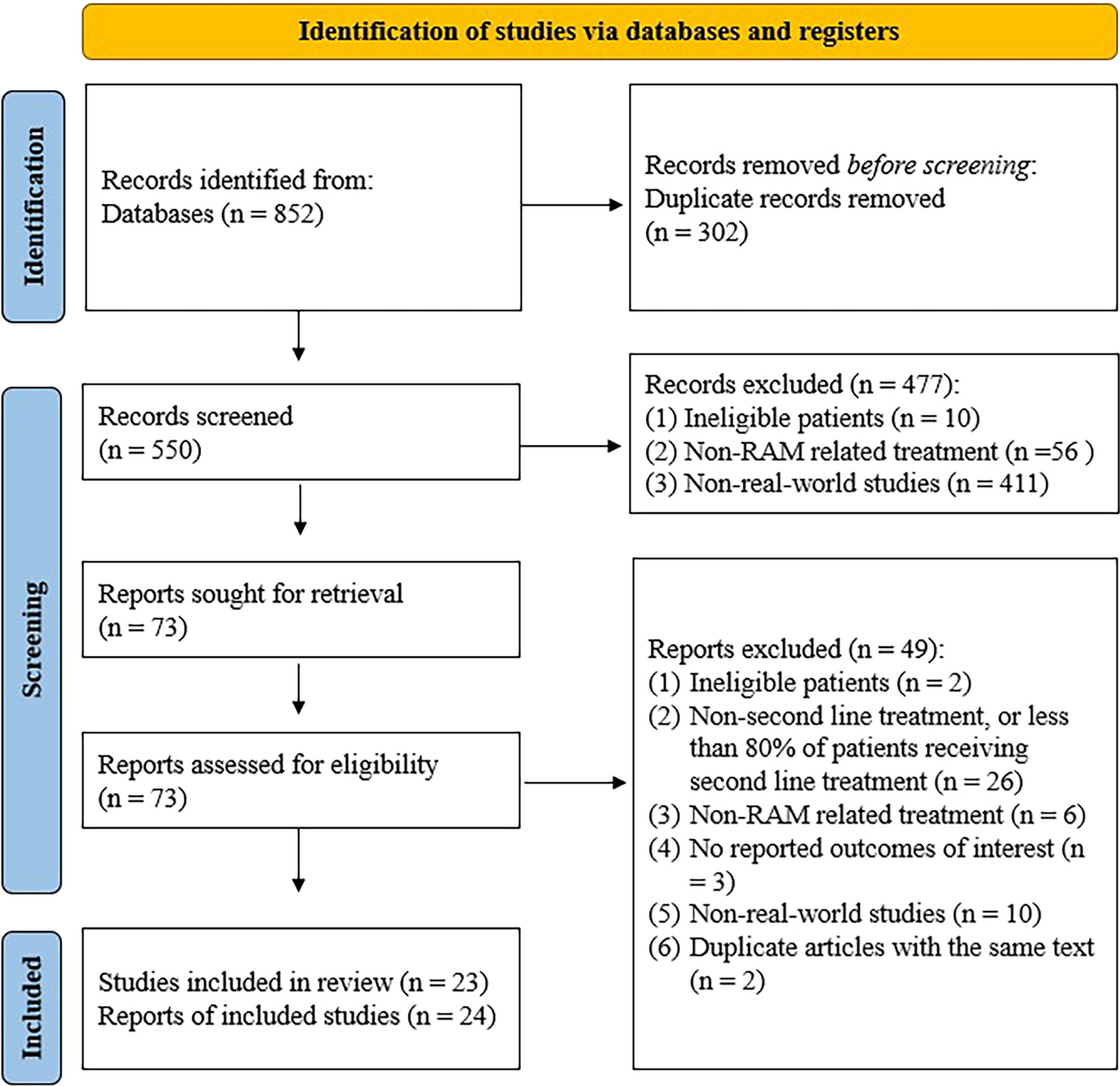
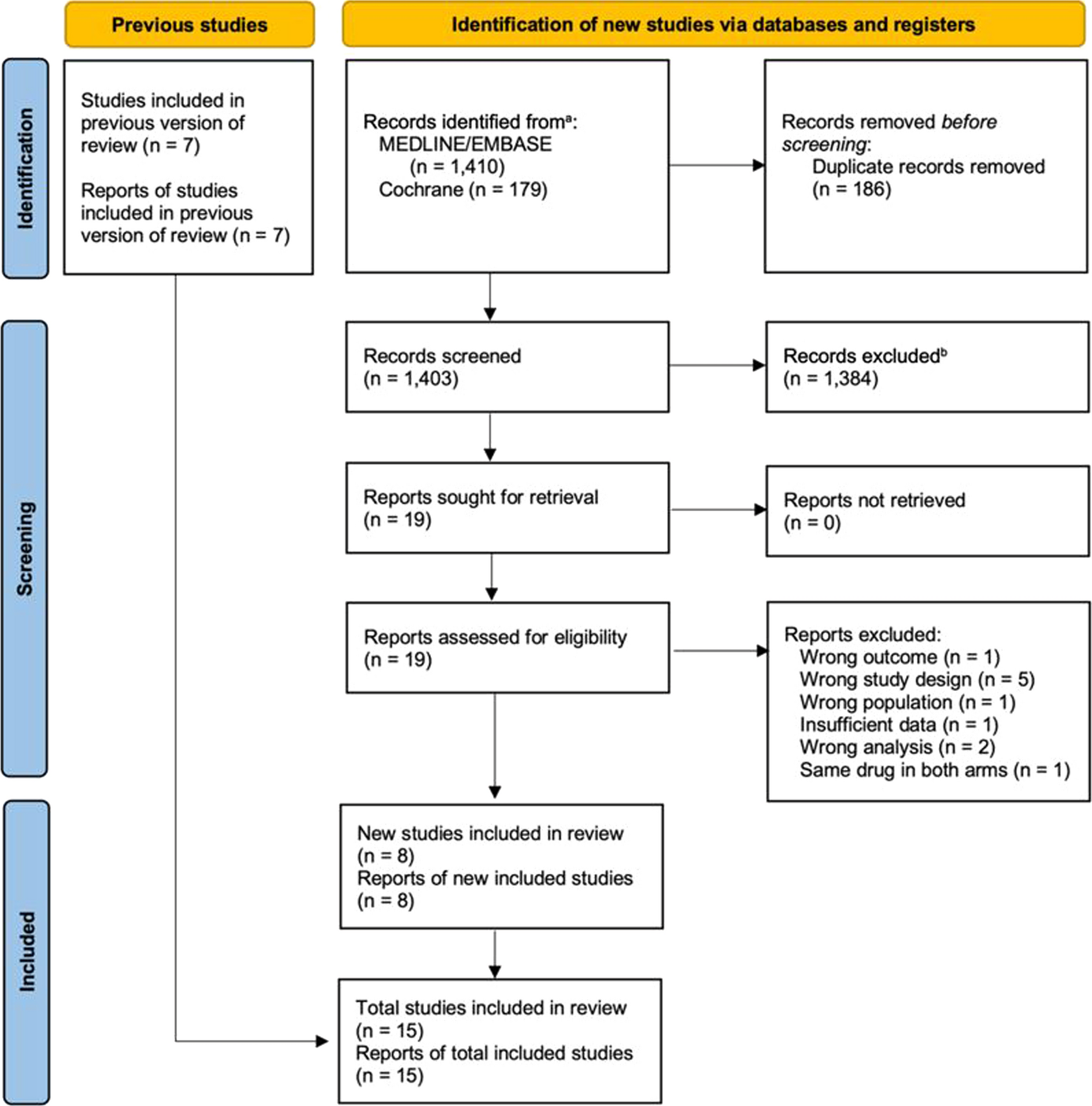
A literature search in the PubMed database was performed for research articles published up to November 2022, and included any of the terms, Cardiac Arrest, Targeted Temperature Management, Post-Cardiac Arrest Syndrome, Heart Arrest, Temperature Control, and Hypothermia, were reviewed and included in this scoping review. The citations included were analyzed to determine if any additional articles met the inclusion criteria. Only peer-reviewed articles published in the English language were considered for this scoping review.
Mechanisms of Neurologic Injury in Cardiac Arrest
HIBI is one of the most feared complications from CA [14], and encompasses both primary and secondary neuronal injuries. Along with shock-like endotheliopathy, secondary brain injury mechanisms are the cornerstone of the post-resuscitation syndrome, making them appealing targets for interventions aimed at improving neurological outcomes and survival post-CA.
Primary Brain Injury
Primary brain injury occurs during the “no-flow” phase of CA when oxygenation to vital organs becomes compromised. Previous data have reported that electroencephalographic (EEG) attenuation or suppression ensues within 30 s of circulatory arrest. However, in rare cases, EEG activity can continue for several minutes after blood flow ceases [15]. Neuronal death may occur within minutes [16]. This ischemic injury continues until partial reperfusion is restored during cardiopulmonary resuscitation (CPR), and is characterized by depletion of ATP causing dysfunction of ion exchange pumps [6]. The loss of transmembrane ionic gradient leads to anoxic depolarization, a type of spreading depolarization characterized by a massive wave of depolarization, causing cytotoxic edema, release of glutamate, and excitotoxicity. Anoxic depolarization leads to cell death unless bioenergetic supply is restored [17, 18]. Additional mechanisms in primary brain injury include intracellular acidosis, neuronal excitotoxicity, and apoptosis [16]. It is imperative to restore perfusion promptly, as the brain is uniquely intolerant to ischemia, and animal studies have shown that signs of cerebral edema begin to appear on imaging as early as during the initial “no-flow” phase of CA [19].
Secondary Brain Injury
When CPR is initiated and a temporary “low-flow” state ensues, cerebral blood flow (CBF) is restored at ~ 25% of its normal rate [6]. This suboptimal CBF is insufficient to effectively perfuse the brain, and subsequent neuronal damage through complex mechanisms follows. Immediately after the return of spontaneous circulation (ROSC), there is a transient state of “no-reflow”, which is characterized by microcirculatory failure despite restoration of forward flow [20]. Recently, this “no-reflow” phenomenon has been observed in vivo, and is hypothesized to be caused by cortical hypoperfusion due to reduced capillary red blood cell velocity. This multifaceted phenomenon occurs in multifocal areas in the brain parenchyma, and its effect compound on impaired cerebral autoregulation, blood–brain barrier dysfunction, cerebral edema, intracellular Ca2+ accumulation, and release of reactive oxygen and nitrogen species, a cascade which results in further cell death [6, 16, 21, 22]. These physiological changes may continue over the course of days post-arrest, leading to secondary brain injury, and have become the main targets of interventions aiming to mitigate HIBI.
The Role of Temperature Control in Post-Cardiac Arrest Care
Hyperthermia following CA is common, with over 40% CA survivors experiencing elevated core temperatures within 48 h of ROSC. Post-CA hyperthermia has been shown to have deleterious effects on survival and neurological outcomes [13, 23,24,25]. A temperature > 37.5 °C following resuscitation will potentiate neuronal injury by further disrupting the blood–brain barrier, increasing cerebral metabolism, intracellular Ca2+ influx, and enhancing neuronal excitotoxicity, ultimately enhancing cell-death pathways [16]. In addition, hyperthermia post-CA may further impair cerebral autoregulation [26]. For this reason, guidelines universally recommend avoiding hyperthermia (> 37.7 °C) for at least 72 h after ROSC [9, 10].
Temperature control is a standard practice in post-CA care, and involves actively maintaining a temperature between 32 and 37.5 °C for at least 24 h in patients who remain unresponsive to verbal commands after ROSC [9, 27]. Currently, guidelines recommend initiating temperature control as early as possible following ROSC in patients who do not respond to verbal commands, regardless of location of arrest and type of non-perfusing rhythm.
The Scientific Premise of Hypothermia and Neuroprotection
The neuroprotective effects of modulating temperature following HIBI are well established in the literature, and include decreasing cerebral metabolic rate (cerebral metabolic rate decreases by ~ 6% per every 1 °C the temperature is decreased), inhibition of the inflammatory cascade, minimizing release of excitatory neurotransmitters, decreasing neuronal apoptosis, and preserving the blood–brain barrier integrity [9, 28, 29]. This neuroprotection was first demonstrated in humans in a case series of four adult and pediatric patients who experienced CA and were cooled to 30–33 °C via a water-cooled mattress for at least 24 h [30]. At discharge, three patients had complete neurological recovery, while one had severe visual deficits that fully resolved after 1 month. These findings were later confirmed by a slightly larger case series comprising 19 patients who suffered CA; 7 patients did not undergo hypothermia and the remaining 12 were cooled to 31–32 °C with a cooling blanket. Of the 12 patients who were cooled, 50% survived compared to the 14% who survived in the non-treatment group [31]. Although these initial studies were not randomized, controlled trials (RCT), the results were promising; however, research on hypothermia post-CA was almost halted due to difficulty managing complications such as arrhythmias and shivering [32]. In the decades that followed, preclinical studies consistently showed improved neurological outcomes post-CA when hypothermia was implemented during, or shortly after, circulatory arrest [32, 33]. This body of evidence prompted the design of the two landmark trials published in 2002 showing the efficacy of hypothermic temperature control on improving neurological outcomes in OHCA survivors with shockable rhythm who were unresponsive to verbal commands.
Early Clinical Trials on Hypothermia
The Hypothermia After Cardiac Arrest (HACA) study enrolled 275 adults who suffered OHCA with ventricular fibrillation (VF) or pulseless ventricular tachycardia from cardiac etiology, and remained unable to follow commands after ROSC; 55% of the patients who underwent hypothermia (32–34 °C) for 24 h had achieved independence at 6 months compared to 39% of those in the control group [34]. Of note, the target temperature was not specified in the control group in this study. Bernard et al. found similar results in a study that enrolled 77 comatose adults from VF OHCA from any etiology (no definition for coma was provided). Of the 43 patients who underwent hypothermia targeting 33 °C for 12 h, 49% had early favorable outcomes (discharge to home or rehabilitation) as opposed to 26% of the 34 patients in the normothermia group targeting 37 °C [35]. Both trials used cooling devices without a loop feedback mechanism, employed no control on the rate of rewarming, nor maintained normothermia following the cooling phase. Additionally, post-CA care and neuroprognostication were not standardized. After the publication of these trials, temperature control was quickly incorporated into guideline recommendations as standard post-CA care for adults suffering OHCA of shockable rhythms.
Evolution of Evidence Surrounding Temperature Control
Although the results of these two landmark trials were promising, there were several limitations that dampened the enthusiasm: they were open-label, their sample size the small with a high rate of screen failures (thus, raising concern for non-generalization), and at the time there were no established protocols for neuroprognostication post-CA and withdrawal of life-sustaining therapy (WLST) [36]. These limitations were subsequently addressed in the 2013 TTM1 trial, a RCT that analyzed 939 adult OHCA patients who remained unresponsive to verbal commands, and randomly assigned them to either temperature control at 33 °C or 36 °C for 24 h, followed by controlled active rewarming at 0.5 °C/h to 37 °C and subsequent normothermia until 72 h from randomization. Patients with a presumed cardiac etiology and any non-perfusing rhythm were eligible, excluding unwitnessed arrests with asystole as presenting rhythm. Standardized post-CA care was performed, including sedation and neuroprognostication, by a blinded independent physician using multimodal prognostication. The authors found no difference in survival or neurological outcomes at 6 months [37]. It is important to mention that the temperature in both arms was actively managed and no patient’s temperature was allowed to “self-regulate.” Unfortunately, within months of publication of the TTM1 trial, there was an abrupt drop in temperature control use altogether following CA in the United States, as well as decreased survival-to-discharge rates [38]. However, this reported decrease in survival rates could not be fully explained by the decline in temperature control use given the small number of hospitals used for the analysis. Post-CA care guidelines in 2015 started to recommend temperature control between 32 and 36 °C for at least 24 h in patients who remained comatose after OHCA or IHCA despite initial rhythm; however, data on the potential benefit of temperature control in patients who presented with an initial non-shockable rhythm (pulseless electrical activity (PEA) or asystole), or those who suffered IHCA, were lacking. Subsequently, a large retrospective study capturing the transition of target temperature during temperature control in a high-volume CA center demonstrated a negative impact on outcomes with shifting target temperatures from 33 to 36 °C [39].
In 2019, the HYPERION trial demonstrated that temperature control at 33 °C for at least 24 h in adults who suffered OHCA and IHCA with initial non-shockable rhythms increased favorable neurological outcomes at 90 days compared to targeted normothermia at 37 °C (10.2% vs. 5.7%) [40]. The study recruited 584 participants in France, but still had a high fragility index for this outcome. Two years later, the results of the largest and most rigorous RCT on temperature control to date, TTM2, challenged the routine use of target temperatures at 33 °C for OHCA of presumed cardiac etiology. The TTM2 trial recruited 1861 OHCA patients with shockable and non-shockable rhythms, and showed no difference in mortality or independence on ambulation at 6 months with targeted hypothermia at 33 °C versus targeted normothermia at < 37.5 °C [41]. Conversely, clinically significant arrhythmias were more common in the hypothermic group (24% vs. 16%). Since the publication of TTM2, there has been a debate on whether temperature control beyond merely preventing fever (i.e., ≤ 37.8 °C) during the first 72 h post-CA is enough to impact survival and neurological recovery [12, 13]. The TTM2 study had notable strengths, such as the largest sample size thus far, sound statistical methodology, blinding of families, statisticians, and outcome assessors, as well as established neuroprognostication protocols by an independent blinded physician only after 96 h post-randomization [12, 42]. Nonetheless, caution in extrapolating data from this trial to all CA populations is advised. In TTM2, over 90% of recruited patients experienced a witnessed CA and approximately 80% had bystander CPR [41]. These rates of witnessed CA and bystander CPR in the TTM2 population are remarkably higher than what is seen in clinical practice, with latest global data reporting that only 35–40% of patients who suffer OHCA receive bystander CPR [43,44,45]. Patients who do not receive bystander CPR and have longer “no-flow” times will generally present with more severe HIBI, and could potentially benefit the most from temperature control. However, the patients included in TTM2 had shorter “no-flow” times and higher rates of bystander-initiated CPR, potentially blunting the benefits of targeted hypothermia. Additionally, over 70% of recruited patients had shockable rhythms, cardiac or presumed cardiac etiology—with over 40% of ST elevation myocardial infarction—and only 28% presented with shock on admission; these facts demonstrate that the cohort is representative of a very specific subgroup of CA patients.
Most recently, the CAPITAL CHILL trial addressed the question of whether an even lower temperature target would be more beneficial for neurological recovery. The trial randomly assigned adult patients to a targeted temperature of 31 °C or 34 °C for 24 h, and demonstrated that a lower temperature goal of 31 °C did not improve outcomes compared to the standard of care targeted temperature of 34 °C. It is important to note that this was a single-center study and likely underpowered [46].
Another challenge interpreting this body of evidence is the inclusion of very broad patterns of brain injury leading to heterogeneity in the effects of temperature control at different targets and durations. As multiple authors have previously discussed, there are likely numerous brain injury phenotypes after CA, and neuroprotective interventions should likely be tailored to each individual brain injury target [47, 48]. If this differentiation of HIBI phenotypes is not carried out, therapies will likely fail as they are not being employed in the patient population most likely to benefit from them.
From Bench to Bedside: Integrating Temperature Control Evidence into Clinical PracticeTiming of Initiation
The post hoc analysis of the Continuous Chest Compressions trial showed that faster door-to-temperature control times were associated with better outcomes, particularly if within 122 min of admission. This trial supported the hypothesis that shorter times to temperature control initiation in OHCA patients increases the likelihood of a favorable neurological outcome [49]. However, given the retrospective nature of the study, as well as wide variability in temperature control initiation timing, cautious data interpretation is advised. Two RCTs have shown that pre-hospital cooling with cold saline infusion, as opposed to temperature control upon arrival to the treating hospital, confers no added benefit and, in fact, can cause a higher rate of early re-arrests [50, 51]. This is likely due to the decreased coronary perfusion caused by cold intravenous fluids [52], as well as pulmonary edema [50, 51]. Intra-arrest temperature control has been another area of interest, as pre-clinical studies in animal models showed promising results and, theoretically, prompt initiation of temperature control would mitigate even primary brain injury [32, 53,54,55,56]. Both the PRINCESS and RINSE trials showed that intra-arrest cooling in OHCA patients did not impact overall either neurological outcomes or survival rate, compared to temperature control after hospital admission, and this practice could even potentially decrease the rate of ROSC in initially shockable rhythms [52, 57]. However, a pooled analysis of these trials suggested a potential benefit of intra-arrest transnasal evaporative cooling in the subset of patients with shockable nonperfusing rhythms [58].
In a post hoc study of the TTM2 trial, no association of faster time to target 33 °C was noted with outcomes, challenging the critique that achievement of hypothermia earlier in the TTM2 trial could have altered the trial results [59].
Temperature control should be initiated as soon as possible after ROSC; however, there is insufficient data to support induction of pre-hospital cooling [9, 60].
Methods for Temperature Control
There are several pharmacologic and nonpharmacologic cooling methods employed to achieve target temperature. The most widely used are surface cooling devices, such as external gel pads containing cold water placed on the skin, and intravascular devices with a closed-loop feedback system that allow for more precise and controlled temperature control [36]. Infusion of cold saline intravenously is no longer recommended.
Due to their pragmatic nature, clinical trials in temperature control have been agnostic to the type of devices for temperature modulation. Several recent meta-analyses have demonstrated that intravascular cooling leads to better neurological outcomes compared to surface cooling, likely due to the intravascular route being more precise in maintaining the desired temperature, causing less temperature variation and being less associated with shivering [61, 62]. Several studies that evaluated surface cooling did not indicate whether temperature feedback was utilized [62]. It is also important to consider the possible complications of each method. The most common adverse events associated with surface cooling are skin injuries, such as tears and decubitus ulcers, whereas thrombosis, hemorrhage, and infections are prominent in intravascular cooling, as expected with central access [63,64,65]. While patient-specific factors could influence the selection of the method for temperature control (e.g., those with higher risk for thrombotic complications could benefit from external pads), most commonly the decision hinges upon the availability of the method in each institution.
Temperature Target Selection
Although it is imperative to actively control temperature and prevent fever in post-CA patients, the ideal target temperature for each CA phenotype has yet to be elucidated. It is quite possible that in the future individual factors leading to distinct injury phenotypes may influence the ideal temperature target [50, 66, 67]. In fact, five distinct phenotypes of post-CA brain injury were identified in a large retrospective cohort using unsupervised machine learning[47]. These phenotypes were determined based on features of neurological exam, EEG, and neuroimaging. The heterogeneity that exists within this patient population is reflective of the need for personalization of resuscitation efforts, such as temperature control strategies. However, more research is needed to better elucidate these findings, and to support the recommendation of different target temperatures for specific phenotypes.
While guidelines recommend a target temperature of 32–37.5 °C for at least 24 h after ROSC, there is no set temperature that has been proven to show more benefit over another, and the selection tends to be patient-dependent. A recent Bayesian meta-analysis determined that temperature control at 32–34 °C as compared to temperatures over 36 °C did not lead to more positive neurological outcomes [68]. Furthermore, a network meta-analysis indicated that hypothermia at 31–36 °C compared to normothermia at 37–37.8 °C did not lead to increased survival rates or better outcomes, and was associated with a greater risk of developing arrhythmias [14]. Prior data suggest that a target temperature ~ 36 °C might be preferrable in those with bleeding, intracerebral hemorrhage, or hemodynamic compromise, all of which could be exacerbated by lower temperatures [7]. Furthermore, rewarming patients who are spontaneously hypothermic may have detrimental effects, and targeting lower temperatures to avoid rewarming may be considered[50]. A lower temperature of 33 °C may be desired in those at risk for worse neurological damage from severe HIBI [4, 50, 67], but may also be associated with increased risk of arrhythmias in patients with cardiac etiologies for CA.
Maintenance Phase
Once temperature control is initiated, core temperature should be measured using either an esophageal, bladder, or intravascular probe. It is discouraged to use a rectal, oral, or axillary probe, as core temperature measurements are not as accurate. As recommended by guidelines, the cooling phase (a constant temperature between 32 and 37.5 °C) should last at least 24 h after ROSC, with special attention to avoidance of fever (> 37.7 °C) for at least > 72 h after ROSC. In the TH48 trial, extending temperature control at 33 °C for 48 h conferred no additional benefit over 24 h [69] on neurological outcomes at 6 months. The extended duration arm was associated with increased adverse events (although most of these appeared to be mild) as well as longer ICU length of stay. Until further data from large RCTs are obtained, target temperatures should be maintained for 24 h.
Rewarming Phase
The rewarming phase should occur at a rate of 0.15–0.25 °C/h, as rapid rewarming could cause an increased inflammatory response and potentially worsen outcomes [70, 71]. However, these rates of rewarming are extrapolated from study protocols from RCTs in temperature control evaluating target temperatures, and not based on large trials comparing different arms with rates of rewarming. To date, only ISOCRATE has explored the potential impact of slower rewarming rates, in a pilot study that failed to demonstrate a change in IL-6 and neurofilament light chain levels with 0.25 °C/h compared to 0.5 °C/h [72]. Hence, the ERC/ESICM guidelines make no recommendations on a specific rewarming rate [



留言 (0)