
記住我

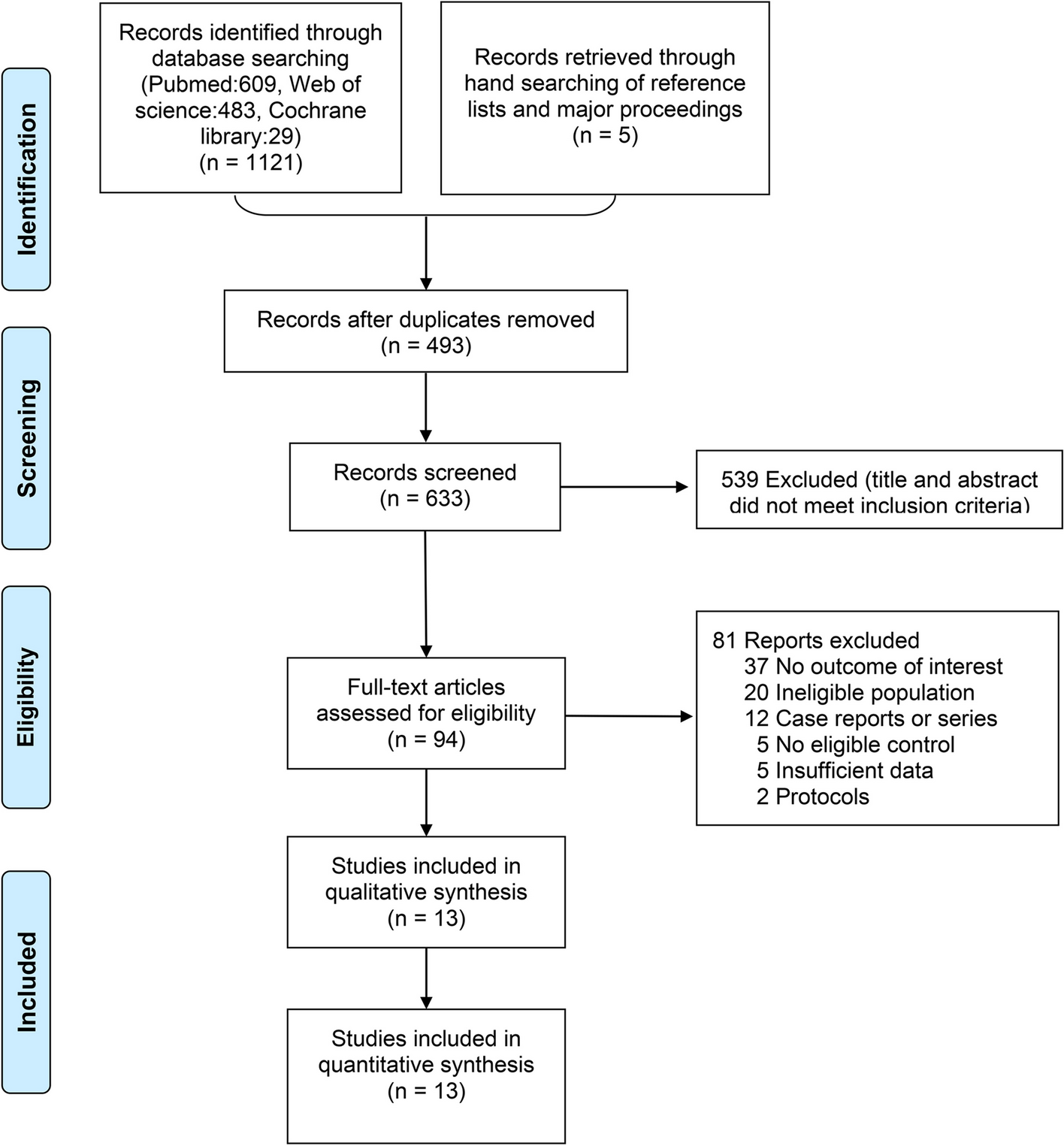



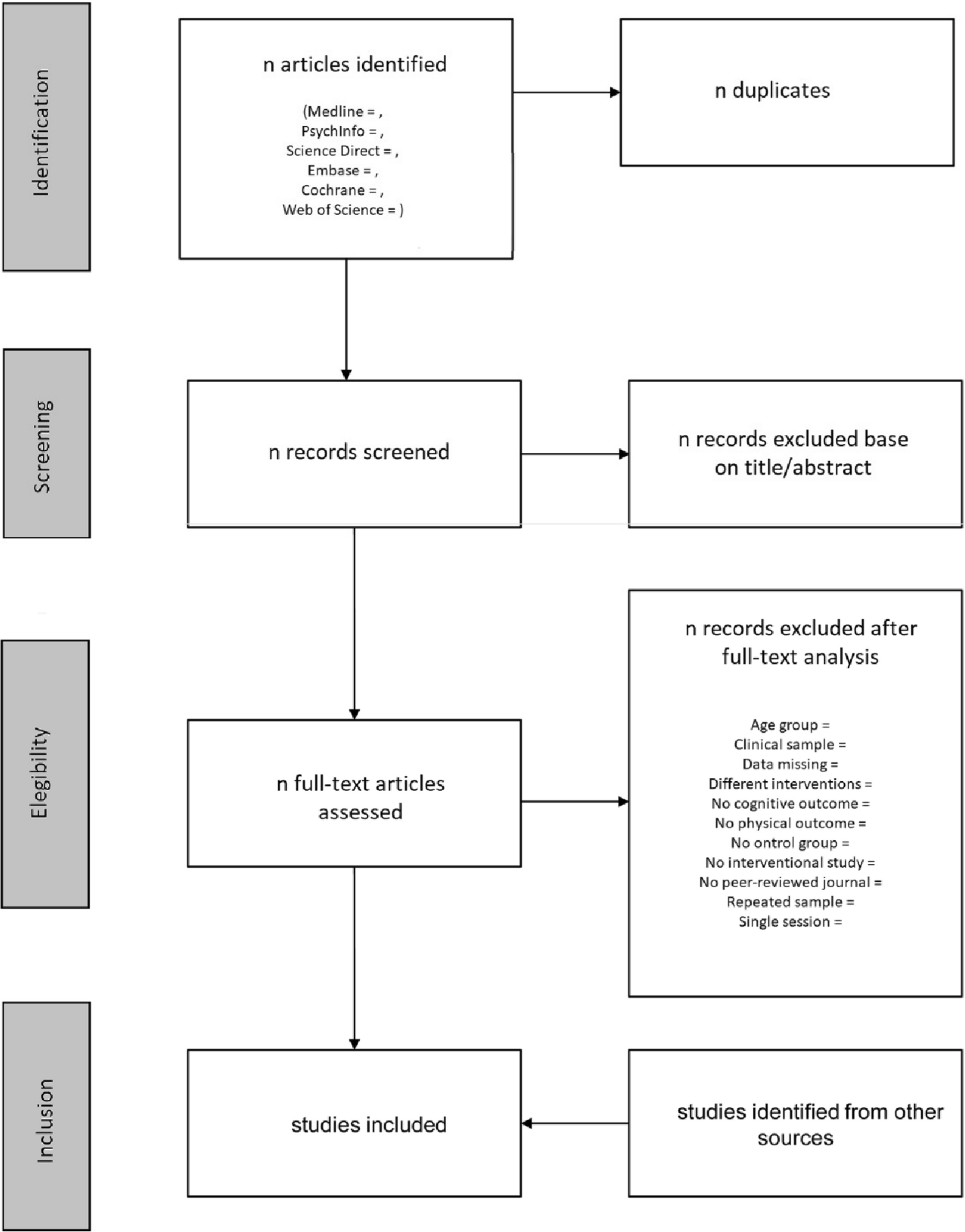

Of 7151 unique records retrieved by the searches for KQ1a and b, we assessed 163 for eligibility by full text and included five trials (4 randomized controlled trials [RCT] [4,5,6, 90], 1 controlled clinical trial [CCT] [68]) and two associated publications [91, 92] for KQ1a, and one RCT for KQ1b [93] (Fig. 1). Studies excluded after full text appraisal are listed with reasons in Additional file 5.
Fig. 1
Flow of records through the selection process. Legend: not applicable
Study characteristicsTable 3 shows the characteristics of the included trials for KQ1a. The trials were conducted in countries with a moderate-to-high baseline fracture risk [94]: Denmark (ROSE [5]), the Netherlands (SALT [4]), the UK (SCOOP [6] and APOSS [90]), and the USA (Kern CCT [68]). Aside from the Kern CCT, which included a relatively equal proportion of males and females ≥65 years old [68], the trials included populations of exclusively peri-menopausal (aged 45 to 54 years) [90] or postmenopausal (mean ages 70 to 75.5 years; range 65 to 90 years) [4,5,6] females. When reported, between 10 and 44% of the study population had a prior fracture [4,5,6]. The proportion of participants with a prior fracture was highest in the SALT trial (44%), which enrolled females who reported at least one clinical risk factor on the clinical FRAX tool [4]. Participants were not treatment-naïve in all trials; in particular, the APOSS trial allowed enrollment by females with past use of hormone replacement therapy [90] and 11% of participants in the ROSE trial were taking anti-osteoporosis medications at baseline [5].
Table 3 Characteristics of studies included for key questions 1a&b on the benefits and harms of screening versus no screening, and the comparative benefits and harms of different screening approachesThe three more recent trials (published 2018–2019) [4,5,6] employed a 2-step approach to screening, whereby all participants completed a mailed questionnaire including data to assess risk with the clinical FRAX tool, and only those surpassing certain risk thresholds were offered BMD assessment. The threshold for BMD assessment varied across trials; in the SALT trial, the entire population had ≥1 risk factor and were offered BMD and vertebral fracture assessment [4], whereas ROSE offered BMD for those with a clinical FRAX-based 10-year major osteoporotic fracture risk ≥15% [6], and SCOOP used age-based thresholds of 10-year hip fracture risk [5]. The two older trials (APOSS [2010] and Kern CCT [2005]) used a one-step direct to BMD screening approach [68, 90]. No trials included a true “no screening” comparator; in all cases, the comparator was usual care, with evidence of varying levels of ad hoc screening and treatment (median 17% treatment rate when this was reported, range 5 to 59% [4,5,6, 90]) within the comparison groups.
Thresholds for treatment were also variable across the trials. In both the SALT and SCOOP trials, BMD assessment was used to recalculate the 10-year FRAX fracture risk with inclusion of BMD, and treatment was offered when participants exceeded age-specific thresholds [4, 6]; the SALT trial also allowed for several other treatment indications according to Dutch guidelines (e.g., vertebral fracture) [4]. Of note, in the SCOOP trial, only 898 females exceeded a treatment threshold despite 3064 being considered at elevated risk based on fairly similar thresholds but without incorporation of the BMD results into the risk prediction by clinical FRAX. In the ROSE trial, treatment was offered when the BMD T-score at any measured site was ≤2.5, and/or a fracture was detected on vertebral fracture assessment [5]. In the two 1-step screening trials, treatment was offered to those in the lowest quartile of BMD, based on the first 1000 participants screened (APOSS) [90], and to those below the age-matched mean of the reference group according to the densitometer’s manufacturer (Kern CCT) [68]. Across the trials, between 7 and 25% of those assigned to screening had indications for treatment; the proportion was highest in the SALT trial, where higher-risk patients were enrolled [4]. The rate of treatment was lowest in the Kern CCT (31% of those with a treatment indication) [68]; among the remaining trials, more than two-thirds (69 to 80%) of those with a treatment indication reported using some form of anti-osteoporosis drugs during follow-up (variable treatments across studies, and sometimes including those such as calcitonin and hormone replacement therapy, which are no longer recommended; see Table 3). It was apparent that most of the treatment provided in the recent RCTs was pharmacologic, though at least one protocol (SALT) mentioned calcium and vitamin D supplementation, as well as notification of a high fall risk, that may have been acted upon by the primary care practitioner.
The trials provided data for hip fractures [4,5,6, 68, 90], clinical fragility fractures (described as major osteoporotic [4, 5, 90] or osteoporosis-related fractures [6]), serious adverse events [6], all-cause mortality [4, 6, 68, 90], and quality of life or wellbeing [6, 90, 92]; no trials reported on fracture-related mortality, functionality and disability, discontinuation due to adverse events, or non-serious adverse events. Though not directly reported, data were available in two trials to estimate the potential extent of overdiagnosis (see Additional file 3 for calculations) [4, 6]. Because of differences in design and reporting across the trials, we considered three possible population perspectives in our analyses. Two trials (APOSS and ROSE) provided data for an offer-to-screen population, whereby all eligible people invited for screening by mail, regardless of actual participation in any screening, were analyzed [5, 90]. The APOSS study also provided data for acceptors of screening, where the analysis included only those who attended for BMD measurement and thus completed screening. The SALT, ROSE, and SCOOP trials provided data for what we considered an offer-to-screen in selected population approach, because the analyses only included people who independently completed a mailed clinical FRAX questionnaire as part of 2-step screening [4,5,6]. The Kern CCT [68] also contributed data for this approach, as the sample population for screening was those already enrolled in the Cardiovascular Health Study (i.e., not the general population) [95]. We considered the “selected population” approach to be the one to be most applicable to primary care—where healthcare providers would complete risk assessment tools during the patient visit and then discuss the findings—although the participants in these trials are likely to be more accepting and compliant with screening, and possibly with treatment, than the general population presenting to primary care.
The risk of bias ratings for the included trials for KQ1a are in Table 4. The main risk of bias concerns were related to participant awareness of group assignments and contamination of the control groups in all trials (aforementioned ad hoc screening and treatment, likely to bias the findings toward the null) [4,5,6, 68, 90], and a high risk of attrition bias in the APOSS trial (42% lost to follow-up) in the offer-to-screen population [90]. The Kern CCT was not randomized, however patients were invited based on age- and sex-stratified random sampling and analyses were adjusted for baseline differences between groups [68]. We rated this trial, as well as the “acceptors” population for the APOSS and the “selected population” in the ROSE trial, to be at unclear risk of selection bias [5, 90], because in these analyses, the participants no longer represented the initially randomized population.
Table 4 Risk of bias assessments for trials included for KQ1a on the benefits and harms of screening vs. no screening, and KQ1b on the comparative benefits and harms of different screening approachesFindingsTable 5 summarizes the main findings for KQ1a; Additional file 3 contains the full GRADE Evidence Profiles and Summary of Findings Tables, with explanations for each rating as well as the forest plots, which include the results of statistical tests for subgroup differences. Among females aged 68–80 years, data from one trial showed that a mailed offer of screening in the general population may not reduce the risk of hip fractures, clinical fragility fractures, or all-cause mortality during 5 years of follow-up [5]. The evidence is very uncertain for all outcomes from a mailed offer of screening with BMD among females aged 45–54 years during 9 years of follow-up (1 trial) [90].
Table 5 Summary of findings for KQ1a on the benefits and harms of screening compared with no screeningAmong a selected population of females aged ≥65 years who are willing to independently complete a mailed fracture risk questionnaire, 2-step screening with risk assessment (clinical FRAX or FRAX-like tool) and BMD probably reduces the risk of hip fractures (3 RCTs + 1 CCT; n=43,736; 6.2 fewer in 1000, 95% confidence interval [CI] 9.0 fewer to 2.8 fewer; NNS=161) [4,5,6, 68] and clinical fragility fractures (3 RCTs; n=42,009; 5.9 fewer in 1000, 95% CI 10.9 fewer to 0.8 fewer; NNS=169) [4,5,6]. However, screening in this selected population probably does not reduce the risk of all-cause mortality (note: 1379 males were included in this analysis from the Kern CCT, representing 5.4% of the total sample) [4, 6, 68]. Our sensitivity analyses using assumed/baseline risks from a general Canadian population (age roughly corresponding to that of the trials) suggest that the effects for clinical fragility fracture may be larger than found in the trial populations, but these analyses are considered exploratory (Table 5). Post hoc subgroup analyses from the SCOOP study showed that the effectiveness of screening on hip fracture risk was greater in females with higher baseline clinical FRAX 10-year hip fracture risk (HR [95% CI] 0.67 [0.53–0.84] in the 90th percentile of risk vs. 0.93 [0.71–1.23] in the 10th percentile, p=0.021) and with prior fracture (HR [95% CI] 0.55 [0.38–0.79] vs. 0.87 [0.68–1.12], p=0.040 without prior fracture) [91]. The evidence for the effect of an offer of screening in a selected population of males is very uncertain [68]. In females aged 70–85 years, screening may make little-to-no difference in health-related quality of life [6]. Between 11.8% [6] and 19.3% [4] of females in a selected population offered 2-step screening may be overdiagnosed, but the magnitude of these estimates is of low certainty due to serious concerns of indirectness from lack of data provided as required for the proposed equation (e.g., mean risk in the high-risk population in SCOOP was limited to results of clinical FRAX without incorporation of BMD as used for treatment decisions) and from use of data from the SALT trial where participants were all at increased risk. Among females aged 70–85 years who are considered at high-risk by FRAX 10-year hip fracture risk alone and are referred to BMD assessment, data from one trial indicate that 24.1% may be overdiagnosed [6], but there is low certainty about this due to serious concerns about indirectness.
The evidence for hip and clinical fragility fractures among females aged 45–54 who accept 1-step screening with BMD measurement is very uncertain.
KQ1b: Does the effectiveness of screening to prevent fragility fractures vary by screening program type (i.e., 1-step vs. 2-step) or risk assessment tool?Study characteristicsAs indicated in the findings for KQ1a, one RCT (OPRA) [93] was included for the comparative effectiveness of different screening approaches. Characteristics of the OPRA trial are in Table 3. The trial included a mailed offer-to-screen population (acceptors of screening also available but less relevant to the primary care population). Eligible (n=9268; 34% participated) postmenopausal females were randomized to one of three screening approaches: 1-step screening using BMD via DXA; 2-step screening using the Simple Calculated Osteoporosis Risk Estimation (SCORE)-based tool, with BMD assessment offered when the score was ≥7 (74% eligible); and 2-step screening using the Study of Osteoporotic Fractures (SOF)-based tool, with BMD assessment offered to those with ≥5 clinical risk factors (7% eligible) [
留言 (0)