
記住我
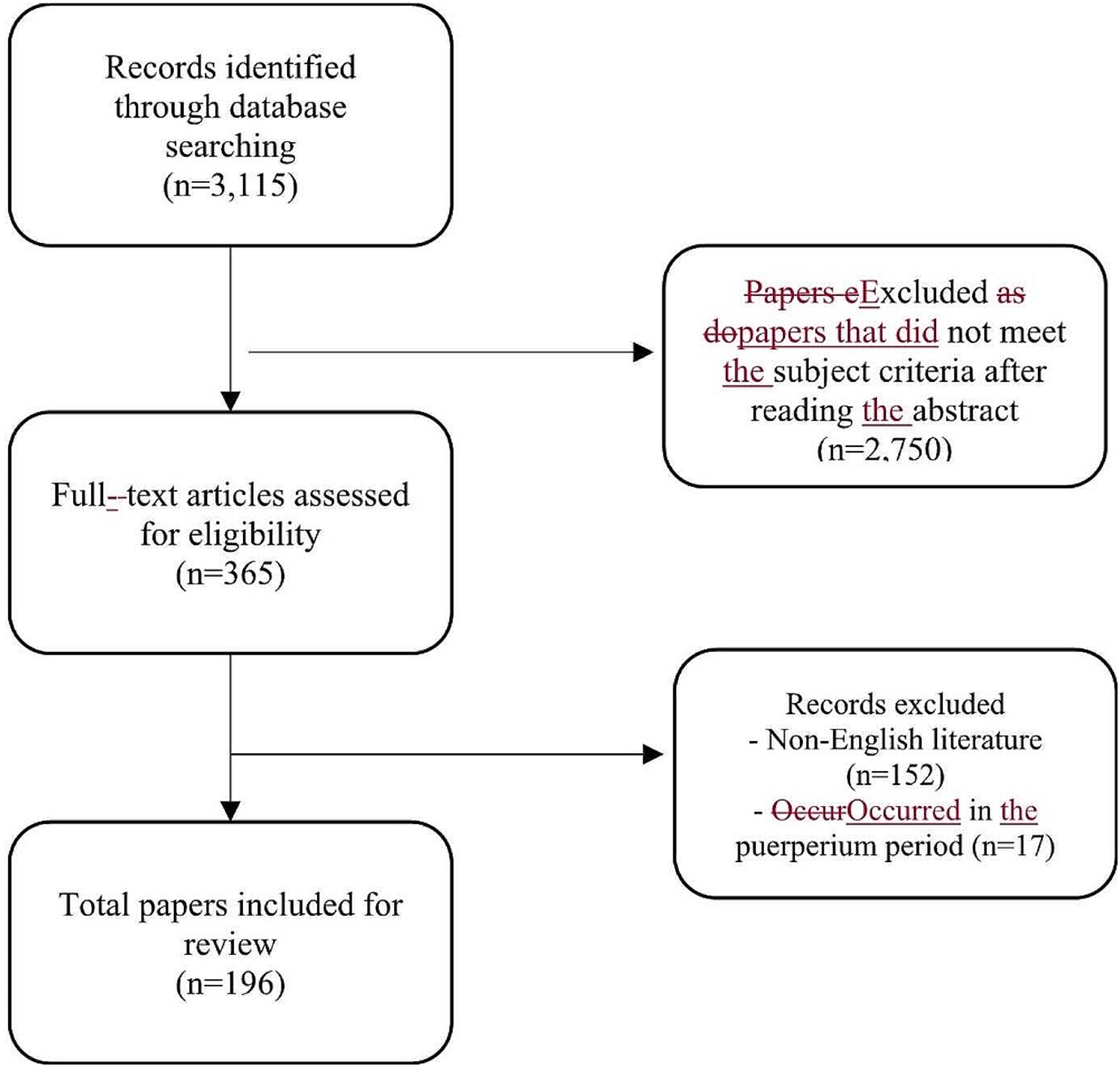
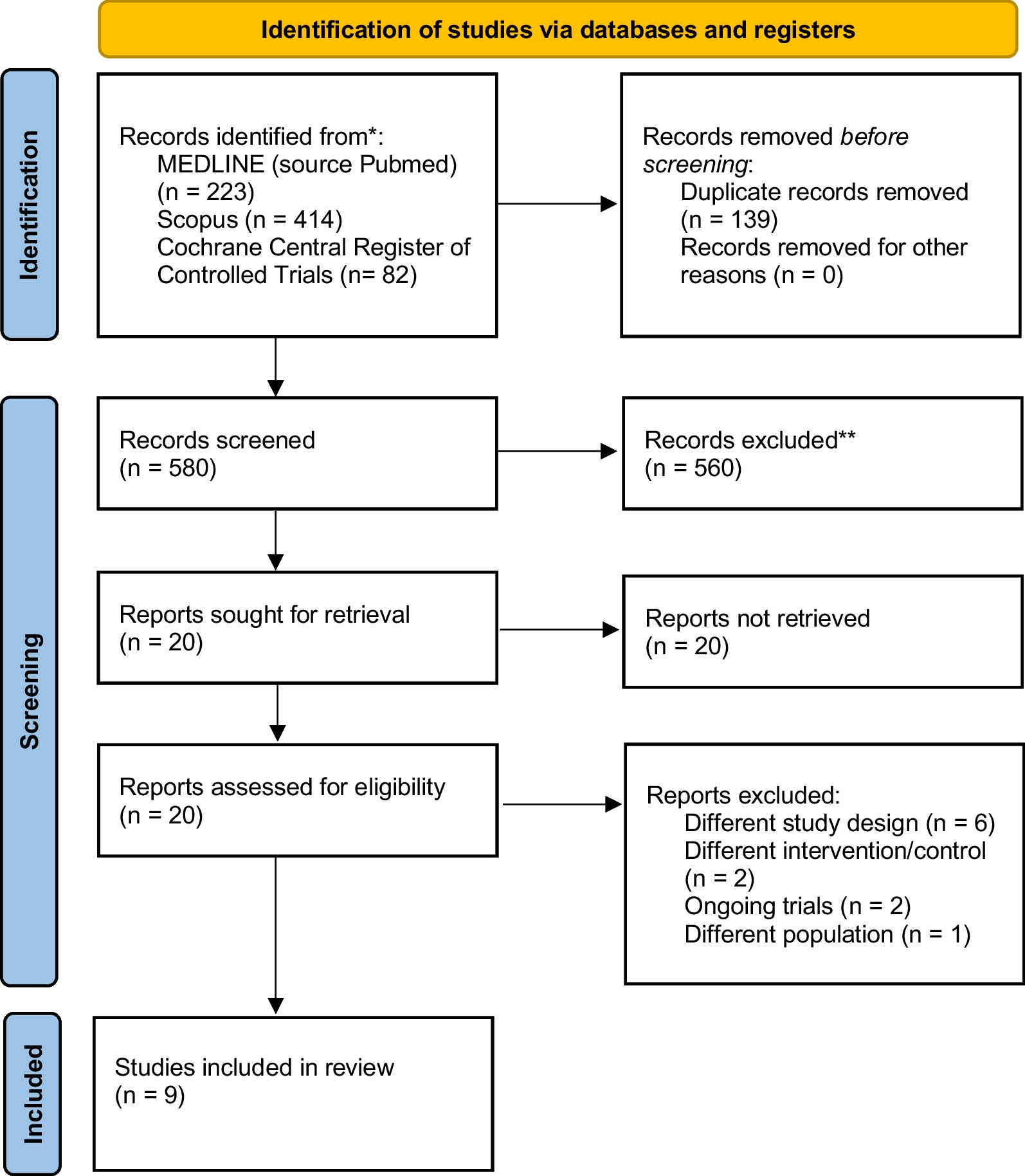


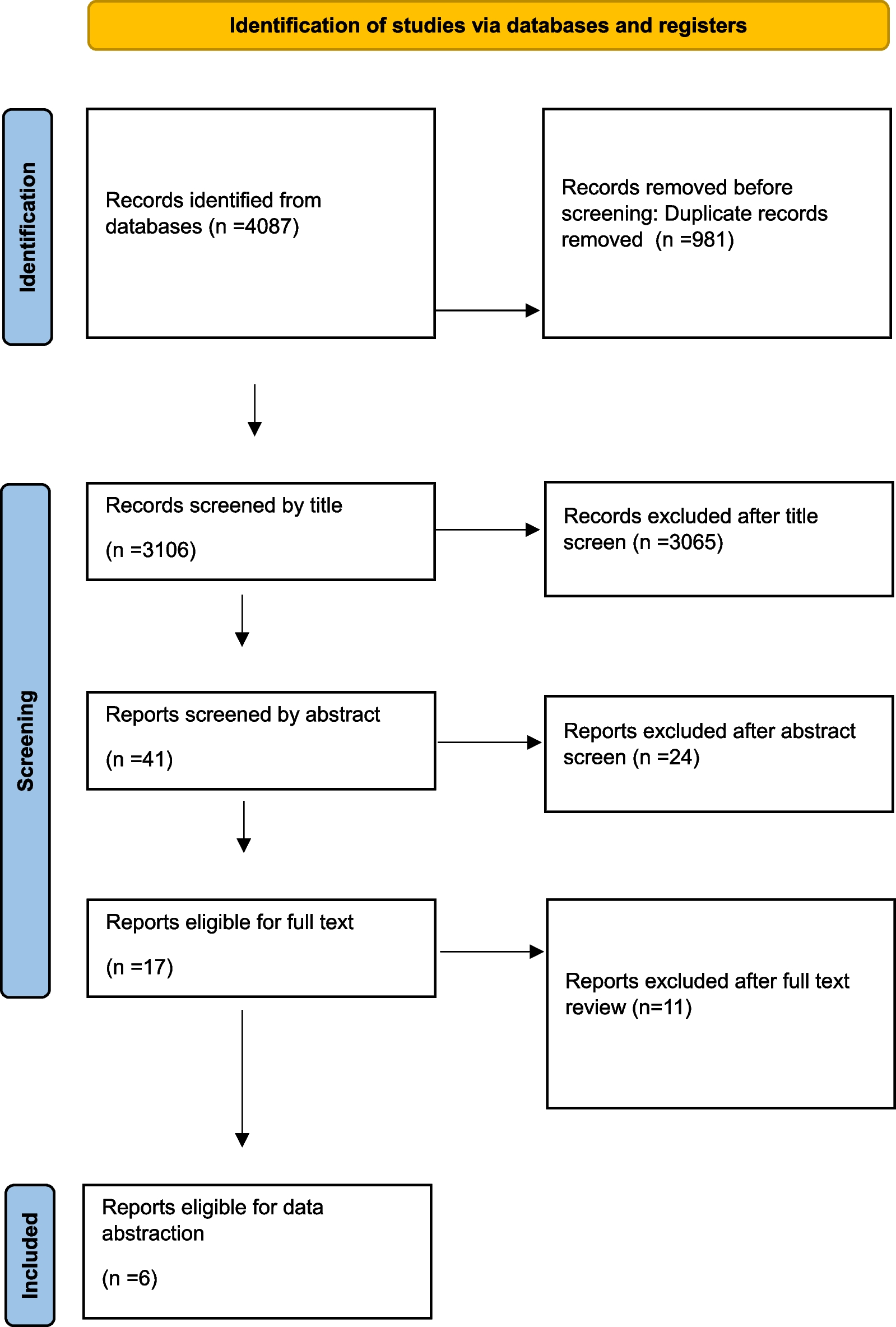
Overall, the combined search identified 10,878 records, of which 10,834 were excluded based on duplicates and the title and abstract evaluation. The remaining 44 articles underwent full-text evaluation, and 34 were excluded (Additional file 1: Table S4). Finally, ten RCTs including 1318 patients were included [31,32,33,34,35,36,37,38,39,40]. The PRISMA diagram of the study selection process is shown in Fig. 1.
Fig. 1
Literature search and screening process
Characteristics of included studiesTen RCTs were published from 1982 to 2020, nine were journal papers [31,32,33,34,35,36,37,38, 40] and one was a doctoral thesis [39]. Eight RCTs [33,34,35,36,37,38,39,40] focused on appendicitis and two RCTs [31, 32] focused on peritonitis caused by perforation or injury to the stomach, duodenum, small intestine, appendix, etc. No studies focused on infectious pancreatitis or fecal peritonitis. Eight RCTs involved adults [31, 32, 34,35,36,37, 39, 40] and two involved children [33, 38]. The majority of the patients with peritonitis involved in two RCTs [31, 32] were diffuse infections, and the patients with appendicitis involved in eight RCTs were localized infections [33,34,35,36,37,38,39,40]. Peritonitis studies have mainly focused on the outcomes of mortality, intra-abdominal abscess (IAA), incisional surgical site infections (SSI), and postoperative complications. Studies on appendicitis not only examine these outcomes, but also evaluate reoperation, readmission, operative time, length of stay, and hospital charges. Eight RCTs performed laparoscopic appendectomy [33,34,35,36,37,38,39,40] and two RCTs performed open surgery [31, 32] (Table 1). The RoB assessment showed that none of the included RCTs were blinded to participants and personnel. All RCTs did not specify whether the assessment of the outcome was blinded, six RCTs were unclear about allocation concealment, and four RCTs were unclear about random sequence generation (Additional file 1: Fig. S1).
Table 1 Characteristics of the included studiesMortalityThree RCTs with 373 patients reported on mortality, one included patients with appendicitis and two included patients with peritonitis [31, 32, 40]. There were no reported deaths in the IOPL group and two (1.1%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of mortality compared to non-IOPL for patients with appendicitis (RR, 0.31 [95% CI, 0.02–6.39]) (Fig. 2A). Ten patients with peritonitis (22.7%) died in the IOPL group, compared to 10 patients (23.3%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of mortality compared to non-IOPL for patients with peritonitis (RR, 0.97 [95% CI, 0.45–2.09], I2 = 0%) (Fig. 2A). No significant differences in mortality were found in other subgroups stratified by the type of population (child: no data on mortality; adult: RR, 0.91 [95% CI, 0.43–1.91]), irrigation volume (< 3L: RR, 0.31 [95% CI, 0.02–6.39]; ≥ 3L: RR, 0.97 [95% CI, 0.45–2.09]), and country income level (HIC: RR, 0.93 [95% CI, 0.29–3.03]; LMIC: RR, 0.89 [95% CI, 0.34–2.31]) (Table 2, Additional file 1: Fig. S2).
Fig. 2
Primary outcomes in patients with IAIs who used IOPL compared with patients who did not
Table 2 Subgroup analysis of primary outcomes in patients with IAIs who used IOPL compared with patients who did notIAANine RCTs with 1232 patients reported on IAA, seven included patients with appendicitis and two included patients with peritonitis [31,32,33,34,35, 37,38,39,40]. IAA occurred in 67 patients with appendicitis (12.3%) in the IOPL group and 72 patients with appendicitis (11.8%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of IAA compared to non-IOPL for patients with appendicitis (RR, 1.02 [95% CI, 0.70–1.48], I2 = 24%) (Fig. 2B). IAA occurred in two patients with peritonitis (5.1%) in the IOPL group and two patients with peritonitis (5.0%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of IAA compared to non-IOPL for patients with peritonitis (RR, 1.05 [95% CI, 0.16–6.98], I2 = 0%) (Fig. 2B). No significant differences in IAA were found in other subgroups stratified by the type of population (child: RR, 0.98 [95% CI, 0.57–1.70]; adult: RR, 1.02 [95% CI, 0.66–1.58]), irrigation volume (< 3L: RR, 0.97 [95% CI, 0.67–1.41]; ≥ 3L: RR, 0.90 [95% CI, 0.30–2.67]), and country income level (HIC: RR, 0.98 [95% CI, 0.66–1.46]; LMIC: RR, 0.91 [95% CI, 0.39–2.12]) (Table 2, Additional file 1: Fig. S2).
Incisional SSISix RCTs with 849 patients reported on incisional SSI, five included patients with appendicitis and one included patients with peritonitis [32, 34,35,36, 38, 40]. Incisional SSI occurred in 12 patients with appendicitis (3.3%) in the IOPL group and 16 patients with appendicitis (3.8%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of incisional SSI compared to non-IOPL for patients with appendicitis (RR, 0.72 [95% CI, 0.18–2.86], I2 = 50%) (Fig. 3A). Incisional SSI occurred in five patients with peritonitis (17.2%) in the IOPL group and six patients with peritonitis (20.7%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of incisional SSI compared to non-IOPL for patients with peritonitis (RR, 0.83 [95% CI, 0.29–2.43]) (Fig. 3A).
Fig. 3
Secondary outcomes in patients with IAIs who used IOPL compared with patients who did not
Postoperative complicationNine RCTs with 1096 patients reported on postoperative complication, seven included patients with appendicitis and two included patients with peritonitis [31, 32, 34,35,36,37,38,39,40]. Postoperative complication occurred in 52 patients with appendicitis (11.0%) in the IOPL group and 71 patients with appendicitis (13.2%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of postoperative complication compared to non-IOPL for patients with appendicitis (RR, 0.74 [95% CI, 0.39–1.41], I2 = 64%) (Fig. 3B). Postoperative complication occurred in 12 patients with peritonitis (28.6%) in the IOPL group and 11 patients with peritonitis (25.6%) in the non-IOPL group. The use of IOPL was not significantly associated with a decreased risk of postoperative complication compared to non-IOPL for patients with peritonitis (RR, 1.11 [95% CI, 0.55–2.23], I2 = 0%) (Fig. 3B).
ReoperationSix RCTs with 1019 patients reported on reoperation, in which all included patients were appendicitis [33,34,35, 37, 38, 40]. Reoperation occurred in 14 patients with appendicitis (2.9%) in the IOPL group and 9 patients with appendicitis (1.7%) in the non-IOPL group. The use of IOPL was not associated with a significantly decreased risk of reoperation compared with non-IOPL in patients with appendicitis (RR, 1.71[95% CI, 0.74–3.93], I2=0%) (Fig. 4A).
Fig. 4
Secondary outcomes in patients with appendicitis who used IOPL compared with patients who did not
ReadmissionFive RCTs with 759 patients reported on readmission, in which all included patients were appendicitis [33, 34, 37, 38, 40]. Readmission occurred in 18 patients with appendicitis (5.2%) in the IOPL group and 27 patients with appendicitis (6.6%)
留言 (0)