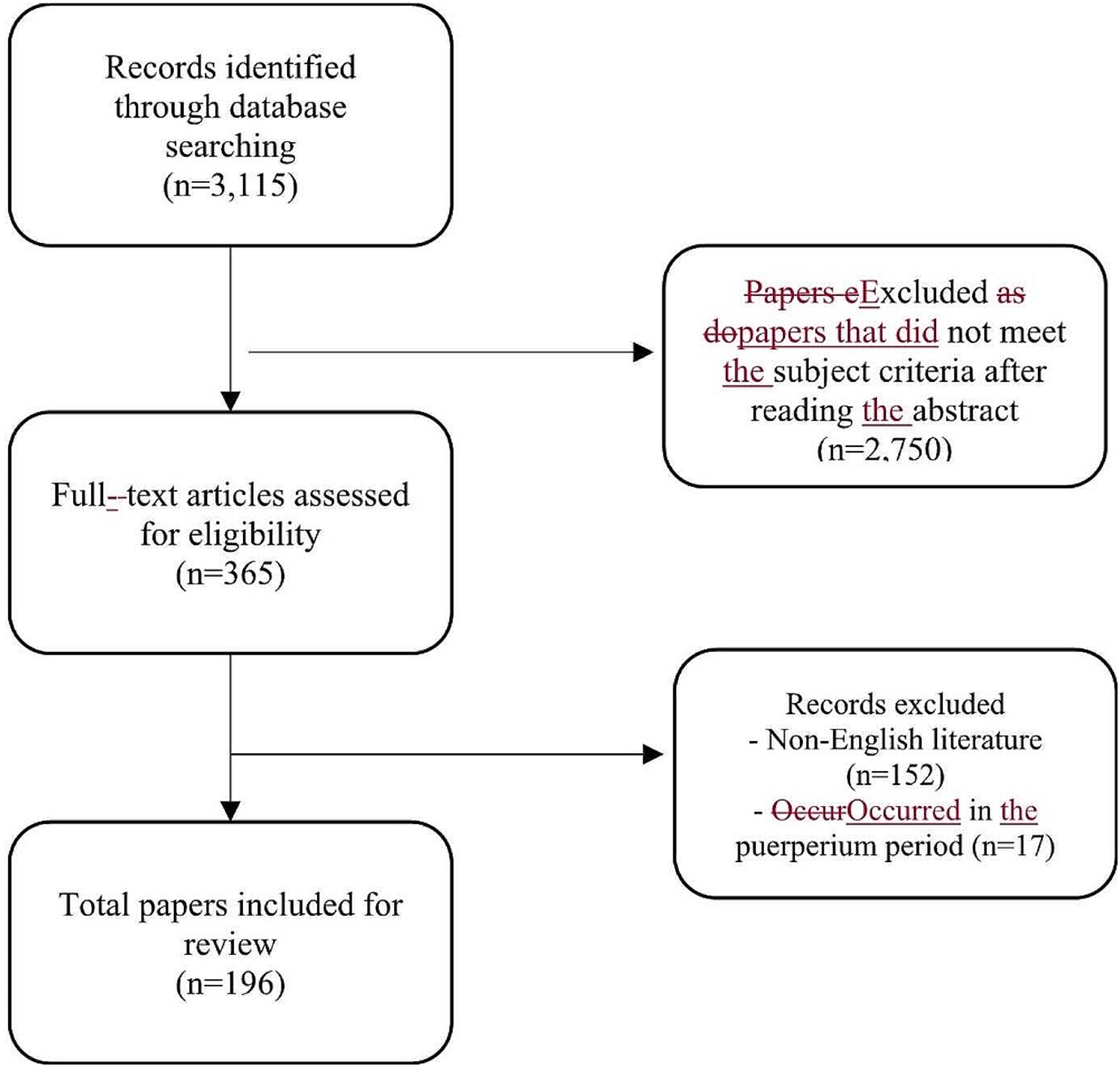
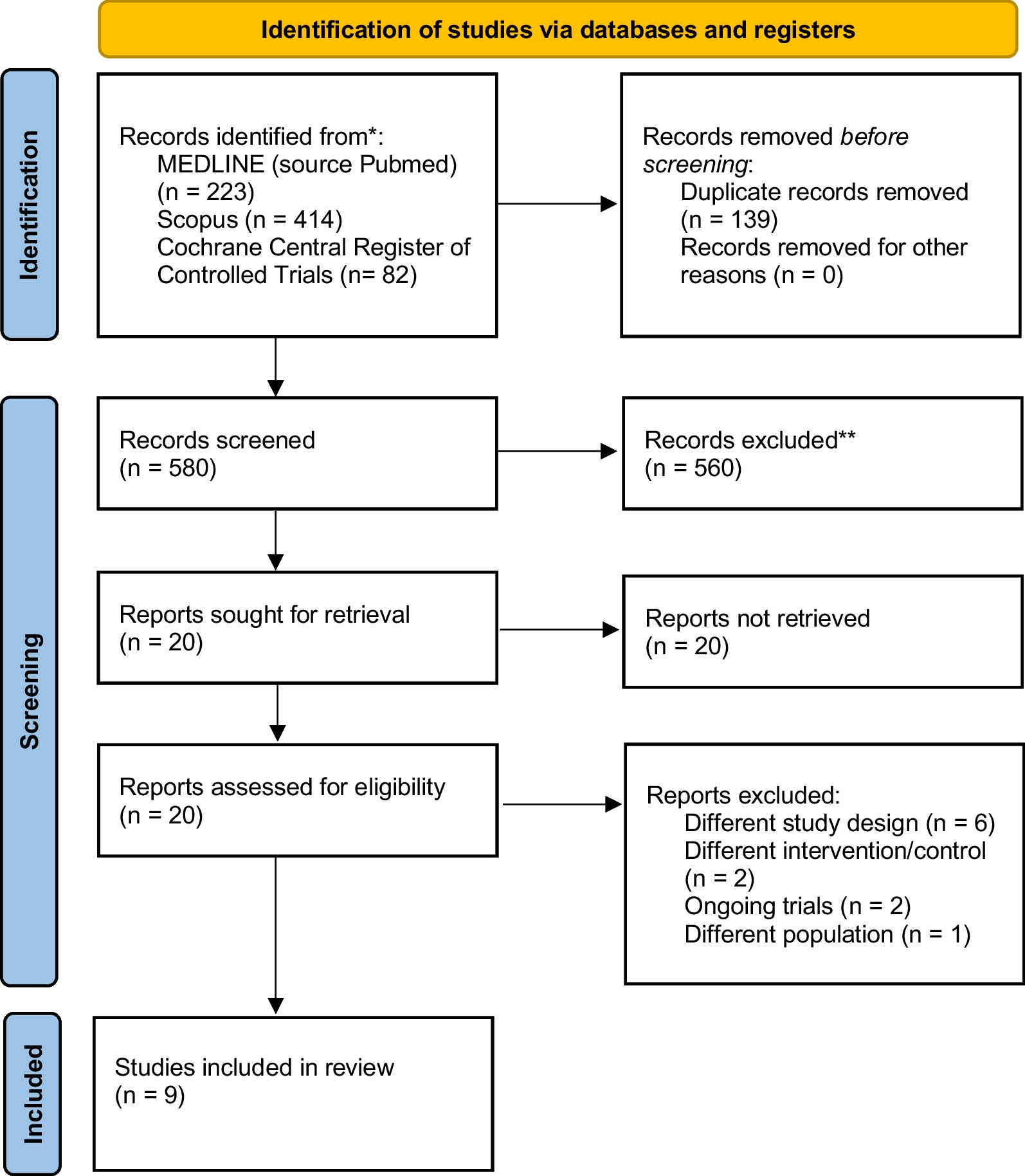


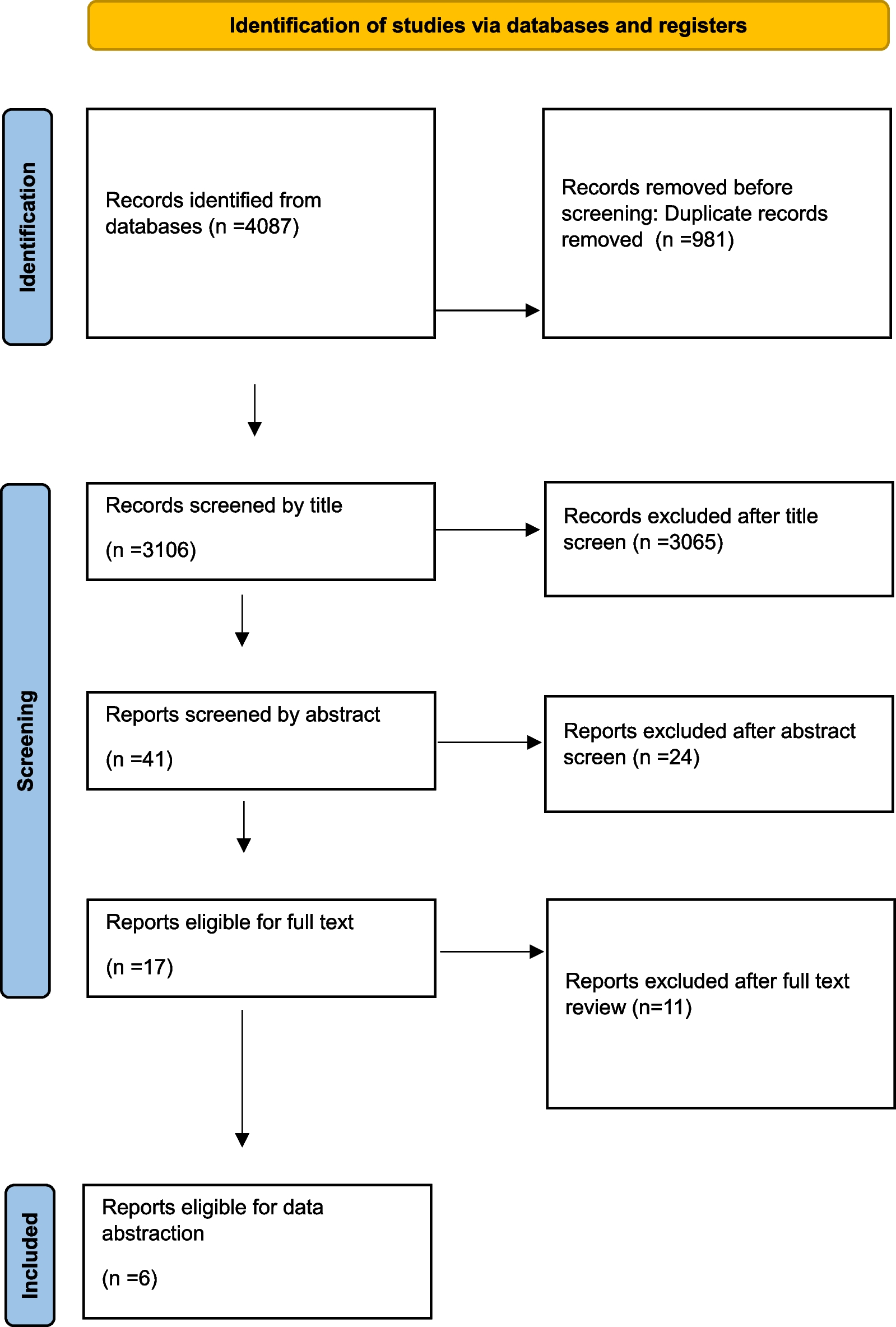
A literature search identified a total of 2349 studies, of which 1508 were removed due to duplication or overlap. An additional 750 studies were excluded after screening titles and abstracts, leaving 91 full-text studies. Of these, 68 studies that did not meet the inclusion criteria were excluded, leaving 23 studies that were eligible for inclusion in the review. Figure 1 shows a flow chart illustrating the process of selecting publications for inclusion.
Fig. 1
Flow chart of the selection of publications included in the meta-analysis
Quality assessmentThe Newcastle–Ottawa quality assessment scale was used to evaluate the quality of the evidence. According to this scale, all of the selected studies received at least 5 stars, indicating a low to moderate risk of bias (Table 1).
Table 1 Newcastle-Ottawa Scale for risk of bias assessment of studies included in the meta-analysisCharacteristics of eligible studiesAll 23 studies [3, 7, 19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39] included were retrospective studies with a total of 49,152 patients, and 1448 patients were treated HBO, versus 47,704 patients treated without HBO. Ten studies came from North America (8 from USA, 2 from Canada). Six studies came from Europe (2 from Germany, 2 from Italy, 2 from Denmark). Four studies came from Asia (1 from China, 1 from Taiwan, 1 from Singapore, and 1 from Israel). Two studies came from South America (Brazil), and only 1 study came from Oceania (Australia). 65.2% of the patients were males. The body regions infected varied among the studies, and the major body regions affected were head and neck, truncal, perianal, anorectal, perineal and genital areas. The primary outcome included the mortality rate. The secondary outcomes included the amputation rate, the number of debridement and complications. The complications in this meta-analysis were sepsis, shock, myocardial infarction, pulmonary embolism, pneumonia and MODS. The characteristics of the included studies are summarized in Table 2.
Table 2 Characteristics of the studies and patients included in the meta-analysisEvidence synthesisPrimary outcomesAs the primary outcome, the mortality rate was reported in all included studies. The mean mortality rate in the HBO group was 10.6% [95% CI (6.7, 14.5)] and the mean mortality rate in the non-HBO group was 25.6% [95% CI (19.5, 31.7)]. The study found that the mortality rate in the HBO group was significantly lower than that in the non-HBO group [RR = 0.522, 95% CI (0.403, 0.677), p < 0.05] (Fig. 2).
Fig. 2
Forest plot of the mortality rate
Secondary outcomesThe number of debridements was reported in 8 studies [3, 7, 23, 25, 29, 31, 37, 38]. The study found that the number of debridements in the HBO group was higher than in the non-HBO group [SMD = 0.611, 95% CI (0.012, 1.211), p < 0.05] (Fig. 3).
Fig. 3
Forest plot of the number of debridement
The amputation rate was reported in 6 studies [3, 23, 27,28,29, 34]. The study found no statistical significance in the amputation rate between the HBO group and non-HBO group [RR = 0.836, 95% CI (0.619, 1.129), p > 0.05] (Fig. 4).
Fig. 4
Forest plot of the amputation rate
Complications were reported in 5 studies [3, 7, 22, 27, 33], including sepsis, shock, myocardial infarction, pulmonary embolism, pneumonia, and MODS. Data on the incidence of MODS was available for analysis from 2 studies [27, 33]. The study found that the incidence of MODS in the HBO group was lower than in the non-HBO group [RR = 0.205, 95% CI (0.164, 0.256), p < 0.05]. However, there was no statistical significance in the incidence of other complications, such as sepsis, shock, myocardial infarction, pulmonary embolism, and pneumonia, between the two groups (p > 0.05) (Fig. 5).
Fig. 5
Forest plot of the incidences of complications
Subgroup analysesWe did a subgroup analysis with pathological entity into two categories: FG subgroup and Non-FG subgroup. The FG subgroup consisted of 10 studies [7, 19,20,21, 24, 25, 30, 33, 35, 36]. The Non-FG consisted of 13 studies [3, 22, 23, 26,27,28,29, 31, 32, 34, 37,38,39]. The mortality rate was significantly lower in the HBO group compared to the non-HBO group in both non-FG [RR = 0.580, 95% CI (0.436, 0.770), p < 0.05] and FG subgroups [RR = 0.389, 95% CI (0.209, 0.723), p < 0.05]. The number of debridements in the HBO group was higher than in the non-HBO group [SMD = 0.614, 95% CI (0.453, 0.775), p < 0.05] in the non-FG subgroup, while there was no statistical significance of the number of debridements between the HBO group and non-HBO group [SMD = 0.340, 95% CI (− 3.032, 3.712), p > 0.05] in the FG subgroup. There was no statistical significance in the incidence rate of sepsis between the HBO group and non-HBO group [RR = 0.800, 95% CI (0.304, 2.108), p > 0.05] in the non-FG subgroup, as well as in the FG subgroup [RR = 1.319, 95% CI (0.943, 1.843), p > 0.05]. (Table 3). The forest plots of subgroup analyses are showed in Additional file 4.
Table 3 Subgroup analysis with pathological entity into two categoriesPublication biasThe funnel plot did not show significant publication bias for the mortality rate (p = 0.086). The funnel plot is shown in Fig. 6.
Fig. 6
Funnel plot assessing publication bias based on the mortalityrate
Evidence certaintyThe GRADE level of evidence is very low for mortality rate, amputation rate, very low for number of debridement. GRADE evidence certainty for the outcomes is shown in Table 4.
Table 4 GRADE evidence certainty
留言 (0)