This protocol is registered with the International Prospective Register of Systematic Reviews (PROSPERO) database (reference number CRD42021290542) [14]. We report this protocol in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) (see Additional file 1) [15].
Eligibility criteriaStudy design
Any randomized control trial (RCT) reporting the QoL of AF patients following an eligible rate or rhythm control intervention will be eligible for inclusion.
Population
Studies that include adult patients aged 18 years or older with AF will be considered eligible.
Interventions
The following rate and rhythm control strategies will be included: pacing, atrioventricular (AV) node junction and bundle of HIS ablation, pharmacological therapy, radio frequency catheter ablation, cryoablation, pulmonary vein (PV) isolation, maze operation, pace maker implantation, and defibrillator implantation.
Comparators
Any of the aforementioned interventions will also be considered as eligible comparators.
Outcome measures
QoL irrespective of the tool used will be the only eligible outcome.
Search strategy
The Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, and Embase via OVID and CINAHL (Cumulative Index to Nursing and Allied Health Literature) will be searched for eligible studies. Additional file 2 contains an example of the search strategy in MEDLINE. The following trial registries will additionally be searched: WHO International Clinical Trials Registry Platform, ClinicalTrials.gov, and ClinicalTrialsRegister.eu. References of all included studies will be assessed for additional eligible studies not identified within the search.
The search strategy was developed using a combination of keywords and index terms. Key terms such as “atrial fibrillation,” “quality of life,” “rate control,” and “rhythm control” will be entered. There will be no restriction on language or setting. Publication date will be restricted to 2004 or later; this will allow for a 1-year overlap with the search date from the systematic review conducted by Thrall et al. (i.e., January 2005) [11] to ensure we include any studies missed in the 2006 published review due to delays in adding to databases or indexing within them. Studies that are included in the 2006 review will be included in our review if they meet the eligibility criteria.
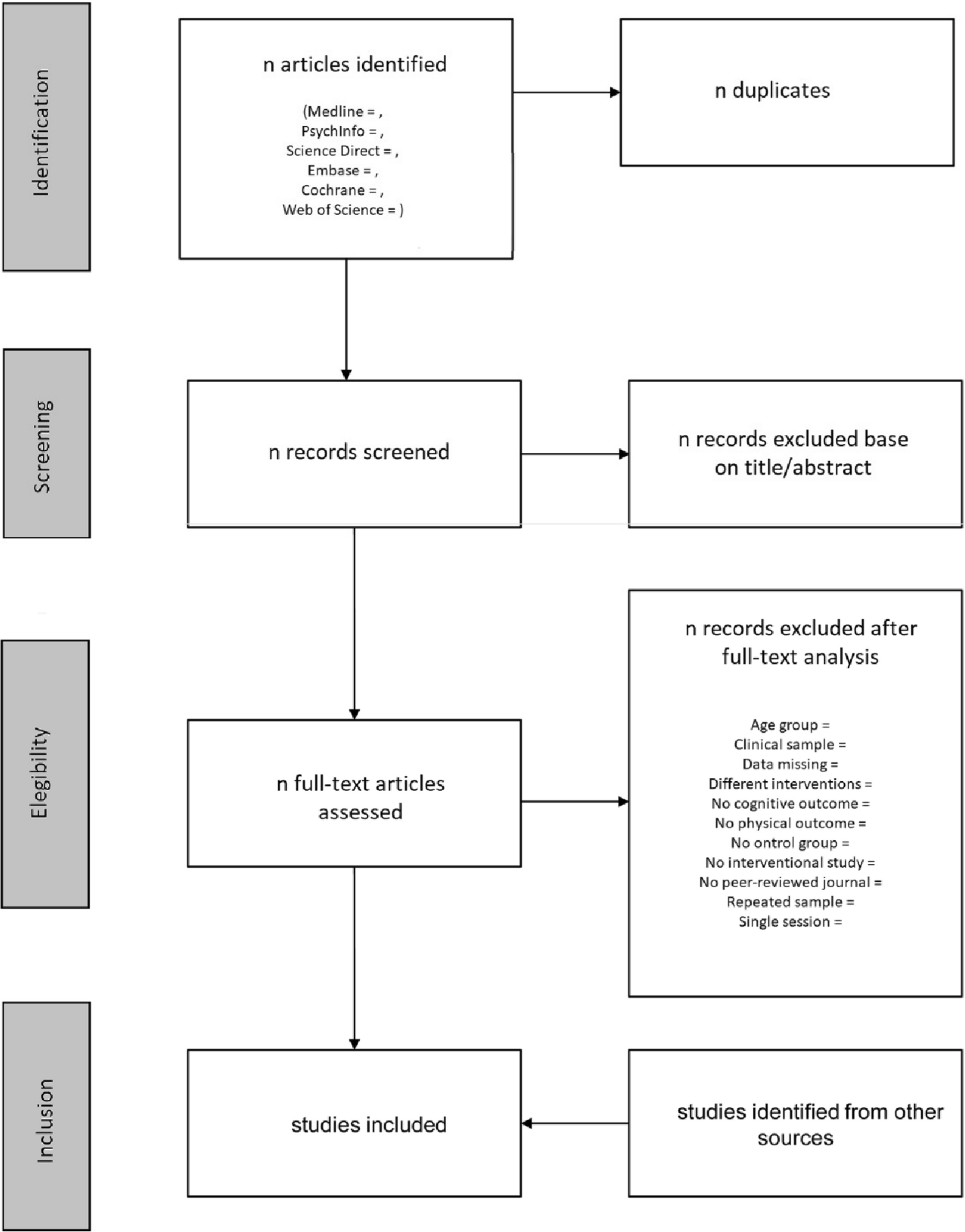
Citations of all identified studies from the search strategy will be exported to Rayyan [16]. Duplicate citations will be removed using the automated features of Rayyan. Titles and abstracts will be assessed independently by two reviewers (PU and SK). The same two reviewers will independently assess the full text of any primary study that potentially meets the eligibility criteria. Any disagreements will be handled through discussion or a third reviewer when necessary (AS).
Data extraction and management
Relevant data will be extracted from included studies using a piloted extraction tool in Excel. Data will be extracted by two reviewers independently (PU and SK); the data will then be cross-checked for accuracy.
The following information will be recorded:
Study characteristics (title, authors, journal, publication date, study period, number of participants, country, any conflicts of interest, and funding source)
Study design/methodology (study type, recruitment strategy, trial arm assignment strategy, eligibility criteria, QoL measurement tool, and duration of intervention)
Study population characteristics (age, sex, type and duration of AF, and any comorbidities where available)
Interventions (rate and rhythm control strategies) and comparator used
Outcome (loss to follow-up, time points of assessment, QoL for intervention and control arms for each time point assessed; any results to statistical tests including any sub-group analyses)
We will contact the authors for any missing information. If there is no response after two attempts to contact, we will continue with the data available within the published article.
Risk of bias assessment
Two reviewers (UP and SK) will independently assess the risk of bias using the Cochrane Collaboration Risk of Bias 2.0 (RoB 2) tool, providing a judgment of low risk of bias, high risk of bias, or some concerns for the QoL outcome from each included study [17]. Overall judgment of bias will be made by assessing each study’s randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, selection of the reported result, and any other potential process that could result in bias (for example, blinding). Any disagreements will be settled through discussion or by a third reviewer (AS) where necessary.
Analysis plan
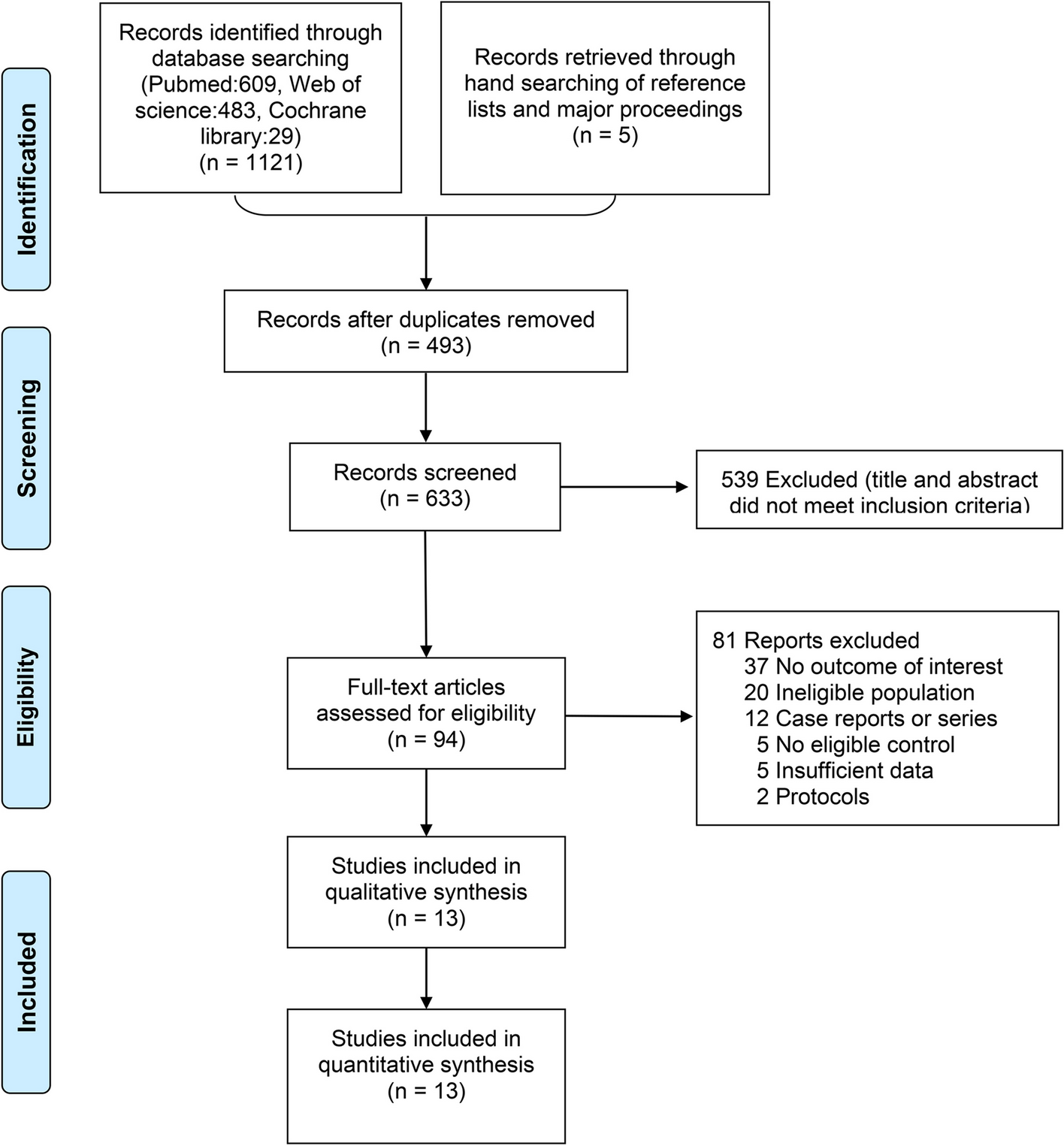
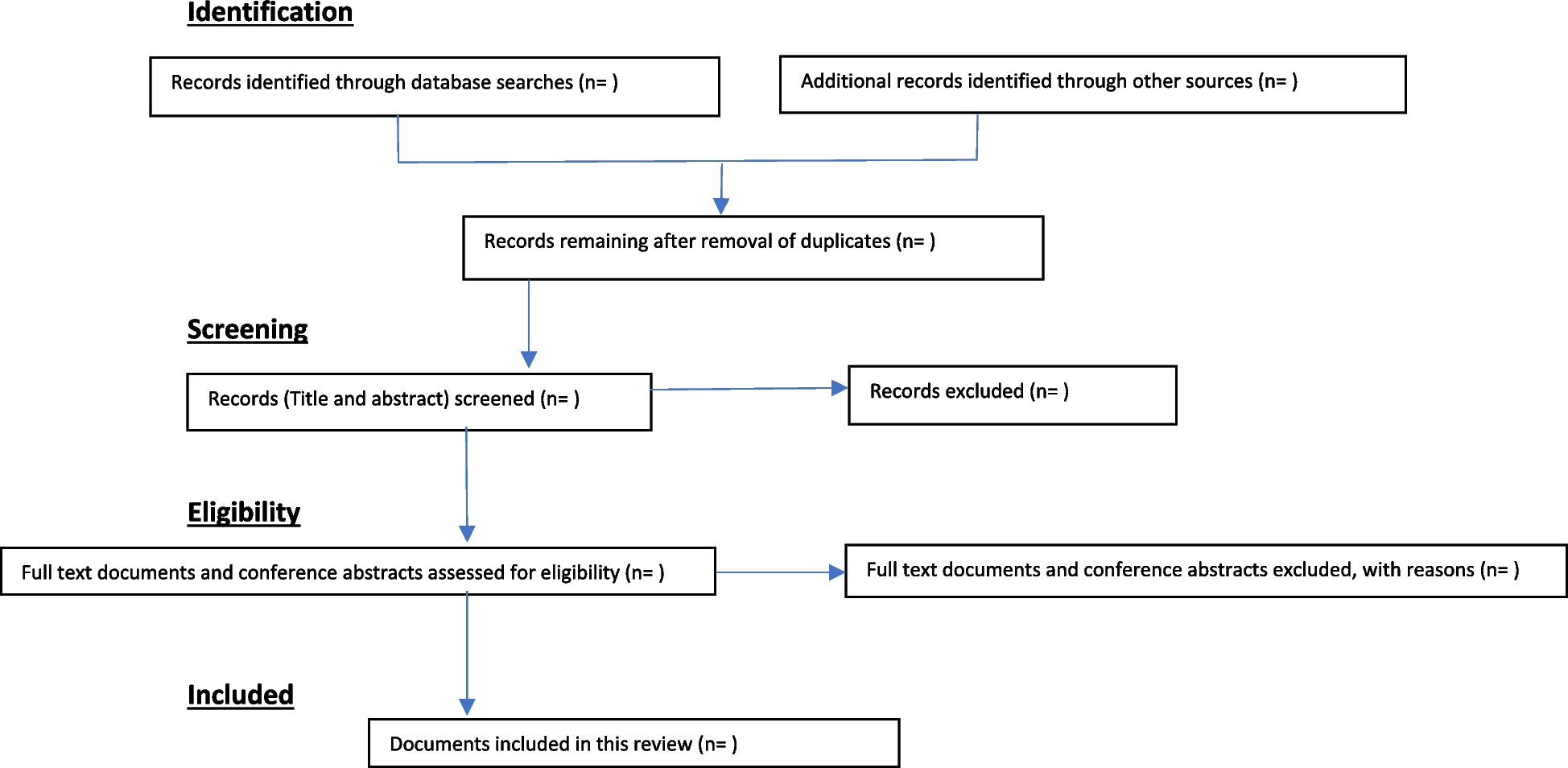
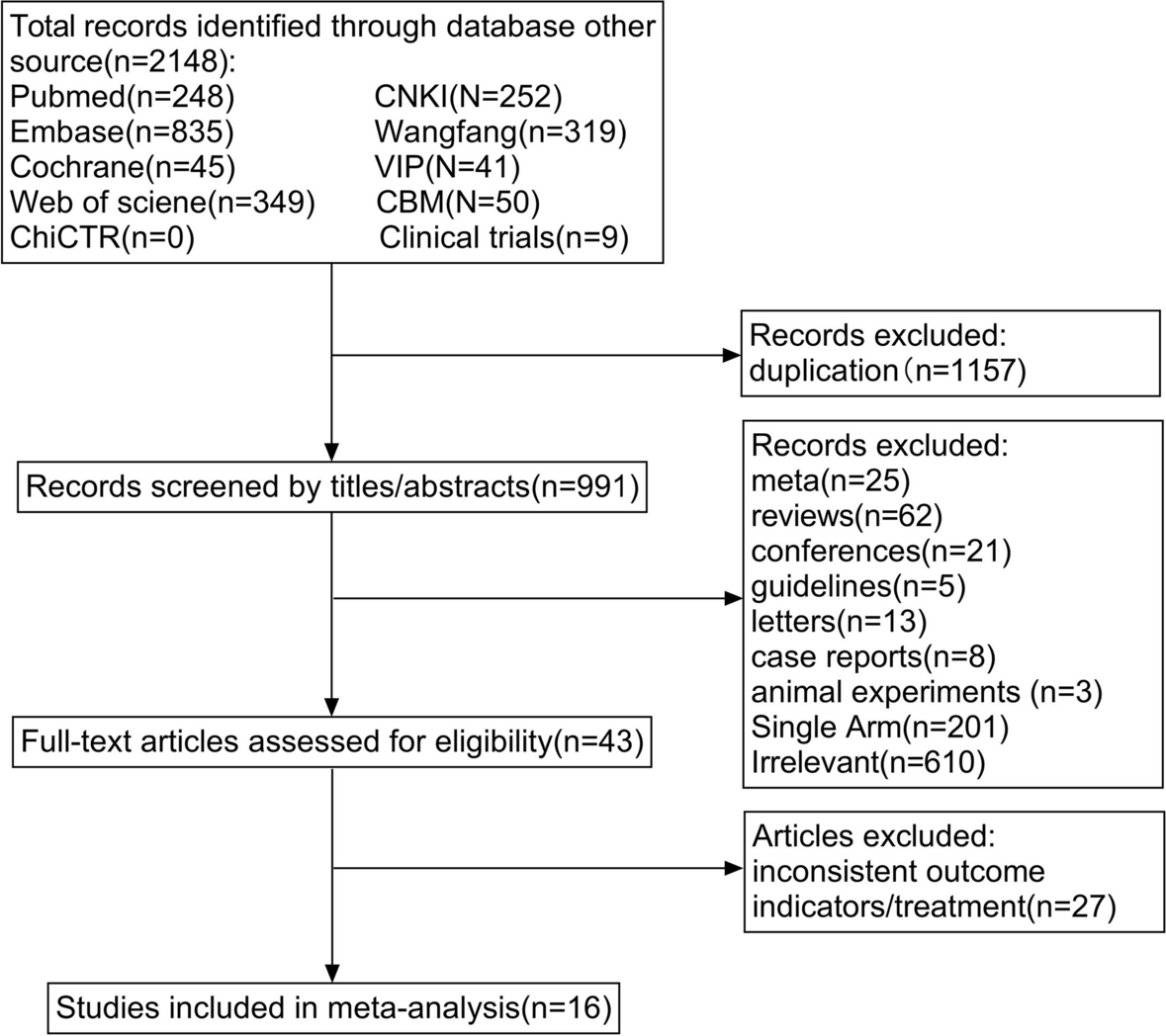
The study selection process will be summarized using a PRISMA-recommended study flow diagram [15]. A summary of findings table will present the characteristics of included studies along with reported outcome data relevant to our objectives.
Data will be managed in Excel and analyzed using Stata 14.0 (College Station, TX, USA). Continuous variables will be reported with mean and standard deviation and categorical variables with frequencies and percentages. Studies will be grouped by type of AF within the trial (paroxysmal, persistent, chronic, or permanent), intervention type, type of QoL assessment (generic or disease specific), and QoL tool used. The suitability of conducting a meta-analysis will be assessed by the clinical and methodological similarities of included studies. Any meta-analysis will use a pairwise random effects model due to the expectation that various tools will be used to assess QoL. If a meta-analysis is determined appropriate, the I
2 statistic and chi-squared test will be used to assess heterogeneity. If there is high heterogeneity (> 75%) and it appears to be from an outlier with an obvious bias (i.e., quality of study), a sensitivity analysis will be conducted (i.e., with low-quality studies excluded). A sub-group analysis for males and females will be conducted where feasible for rate and rhythm-control strategies separately. The effect sizes from each trial will be continuous and due to the expectation that different QoL tools will be used, standardized mean differences (SMDs) will be computed for any meta-analysis. Any pooled estimations of effect will be presented graphically as forest plots [18]. If there are 10 or more studies included in a meta-analysis, an assessment of the small study effect will be undertaken visually using a funnel plot. If a meta-analysis is not feasible, a qualitative synthesis of the results to each trial will be provided.
Level of certainty for the outcome of QoL for each included study and sub-group will be assessed using the Grading of Recommendation, Assessment, Development and Evaluation (GRADE) approach for systematic reviews. As per guidelines [19], we will critique the study limitations, inconsistency of results, indirectness of evidence, imprecision of findings, and other considerations that will contribute to the grading of the overall quality of evidence. The GRADE assessment results will be presented in the table of study characteristics as very low, low, moderate, or high. Explanations for any level other than high will be provided in the table footnotes.






留言 (0)