
記住我


Over a period of five years, spanning from July 2016 through June 2021, a total of 741 visits were completed at the ECC, providing care for 432 individual patients (Table 1). Of these, 220 patients (50.9%) returned for at least one follow-up appointment, and while we continued to gain substantial numbers of new patients, follow-ups accounted for an increasing proportion of visits yearly (Fig. 2). By 2020–2021 (Year 5), 62.5% of visits were follow-ups. Genetic medicine practices typically focus on initial diagnosis, yet our experience suggests that patients and their families prefer to continue receiving care where highly specialized and multidisciplinary expertise is available for this class of rare disorders. With the departure of one medical geneticist in 2018 (Year 3), the number of appointment slots had to be reduced by approximately 50% (Fig. 2). The ECC remained fully booked throughout the COVID-19 pandemic, which reached the United States by March 2020, towards the end of Year 4. In accordance with institutional safety guidelines, patients were evaluated by video visit whenever possible (Fig. 2). This was especially important as certain epigenetic conditions, such as Kabuki syndrome (MIM 147920 and 300867), can be associated with immunodeficiency (Margot et al. 2020).
Table 1 Epigenetic and Chromatin Clinic DemographicsFig. 2
Visits to the Epigenetics and Chromatin Clinic. Numbers and percentages of visits by year and type of visit. New visits are indicated with red shading, and follow-up visits are indicated with blue shading. Video visits are indicated with black diagonal lines. Year 1: July 2016-June 2017; Year 2: July 2017-June 2018; Year 3: July 2018-June 2019; Year 4: July 2019-June 2020; Year 5: July 2020-June 2021
A notable benefit of the widespread use of telemedicine was improved access to the ECC by out-of-state patients. The ECC has always drawn patients from a wide geographic range. In these five years, patients originated from 3 countries (United States, Australia, and Brazil) and 29 states of the U.S and the District of Columbia (Fig. 3). In total, 116 patients (26.9%) resided outside of Maryland. Other top states included Virginia (30 patients, 6.9%) and Pennsylvania (18 patients, 4.2%). The patient population we encountered was mixed, consisting of 63.4% White/Caucasian, 14.8% Black/African American, 6.9% Asian or Pacific Islander, and 14.8% multiracial or other; 9.0% of all patients identified as Hispanic or Latino (Table 1). Most patients (92.8%) preferred English, with Spanish as the second most common language (4.2%). Qualified language interpretation services were present at all appointments where English was not the language of choice.
Fig. 3
Geographic distribution of Epigenetics and Chromatin Clinic patients in the United States. Number of ECC patients residing in each state at the time of their visit(s) from July 2016 through June 2021. Colors represent the number of patients seen from the state: zero (light yellow); 1–5 (dark yellow); 6–10 (orange); 10–100 (orange red); more than 100 (dark red)
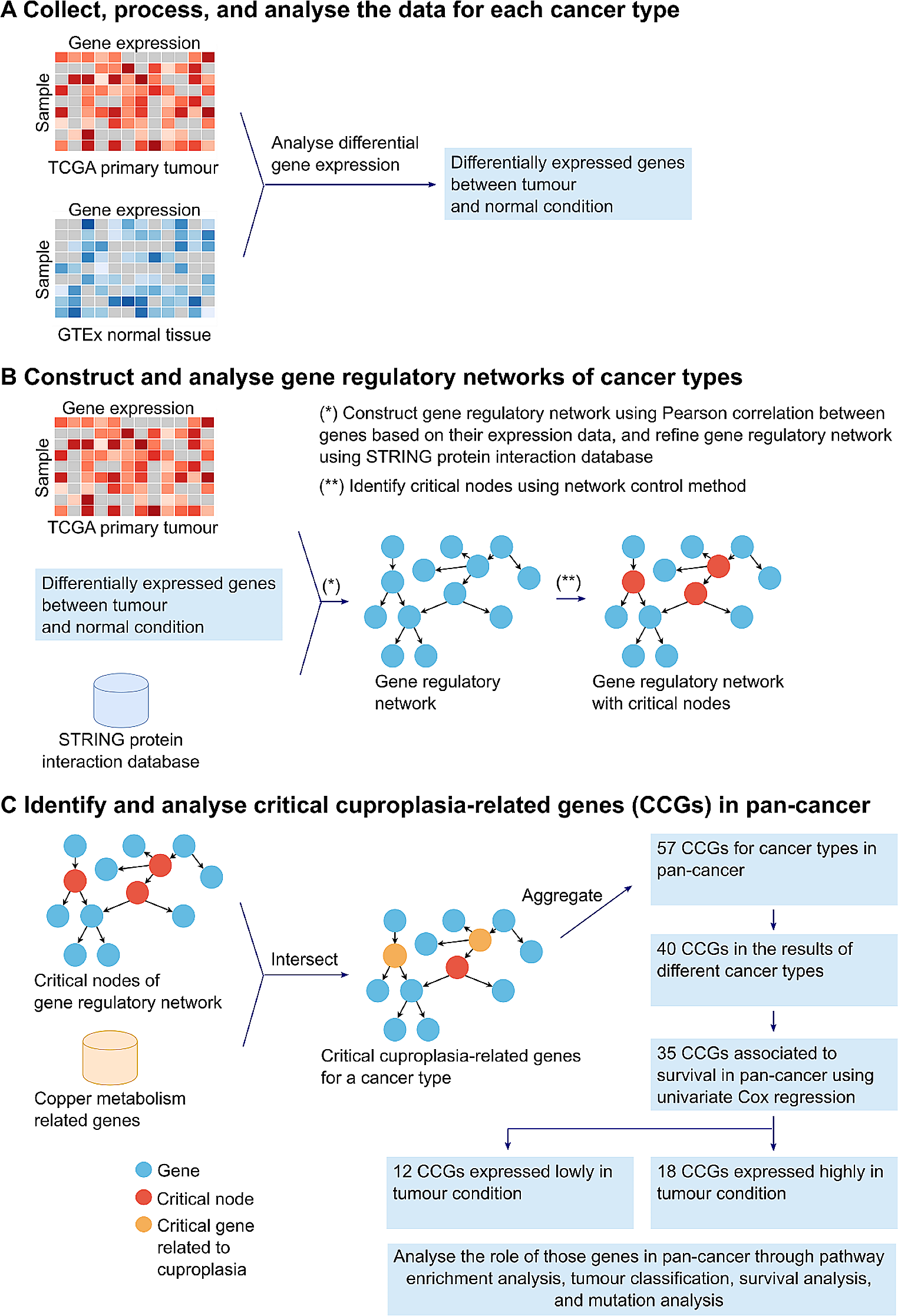
New patients are commonly referred to the ECC either because they are seeking expertise for a known epigenetic condition, or because they have a combination of a growth abnormality with developmental delay and/or intellectual disability. Altogether, 153 individuals with confirmed (clinically or molecularly) epigenetic disorders have been seen in the ECC over the 5-year span. 115 patients (26.6%) were diagnosed with a Mendelian disorder of the epigenetic machinery (MDEM), and 36 patients (8.3%) had an imprinting disorder (Fig. 4a). Notably, 2 patients were discovered to have pathogenic variants in SMARCC2 (Machol et al. 2019) and HIST1H1E (Tatton-Brown et al. 2017), which encode for a scaffolding component of the BAF complex (He et al. 2020) and a linker histone, respectively. Though not strictly considered epigenetic machinery, these proteins nonetheless play a critical role in the proper maintenance of chromatin states and the epigenome, and therefore we classify these as epigenetic disorders (Chromatinopathies). Of the remaining patients seen in the ECC, 139 patients (32.2%) were ultimately diagnosed with a non-epigenetic disorder, 119 (27.5%) remain undiagnosed pending further genetic testing, and 21 (4.9%) were deemed to have a non-genetic etiology (Fig. 4a).
Fig. 4
Patient diagnoses in the Epigenetics and Chromatin Clinic. a Broad categories of diagnoses seen in the ECC from July 2016 through June 2021 include MDEMs (red), Imprinting (blue), and Epigenetic, Other (orange), which are categorized as epigenetic, as well as Non-epigenetic (purple), Undiagnosed (yellow), and None (aqua). Diagnosis types are defined in the text. b Top 5 MDEMs diagnosed July 2016 through June 2021. KS1 Kabuki syndrome 1 (red); WSS Wiedemann-Steiner syndrome (blue); SS Sotos syndrome (yellow); ATS Arboleda-Tham syndrome, also known as KAT6A-associated neurodevelopmental disorder or KAT6A syndrome (purple); MRD1 Intellectual development disorder, autosomal dominant 1, formerly known as Mental retardation, autosomal dominant 1 (orange). All other MDEM diagnoses (aqua)
Among MDEMs, Kabuki syndrome 1 was the most common disorder seen in our clinic, accounting for 34 patients (29.6%) (Fig. 4b). This was followed by Wiedemann-Steiner syndrome (14 patients; 12.2%; MIM 605130), Sotos syndrome (12 patients; 10.4%, MIM 117550), Arboleda-Tham syndrome, also known as KAT6A syndrome (10 patients; 8.7%; MIM 616268), and Intellectual developmental disorder, autosomal dominant 1, also known as MRD1 (7 patients, 6.1%, MIM 156200). In total, we provided care for patients with 26 distinct MDEMs (Table 2). Among imprinting disorders, Beckwith-Wiedemann syndrome (BWS; MIM 130650) was by far the most common (20 patients; 55.6% of imprinting disorders).
Table 2 Mendelian disorders of the epigenetic machinery seen in the Epigenetics and Chromatin ClinicPhenotypic insights from the Epigenetics and Chromatin ClinicOf the 153 patients with epigenetic disorders, 139 individuals have a neurodevelopmental disability of some kind, with 132 individuals exhibiting developmental delay, cognitive impairment, or intellectual disability. BWS (20 individuals) and Russell-Silver syndrome (RSS; 3 individuals) are generally reported to not cause significant neurodevelopmental disabilities. However, we noticed that 9/20 individuals (45%) with a BWS diagnosis have attention-deficit/hyperactivity disorder (ADHD) or a language delay. This has not been previously reported in the literature, although one study from 2008 reported that these children have higher than normal behavioral and emotional problems (Kent et al. 2008). One individual with BWS had profound ID and cerebral palsy, but this was thought to be due to a severe anoxic brain injury shortly after birth as opposed to a direct result of BWS. Another individual with language delay had a confounding paternal interstitial duplication of chromosome 11. We also recognize that some of the language delay in these patients may be solely structural due to macroglossia, although with the known association of ADHD and language delay, some of this may be a true language delay (Mueller and Tomblin 2012). Of the 130 individuals with non-BWS and non-RSS epigenetic disorders, every single one (100%) has some neurodevelopmental disorder and a striking 129/130 (99.2%) had developmental delay, cognitive impairment, or intellectual disability. The single exception is a 22-year-old with Schaaf-Yang syndrome who only has severe anxiety but no other neurodevelopmental diagnosis.
Every single one of the 115 individuals seen in the ECC with a MDEM has some neurodevelopmental disability that includes developmental delay, cognitive impairment, or intellectual disability. This ranges from profound intellectual disability to more mild but still impactful phenotypes such as specific learning disabilities or ADHD. Cognitively, 21/115 individuals (18.3%) have mild impairments that do not meet the level of intellectual disability (Fig. 5). Specifically, 39/115 individuals (33.9%) have mild intellectual disability (or a developmental quotient in that range), 34/115 (29.6%) have moderate intellectual disability (or a developmental quotient in that range), and 21/115 (18.3%) individuals have severe or profound intellectual disability (or a developmental quotient in that range; Fig. 5). Thirteen individuals (11.3%) are nonverbal (Fig. 5). In addition to cognitive impairment, the other two most commonly seen neurodevelopmental endophenotypes in the MDEM group are ADHD and anxiety. In all, 44/115 individuals (38.3%) have clinically significant ADHD and 39/115 individuals (33.9%) have clinically significant anxiety (Fig. 5). In contrast, only 10/115 (8.7%) carry diagnoses of autism spectrum disorder (Fig. 5), which supports previous literature that many MDEM syndromes predispose individuals to high sociability (Awan et al. 2022; Chan et al. 2019; Mervis et al. 2005). Lastly, two other common neurodevelopmental features among the group of individuals with MDEMs are hypotonia and seizures. Clinically notable hypotonia was present in 95/115 (82.6%) individuals at some point in their life. This may even be an underrepresentation given that individuals evaluated in later childhood may have poor documentation of tone in infancy and preschool ages, given that hypotonia typically improves with age. We found 24/115 (20.9%) had seizures at some point with 19 of those having a seizure disorder that required treatment (Fig. 5).
Fig. 5
Neurodevelopmental phenotypes among Mendelian disorders of the epigenetic machinery seen in the Epigenetics and Chromatin Clinic. Number of individuals with each described neurodevelopmental phenotype among the 115 patients with MDEMs broken out by the 5 most common diagnoses and all others (aqua). KS1 Kabuki syndrome 1 (red); WSS Wiedemann-Steiner syndrome (blue); SS Sotos syndrome (yellow); ATS Arboleda-Tham syndrome (also known as KAT6A-associated neurodevelopmental disorder or KAT6A syndrome; purple); MRD1 Intellectual development disorder, autosomal dominant 1, formerly known as Mental retardation, autosomal dominant 1 (orange). It should be noted that quite a few of the individuals with the different syndromes were infants or toddlers and so their ADHD and anxiety phenotypes remain unknown
When we look at our 5 most common MDEM diagnoses, of 34 individuals with Kabuki syndrome type 1 (KS1), 8 (23.5%) have borderline cognitive impairment or global developmental delay above the cutoff for intellectual disability, 17 (50%) have mild intellectual disability or a developmental quotient (DQ) in that range, 7 (20.6%) have moderate intellectual disability or a DQ in that range, 2 (5.9%) have severe or profound intellectual disability (one is a child who had autoimmune encephalopathy in addition to KS1). Three (8.8%) are nonverbal. Two of these nonverbal children use assistive technology and signs to communicate, and one child has not been seen for follow up in clinic and so this data is unknown. Behaviorally, 14 (41.2%) have ADHD, 16 (47.1%) have anxiety, and 4 (11.8%) have autism. Hypotonia was present in 31 (91.2%) and 6 (17.6%) have seizures (Fig. 5). Of 14 individuals with Wiedemann-Steiner syndrome, 3 (21.4%) have borderline cognitive impairment or global developmental delay above the cutoff for intellectual disability, 8 (57.1%) have mild intellectual disability or a DQ in that range, 3 (21.4%) have moderate intellectual disability or a DQ in that range, and none have severe or profound intellectual disability. None are nonverbal. Behaviorally, 10 (71.4%) have ADHD, 9 (64.3%) have anxiety, and 1 (7.1%) has autism. Hypotonia was present in 13 (92.9%) and 1 (7.1%) has seizures (Fig. 5). Of 12 individuals with Sotos syndrome, 4 (33.3%) have borderline cognitive impairment or global developmental delay above the cutoff for intellectual disability, 4 (33.3%) have mild intellectual disability or a DQ in that range, and 4 (33.3%) have moderate intellectual disability or a DQ in that range. None have severe or profound intellectual disability, and none are nonverbal. Behaviorally, 5 (41.7%) have ADHD, 5 (41.7%) have anxiety, and none have autism. Hypotonia is present in 11 (91.7%) and 2 (16.7%) have seizures (Fig. 5). Of 10 individuals with Arboleda-Tham syndrome, 1 (10%) has borderline cognitive impairment or global developmental delay above the cutoff for intellectual disability, 1 (10%) has mild intellectual disability or a DQ in that range, 3 (30%) have moderate intellectual disability or a DQ in that range, and 5 (50%) have severe or profound intellectual disability. Four (40%) are nonverbal. Behaviorally, 5 (50%) have ADHD, none have anxiety, and 1 (10%) has autism. 9 (90%) have hypotonia and none have seizures (Fig. 5). Of 7 individuals with Intellectual developmental disorder, autosomal dominant 1, 1 (14%) has borderline cognitive impairment or global developmental delay above the cutoff for intellectual disability, 1 (14.3%) has mild intellectual disability or a DQ in that range, 2 (28.6%) have moderate intellectual disability or a DQ in that range, and 3 (42.9%) have severe or profound intellectual disability. None are nonverbal. Behaviorally, 5 (71.4%) have ADHD, 5 (71.4%) have anxiety, and none have autism. Two (28.6%) have hypotonia and 2 (28.6%) have seizures (Fig. 5). It should be noted that quite a few of the individuals with the different syndromes were infants or toddlers and so their ADHD and anxiety phenotypes remain unknown.
Eighty-one individuals with MDEMs (70.4%) had some type of growth abnormality, with height affected in 69 individuals (60%) and head size affected in 49 individuals (42.6%) (Fig. 6a,b). Thirty-seven individuals with MDEMs (32.2%) had growth abnormalities affecting both height and head circumference. Of those with growth abnormalities, 63 (77.8%) exhibited growth retardation–with 56 having short stature, 35 having microcephaly, and 28 with both (Fig. 6a). Eighteen individuals (22.2%) exhibited overgrowth–13 with tall stature, 14 with macrocephaly, and 9 with both (Fig. 6b). Only 18/89 individuals with MDEMs (20.2%) exhibited abnormalities in birth growth parameters; however, information was unavailable for 26 individuals.
Fig. 6
Growth abnormalities observed in patients with Mendelian disorders of the epigenetic machinery in the Epigenetics and Chromatin Clinic. Venn diagram for a growth retardation and b overgrowth based on whether height, occipital-frontal head circumference (OFC), or both were affected. Numbers indicate the total number of affected individuals with each feature; gene names indicate the epigenetic machinery component disrupted. *Indicates gene unknown. This is the case for Kabuki-Turner syndrome (KTS), as its molecular etiology is not known, and for Kabuki syndrome not otherwise specified (KS NOS), as the individual met clinical criteria for KS, but no pathogenic variant was identified in either gene that causes KS (KMT2D or KDM6A). + indicates that the affected individual had a pathogenic variant in another gene in addition to EP300. Parentheses indicate that for these genes, overgrowth is not typically observed. Only 18/89 individuals with MDEMs (20.2%) exhibited abnormalities in birth growth parameters; however, information was unavailable for 26 individuals
Molecular insights from the Epigenetics and Chromatin ClinicMDEMs result from pathogenic variants in writers, erasers, readers, and remodelers of chromatin marks (Bjornsson 2015; Fahrner and Bjornsson 2014; Fahrner and Bjornsson 2019) (Fig. 1). Some epigenetic machinery components exhibit dual function, including both a non-enzymatic reader domain and an enzymatic writer, eraser, or remodeler domain (Boukas et al. 2019; Fahrner and Bjornsson 2019) (Fig. 1; Table 2). Of the 26 distinct MDEMs seen in our clinic in the past 5 years, 12 (46.2%) impact writers, 6 (23%) impact erasers, 4 (15.4%) impact readers without dual functions, and 3 (11.5%) impact remodelers (Fig. 7). The exact molecular etiology of one disorder, Kabuki-Turner syndrome, remains unknown (Dennis et al. 1993; Wellesley and Slaney 1994; Rodriguez et al. 2008). Sixteen MDEMs seen in our clinic (61.5%) result from pathogenic variants in dual function components (Table 2). This includes all the remodeler disorders, 10 of the 12 writer disorders, and 3 of the 6 eraser disorders (Fig. 7).
Fig. 7
Components of the epigenetic machinery disrupted in patients from the Epigenetics and Chromatin Clinic. Functions of the epigenetic machinery implicated in the 26 Mendelian disorders of the epigenetic machinery seen in the ECC from July 2016 through June 2021. Proportion of each category: writers (red); erasers (blue); readers (yellow); and remodelers (orange). Purple indicates that the epigenetic machinery component function is unknown. The proportion of each enzymatic component (writer, eraser, remodeler) with dual function (i.e., with an accompanying reader domain) is indicated with black dots. The numbers correspond to the disorders listed in Table 2
According to published literature, the vast majority of MDEMs are inherited in an autosomal dominant manner and result from de novo variants in probands; a smaller fraction of genes are located on the X chromosome or exhibit autosomal recessive inheritance (Bjornsson 2015; Fahrner and Bjornsson 2019) (Fig. 1). Of the 26 distinct MDEMs seen in the ECC, 18 (69.2%) exhibit autosomal dominant inheritance, five (19.2%) exhibit X-linked inheritance, one (3.8%) exhibits autosomal recessive inheritance, and two (7.7%) have both autosomal dominant and autosomal recessive forms described (Table 2).
Fifty-eight individuals out of 115 with MDEMs (50%) were diagnosed by whole exome sequencing (WES), and 39 (34%) were diagnosed by single gene or gene panel testing. The latter category was dominated by individuals with Kabuki, Sotos, and CHARGE (MIM 214800) syndromes, which are all well-known and recognizable to many clinical geneticists because of their well-described and specific constellations of phenotypic features. Most of the remaining 18 individuals with MDEMs who were not diagnosed using WES or gene or gene panel testing had copy number variants and thus were diagnosed by SNP microarray. This included individuals with Intellectual Developmental Disorder, Autosomal Dominant 1 due to 2q23.1 deletions or duplications, Kleefstra syndrome 1 (MIM 610253) due to 9q34.3 deletions, Sotos syndrome due to 5q35 deletions, Wolf-Hirschorn syndrome (MIM 194190) due to 4p16.3 deletion, Smith-Magenis syndrome (MIM 182290) due to 17p11.2 deletion, and Brachydactyly-mental retardation syndrome (MIM 600430) due to 2q37 deletion. Two individuals with Kabuki syndrome-like phenotypes had X chromosome abnormalities diagnosed by karyotype suggestive of Kabuki-Turner syndrome (Dennis et al. 1993; Wellesley and Slaney 1994; Rodriguez et al. 2008) with one having tested negative for mutations in both Kabuki syndrome genes. Two patients met clinical criteria for particular diagnoses (CHARGE and Kabuki syndrome) but lacked molecular confirmation. Both individuals with Chromatinopathies who did not meet criteria for a MDEM were diagnosed by exome sequencing.
Genome-wide DNA methylation profiling as a diagnostic toolOver the past few years, it has become clear that genome-wide DNA methylation profiling is a useful tool for the diagnosis of an increasing number of MDEMs and other neurodevelopmental disorders (Aref-Eshghi et al. 2019; Aref-Eshghi et al. 2020; Aref-Eshghi et al. 2017; Choufani et al. 2015; Choufani et al. 2020; Levy et al. 2022; Sadikovic et al. 2020; Sadikovic et al. 2021). Classically, DNA methylation occurs at cytosines followed by guanines (CpGs). Performed on DNA isolated from human whole blood, DNA methylation array analysis can identify sensitive and specific genome-wide DNA methylation profiles associated with particular genes and syndromes. These so-called “episignatures” consist of a collection of CpG sites whose DNA methylation is altered similarly in a particular disease state compared to other disease states and controls. In many cases, these DNA methylation profiles can confirm or refute the pathogenicity of DNA sequence variants, aiding in diagnosis (Aref-Eshghi et al. 2019; Aref-Eshghi et al. 2020; Aref-Eshghi et al. 2017; Choufani et al. 2015; Choufani et al. 2020; Levy, McConkey et al. 2022; Sadikovic et al. 2020; Sadikovic et al. 2021). Some data suggest that differentially methylated regions (DMRs) identified by DNA methylation array profiling of blood may have biological significance as well (Levy et al. 2021; Levy, Relator, et al. 2022b). Importantly, there is now a clinical DNA methylation array test called EpiSign (Aref-Eshghi et al. 2020; Sadikovic et al. 2020) available in the United States (ggc.org/episign) and the Netherlands (genoomdiagnostiek.nl/product-tag/episign/) that has been useful diagnostically in our ECC.
We have sent clinical DNA methylation profiling on six patients from our clinic since it became available in 2019. In general, clinical DNA methylation profiling is used as a variant interpretation tool (EpiSign Variant) or as part of the broader diagnostic work up (EpiSign Complete). In two cases, EpiSign Complete was negative and non-diagnostic. In one case it revealed a diagnosis of the imprinting disorder Temple syndrome (MIM 616222) in a 7-year-old girl with reduced growth prenatally and postnatally, infantile feeding difficulties, persistent short stature, later-onset obesity, developmental delay, behavioral challenges including skin picking, hypotonia, and precocious puberty. In a second case, we successfully used EpiSign Variant to confirm pathogenicity of a variant of uncertain significance in the well-known CHD7 gene responsible for CHARGE syndrome in a family with an atypical presentation of the disease. The proband had one major and two minor criteria for a diagnosis of CHARGE syndrome (Hale et al. 2016)–unilateral coloboma, heart defect, and mild developmental delay–and was found to have a missense variant of uncertain significance in CHD7. Familial testing revealed the variant in her seemingly unaffected father, who on further evaluation had a history of mild developmental delay, poor childhood growth, mild unilateral facial nerve palsy, and recurrent blocked tear ducts requiring multiple surgeries, and in her infant brother, who had cataracts, noisy breathing, and severe constipation. Simultaneous grandparental testing revealed that the variant occurred de novo in the proband’s father, supporting pathogenicity and further confirming the EpiSign results. In a third case, we used EpiSign Variant to confirm Kabuki syndrome 1 in a patient with a low-level somatic mosaic de novo nonsense variant in KMT2D who had severe congenital heart disease and was initially too critically ill for his features of Kabuki syndrome to be fully appreciated (Montano et al. 2022). Conversely, in addition to confirming variants of uncertain significance as pathogenic, we have used EpiSign Variant to help rule out pathogenicity. A female proband with poorly defined neurodevelopmental difficulties was found to have a missense variant of uncertain significance in KDM5C inherited from a mother with a history of traumatic brain injury. EpiSign Variant revealed that the DNA methylation profile did not match that of other female carriers of pathogenic KDM5C variants (Schenkel et al. 2018), a fraction of whom have mild ID; this helped to rule out a diagnosis of Claes-Jensen X-linked Intellectual Developmental Disorder (MIM 300534) in the family.
Discovery and advancement of novel disorders in the Epigenetics and Chromatin ClinicAs mentioned above, there has been rapid discovery of novel MDEMs, or Chromatinopathies. The knowledge gained through our ECC has allowed our group to participate in the discovery of two such disorders. Pilarowski-Bjornsson syndrome (MIM 617682) is a rare neurodevelopmental disorder associated with speech abnormalities, macrocephaly, and developmental delay (Pilarowski et al. 2018). The original cohort involved 6 female individuals with de novo missense variants in CHD1. Since then, additional patients have been identified with phenotypes that overlap with other syndromes caused by the CHD family of genes, such as speech problems, macrocephaly, and intellectual disability (Yasin and Zahir 2020). In addition, we delineated Beck-Fahrner syndrome (BEFAHRS, MIM 618798), which results from mono- or bi-allelic variants in TET3 and defines a new biochemical category of MDEMs impacting the DNA demethylation eraser system (Beck et al. 2020). Similar to other MDEMs, BEFAHRS has a predominantly neurodevelopmental phenotype with occasional growth abnormalities, as suggested by its mnemonic: Behavioral differences, Epilepsy, characteristic Facial features, Autistic features, Hypotonia, Retardation of psychomotor dev
留言 (0)