
記住我
Vaginal intraepithelial neoplasia (VaIN) is difficult to diagnose and manage and has substantial potential to evolve to invasive cancer. It is a rare disease, but as some patients are at increased risk, knowledge of the epidemiology, natural history, diagnosis, and treatment of VaIN is highly important for prevention of invasive vaginal cancer.
The European Society of Gynaecological Oncology (ESGO), the International Society for the Study of Vulvovaginal Disease (ISSVD), the European Federation for Colposcopy (EFC), and the European College for the Study of Vulval Disease (ECSVD) are leading international societies among gynecologists, pathologists, dermatologists, and other related disciplines. ESGO, ISSVD, EFC, and ECSVD have agreed to collaborate in order to produce a consensus statement on the management of pre-invasive vulvar and vaginal lesions. A consensus statement on the management of pre-invasive vulvar disease has been published already.1 This consensus statement focuses on the management of VaIN. The statement was accepted when consensus of at least two thirds of experts was achieved.
METHODSThe ESGO, ISSVD, EFC, and ECSVD Executive Councils nominated specialists among their members, whose expertise in improving the quality of care for patients with vaginal pre-invasive lesions has been previously confirmed. Five residents were invited to summarize the evidence available. Two external experts, internationally acknowledged for their research in vaginal pre-invasive lesions, were invited to review the final manuscript, before submission and external peer review.
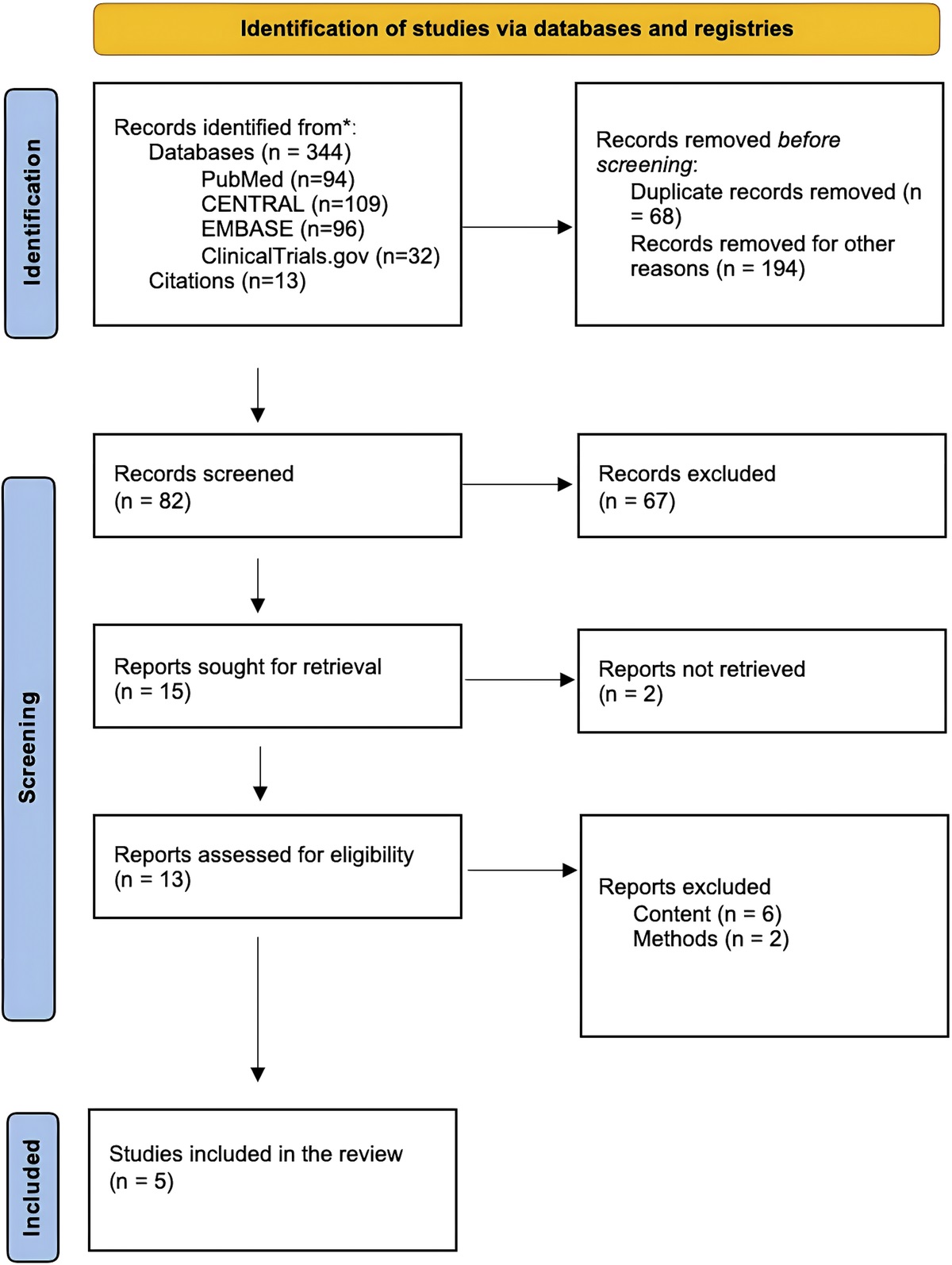
A systematic literature review of the studies published from January 2000 to April 2022 was carried out using the MEDLINE database. Search indexing terms and criteria are listed in an additional file (see Supplemental Digital Content 1, https://dx.doi.org/10.1136/ijgc-2022-004213). Priority was given to high-quality systematic reviews, meta-analyses, and randomized controlled trials. The search strategy excluded editorials, case reports, letters, and in vitro studies.
A total of 97 articles were retrieved dealing with VaIN. Data extraction was performed for all the articles on treatment by two independent teams with double-checking to ensure completeness. Tables with the most relevant clinical outcomes of 54 studies related to the treatment of VaIN were completed and summarized in the text (see Supplemental Digital Content 2, https://dx.doi.org/10.1136/ijgc-2022-004213). The other sections of this paper were drafted by one or more authors, with an independent literature search. A consensus was achieved between all the authors concerning the final version of the document.
Evidence-based consensus statements were also developed on the management of patients with VaIN, chaired by Vesna Kesic. The chair was responsible for drafting corresponding preliminary statements based on the review of the relevant literature (residents assisted in preparing data extraction and analyses: F.B., N.G., B.E.E., B.E.T.). These were then sent to the group of selected specialists. A first round of binary voting (agree/disagree) was carried out for each potential statement. The participants took part in each vote, but they were permitted to abstain from voting if they felt they had insufficient expertise to agree/disagree with the statement or if they had a conflict of interest that could be considered to influence their vote. The voters had the opportunity to provide comments/suggestions with their votes. The chairs then discussed the results of this first round of voting and revised the statements if necessary. The voting results and the revised version of the statements were again sent to the whole group and another round of binary voting was organized, according to the same rules, to allow the whole group to evaluate the revised version of the statements. The statements were finalized based on the results of this second round of voting. The group achieved consensus on 13 statements. One of the authors (F.P.) provided the methodology support for the entire process and did not participate in voting for statements.
Two external independent reviewers, internationally acknowledged for their research in VaIN, reviewed the final manuscript (M.K., S.R.).
Given the characteristics of this study, no ethical approval was considered necessary.
Evolution of Terminology and ClassificationsIn 2012, the Lower Anogenital Squamous Terminology (LAST) Project recommended a uniform two-tiered terminology for human papillomavirus (HPV)-associated squamous intraepithelial lesions (SIL) across all anogenital tract organs.2 It distinguishes between low-grade SIL (LSIL) and high-grade SIL (HSIL). The World Health Organization (WHO) 2020 terminology for precancerous lesions of the vagina parallels that of other organs of the female genital tract. SIL is the preferred terminology, accompanied by a synonymous use of the three-tiered system of intraepithelial neoplasia. LSIL encompasses HPV infection and VaIN 1, while HSIL includes VaIN 2 and VaIN 3. A very small percentage of invasive squamous cell carcinomas of the cervix and vagina may develop independent of an HPV infection.3,4 The current WHO classification from 2020 has not included HPV-independent cervical and vaginal cancer precursor lesions due to lack of citable publications at the time of publication.5
Colposcopic TerminologyAlthough the use of the colposcope is essential for the diagnosis of VaIN, the first colposcopic terminology of the vagina was published in 2011 by the International Federation for Cervical Pathology and Colposcopy (IFCPC)6 (Table 1).
TABLE 1 - 2011 IFCPC Clinical/Colposcopic Terminology of the Vagina General assessment Adequate or inadequate for the reason (ie, inflammation, bleeding, scar)IFCPC, International Federation for Cervical Pathology and Colposcopy.
This nomenclature provides a standardized pattern recognition and interpretation. Furthermore, it distinguishes type 1 (minor) and type 2 (major) findings. Atypical and fragile vessels and lesions with an irregular surface and ulceration are suspicious for invasive disease. The reliability of the 2011 IFCPC vaginal colposcopic terminology is between 69.2% and 82.5%.7–9
To increase the reliability of the pre-biopsy colposcopic diagnosis, investigators proposed to add a micropapillary pattern category8,9 and negative Lugol’s iodine solution test (Schiller’s iodine test)10,11 to the abnormal colposcopic findings. A course of local estrogen therapy is given to post-menopausal women, as it may help to distinguish between benign mimics of atrophy and true pre-neoplastic changes.12
In contrast to the cervical colposcopic terminology, the consistency between colposcopic patterns of VaIN and histopathology has been reported to be less accurate, with the vaginal histopathology frequently being worse than what was anticipated by the colposcopic impression.12,13
Epidemiology and Etiology of VaINVaIN (vaginal SIL) is a rare entity, accounting for only 0.4% of the female lower genital tract premalignant lesions. With an incidence of 0.2 to 2 per 100 000 women/year14–17 it is approximately 100 times less frequent than cervical intraepithelial neoplasia (CIN/SIL of the cervix).18,19 Despite a relatively stable incidence of vaginal cancers, the incidence rate of precursor lesions seems to have increased.20,21 This may be due to an improvement in the screening methods, as well as increased awareness of the condition.
The age-specific incidence rate of high-grade VaIN increases with advancing age until 70–79 years (1.5 per 100 000 woman years), after which it slightly declines. The incidence rate of high-grade vaginal lesions (VaIN 2/3; HSIL) was relatively stable during the total 20-year period but decreased significantly by nearly 16% per year among the youngest individuals (<30 years) in the period following licensure of the HPV vaccine.22
HPV Infection and OncogenesisThe large majority of vaginal neoplasms are HPV-associated squamous cell carcinomas that develop through VaIN (vaginal SIL). Low grade lesions of the vagina (VaIN 1; vaginal LSIL) are associated with both low-risk and high-risk HPV genotypes. In vaginal high-grade lesions (VaIN 2/3; vaginal HSIL), the most common genotypes involved are: HPV 16, HPV 33, and HPV 45.23 Individuals with risk factors for persistent HPV infection (eg, smoking, immunosuppression, HIV infection, history of cervical HSIL) have an increased risk for vaginal precancerous lesions and cancer,24–27 as well as vulvar, perianal, and anal lesions. The reported progression rate of VaIN towards invasive squamous cancer ranges between 2% and 7%.27–29
Vaginal precancer/cancer is also known to occur more frequently in patients with a history of pelvic radiation for other malignancies, such as cervical or endometrial cancer.30 The mechanism of HPV-independent carcinogenesis of the vagina is unknown.5 Vaginal adenosis may be the origin of the rare entities of vaginal adenoma and adenocarcinoma.31
Genetics of VaINLittle is known about the genetic risk factors for VaIN and vaginal cancer. Based on the current studies, no gene mutations associated with hereditary forms of vaginal cancer have been identified.
The persistence, progression, or regression of the HPV-induced lesions may depend, among other factors, on the host heritable immune response.32 Genetic factors may influence the susceptibility to cervical high-risk HPV (hr-HPV) infection.33,34 There are no specific studies of this kind concerning VaIN, but it is likely to be similar to what is known for the cervix.
Over the last three decades, numerous studies on gene association, using either the candidate gene approach or genome-wide association studies (GWAS), have been conducted in an attempt to identify genetic factors associated with persistent HPV infection and cancer development. It is suggested that a disruption in the apoptotic and immune function pathways plays a key role in the susceptibility to HPV-associated cancers.35 Epigenetic and in particular differential methylation events substantially contribute to the regulation of the papillomavirus life cycle.36 Methylated genes (CpG sites for cell adhesion molecule 1 (CADM1)), T-lymphocyte maturation associated protein (MAL), and the microRNA 124–2 (miR124-2) appeared to be promising biomarkers in HPV-related CIN.37 As indicative of underlying biological changes, they might become useful as markers of neoplastic transformation at other lower genital tract sites.38
Vaginal MicrobiomeStability and composition of the vaginal microbiome plays an important role in determining host innate immune response and susceptibility to infections, including HPV. Depletion of Lactobacillus species has been associated with the presence of hr-HPV infection and increases with disease severity.39–43 The rate of a Lactobacillus-depleted microbiome is only 10% in healthy individuals, while this increases two-, three- and four-fold in patients with CIN 1 (LSIL of the cervix), CIN 2/3 (HSIL of the cervix) and invasive cervical cancer, respectively.40,44,45 Furthermore, Lactobacillus depletion has been found to be associated with CIN progression or regression.46 This high diversity microbiome persists after surgical excision of CIN and HPV clearance, suggesting that this microenvironment may contribute to the susceptibility to HPV and is not caused by the infection.47 Similarly, patients with VaIN have increased abundance of several bacterial vaginosis-related bacteria.44
Potential mechanisms of vaginal microbiome influence are through changes in vaginal pH, bacteriocin production, mucosal disruption and epithelial integrity, oxidative stress, and effects on cellular targets such as p53, pRB, and survivin, synergistically with HPV.48 Future research on vaginal microbiota may reveal new important information for understanding the onset and biological behavior of VaIN.
Cytology, Histopathology, and ImmunochemistryWhile cytology can be helpful in the detection of vaginal pre-invasive lesions, in the individual who still has a cervix, the finding of dysplastic squamous cells, or metaplastic or glandular cells, does not necessarily indicate a diagnosis of VaIN or adenosis, as cervical contamination is possible. Thus, cytology is not considered a primary screening modality for these conditions. Vaginal cytology may also be utilized after therapy for follow-up of a treated vaginal lesion, as well as for follow-up of cervical pre-invasive and invasive disease in a patient who had a hysterectomy.
Immunohistochemistry is a useful tool for distinguishing between different types of vaginal pre-invasive lesions (Table 2).
TABLE 2 - Immunohistochemistry in Vaginal Pre-invasive Lesions Lesion Histochemistry/immunohistochemistry Comment HSIL (VaIN 2/3) p16 block positivity, Ki-67 extends above basal layers through the entire epithelium. p63 and p40 will confirm squamous origin, if in doubt Ki-67 will stain above the basal layers in LSIL as well and cannot be used to distinguish LSIL from HSIL. p16 is more useful in this distinction. Adenosis Mucicarmine or periodic acid shift (PAS reaction) with and without diastase will highlight mucin producing cells Pagetoid spread of urothelial intraepithelial neoplasia Positive cytokeratin 7, cytokeratin 20, p63, and GATA3 staining149 and uroplakin150 Exceptionally rare Paget disease Cells are positive for PAS-D, mucicarmine, CK 7, GCDFP-15, GATA3151 Exceptionally rare. Stains to distinguish secondary Paget disease of urothelial (including uroplakin150) or anorectal origin (including CDX-2, CK20152) should be considered in appropriate cases Melanoma in situ Positivity for s100, Melan-A, and HMB 45153 Exceptionally rare. A panel to distinguish melanoma in situ from Paget disease can be helpfulHSIL, high-grade squamous intraepithelial lesions; LSIL, low-grade squamous intraepithelial lesions; VaIN, vaginal intraepithelial neoplasia.
High-grade VaIN (VaIN 2/3, vaginal HSIL) is most often found in association with previous or current cervical neoplasia,49 and is cytologically and histologically identical to that of the vulva and cervix. Cytology focuses on increased nuclear to cytoplasmic ratio with irregular hyperchromatic nuclei. Histology shows maturation abnormality of the squamous epithelium at least two-thirds of the way up from the basement membrane. As in vulvar and cervical HSIL, the neoplastic cells have hyperchromatic irregular nuclei, and mitotic figures are often seen. p16 block positivity is an indicator of transforming hr-HPV infection and can be used to distinguish HSIL from its mimics, although LSIL is occasionally associated with hr-HPV and might show block positivity. Ki-67 immunohistochemistry will distinguish SIL from non-SIL, by extending above the basal layer, but this staining pattern will not distinguish LSIL from HSIL. Neither LAST2 nor the 2018 International Federation of Gynecology and Obstetrics (FIGO) staging for vaginal cancer describes criteria for a superficially invasive lesion.50
Clinical AspectsVaginal intraepithelial neoplasia is an underdiagnosed disease. Due to the absence of symptoms, it is more often diagnosed after a positive cervical cytology and/or HPV test in the absence of cervical intraepithelial neoplasia on colposcopy and/or biopsy, or during follow-up of patients previously treated for cervical disease.
Individuals at higher risk for development of VaIN are those:
With a history of cervical cancer or cervical HSIL51,52 Who had a hysterectomy for cervical HSIL53 Who had previous irradiation for gynecological cancer30 Immunosuppressed individuals54 Post-menopausal individuals51 Diethylstilbestrol (DES) exposed patients.55 CytologyMost vaginal lesions are diagnosed as a result of an abnormal cervical screening test. Individuals who have a positive cytology in the absence of cervical pathology should be surveyed for the presence of vaginal lesions. Cytology is sensitive (67.5–76.2%) and more reliable than colposcopy for detecting vaginal lesions.56 When combined with hr-HPV tests, it can improve detection accuracy up to 95%.57
Colposcopic Assessment of the VaginaThere is often no gross identifiable lesion in the vagina during visual inspection. Therefore, the examination of the vagina using a colposcope is essential. It requires not only the usual application of 5% acetic acid, it must include the complete visualization of the vaginal walls and folds. The vaginal folds make it difficult to detect all suspicious areas because the lesions may be hidden between the mucosal folds of the vagina and between the cervix and vaginal fornices (Figure 1). When undertaking examination, it is important to rotate the speculum with the blades opened through 360 grades.
 FIGURE 1:
FIGURE 1: VaIN 3 (vaginal HSIL) on the posterior vaginal wall and between folds of the vaginal cuff. HSIL, high-grade squamous intraepithelial lesions; VaIN, vaginal intraepithelial neoplasia.
Colposcopic assessment of the vagina is complicated by several problems:
The field to be examined is large It is difficult to see most of the changes at a right angle The colposcopic patterns can be less specific than in the cervix Following hysterectomy, affected areas may not be readily visible at the oversewn vaginal vault including the lateral ‘dog-ears’ Pre-invasive disease is often multifocal It is important to differentiate LSIL from truly premalignant lesions (HSIL) to avoid overtreatment.After the application of acetic acid, vaginal HSIL is usually aceto-white with sharp borders and a granular surface appearance. Occasionally, a punctation pattern can be seen. Mosaic or keratosis are rarely found (Figure 2).
 FIGURE 2:
FIGURE 2: CIN3 (cervical HSIL) extending to anterior vaginal wall (VaIN 3/vaginal HSIL). CIN, cervical intraepithelial neoplasia; HSIL, high-grade squamous intraepithelial lesions; VaIN, vaginal intraepithelial neoplasia.
Similar to other sites, atypical and fragile vessels, and lesions with an irregular surface and ulceration, are suspicious for invasive disease58 (Figure 3).
 FIGURE 3:
FIGURE 3: Invasive cancer at vaginal cuff after hysterectomy for cervical HSIL. HSIL, high-grade squamous intraepithelial lesions.
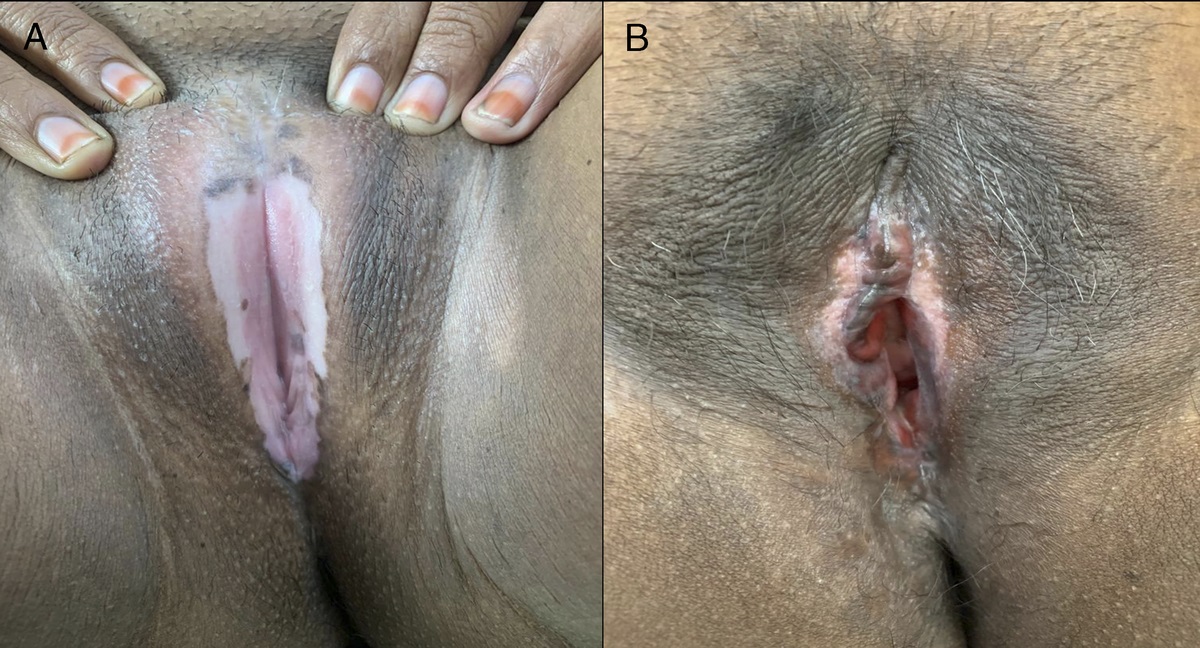
The application of Lugol’s iodine solution (Schiller’s test) is important in colposcopy of the vagina. Colposcopically, VaIN may present as iodine-negative epithelium only, similar to what is observed on the cervix in some cases58 (Figure 4). In post-menopausal patients with a marked atrophy of the vaginal mucosa the interpretation of Schiller’s iodine test may be difficult. The application of a topical estrogen for up to 3–4 weeks before the exam is recommended.
 FIGURE 4:
FIGURE 4: VaIN 3 (vaginal HSIL) (A) after the application of acetic acid, and (B) after staining with Lugol’s solution. HSIL, high-grade squamous intraepithelial lesions; VaIN, vaginal intraepithelial neoplasia.
Histology obtained by biopsy is the gold standard for the diagnosis. The 2020 WHO classification is used to determine the treatment.5
ManagementThere is no unanimous agreement on which is the best method of the treatment of VaIN. Treatment should be individualized, based on characteristics of each patient, disease, and previous therapeutic procedures. The choice of the treatment depends on:
Patient characteristics (age, parity, immune status, sexual activity) Type of the lesion (severity and site of the lesion, extent of the disease, multicentricity) Previous treatment (treatment of VaIN, hysterectomy for HSIL of the cervix, previous irradiation).Vaginal atrophy may create diagnostic difficulties related to colposcopic assessment and may be the cause of overreading of vaginal cytology. Therefore, histological confirmation of vaginal neoplasia is necessary before treatment planning.
Low grade lesions of the vagina (HPV changes/VaIN 1; vaginal LSIL) are considered expressions of HPV infection with a low risk for progression and a high potential for spontaneous regression. Studies including the observational approach of VaIN 1 have shown that it spontaneously regressed without treatment in 48.8–88% of cases.57,59–62 Lesions not associated with HSIL of the cervix or vulva tend to have higher spontaneous regression (91%) than those associated with cervical or vulvar HSIL (67%), suggesting different biologic behavior.61
There is evidence that treatment does not lead to better clinical outcomes in patients with VaIN 1.63 As such, low grade lesions can be safely managed by observation.64 Continuous surveillance is warranted due to the frequent emergence of recurrence even after treatment with laser or excision (24.3% and 22.2%, respectively).59
High-grade lesions of the vagina (VaIN 2/3; vaginal HSIL) have premalignant potential and should be treated. Studies of patients with HSIL of the vagina who were monitored without any treatment reported progression to invasive cancer ranging from 9%61 to 50% of cases.65
A wide spectrum of modalities has been used to treat VaIN. Traditional methods, vaginectomy and vaginal irradiation, are nowadays used only in highly selected cases of extensive and persistent disease. Both treatments cause significant morbidity that greatly worsen the quality of life.14 More conservative options such as local excision, laser ablation, and medical therapy with topical agents are useful as first line treatments, especially in young patients and for multifocal disease. Conservative treatment aims to ensure maintenance of the functional anatomic structure, preserving the elasticity, capacity, and extension of the vagina. Each treatment modality has advantages and disadvantages to be discussed with the individual patient.
Surgical InterventionsSurgical methods used for treatment of VaIN include both excisional and ablative techniques. Cold knife, carbon dioxide (CO2) laser, cavitational ultrasonic surgical aspiration, and electrosurgical loop excision are usually used for excision, while CO2 laser vaporization, photodynamic therapy, and electrocoagulation (fulguration) have an ablative effect.
Excisional MethodsExcisional methods are preferred because they provide a specimen for a complete histopathological diagnosis and permit the identification of underlying invasive cancer. Pre-operative colposcopic assessment of the vagina to identify the extent of VaIN should be done to ensure adequate excision and avoid residual disease. The uneven surface of the vagina makes it difficult to accurately assess the length of surrounding tissue to be removed.
Wide local excision is associated with the lowest risk of recurrence, but it is limited in applicability because SIL of the vagina is frequently multifocal. The reported residual disease rate after excision ranges from 8.6%66 to 18.9%.67
The success rate after surgical excision of VaIN is high, ranging between 66% and 81%. In a study of 35 patients with VaIN 3 treated by wide local excision, 23 patients (66%) were free from disease at a median follow-up of 44 months.66 More recently, a study exploring the outcome of ‘vaginal stripping’ in VaIN 3 found that 90 out of 111 (81%) patients were disease-free after a median follow-up of 76 months. The vaginal stripping procedure was performed as the combination of sharp and blunt dissection used for en bloc removal of the mucosa of the upper vagina, followed by cauterization to achieve hemostasis. Apart from short-term complications such as hemorrhage or infection evidenced in 4% of patients,67 this procedure may result in other complications which include shortening or stenosis of the vagina.
CO2 laser therapy is used for both local tissue excision and ablation. This method enables easier treatment of multifocal disease with limited morbidity. Pain and bleeding are the most frequent complications. In a large retrospective series of 128 cases of VaIN 3 treated with CO2 laser excision only, the overall rate of complication was 7.8% (mostly vaginal bleeding). There was only one (0.8%) major complication (vaginal vault perforation).68 Laser excision is usually combined with other modalities for treatment of VaIN. Laser excision should be performed only by expert specialists to avoid tissue damage and intra-/post-operative complications.17
Partial upper vaginectomy is considered the treatment of choice in high-grade VaIN (vaginal HSIL) at the apical part or in the region of the vaginal cuff scar.69 In cases of multifocal lesions or those that involve the lower one-third of the vagina, upper vaginectomy can be combined with laser vaporization.70
In a retrospective review of 33 patients with VaIN 2/VaIN 3 extending between 20–100% of the vaginal surface treated by single laser skinning vaginectomy, Luyten et al achieved a cure rate of 87.0%. The vaginal epithelium, including all lesions, was excised in one piece with a depth of 2–3 mm. No serious adverse events related to the procedure were recorded. After follow-up of 23 patients for at least 12 months, moderate shortening of the vagina was observed in two patients and another two required treatment of vaginal strictures.71
Similar cure rates were reported in two studies of patients who underwent partial (upper) vaginectomy for VaIN 3, 84% and 88%, respectively.70,72 Post-operative complications ranged from none to 3.5%.
Total vaginectomy is not an advisable procedure because it makes sexual intercourse impossible and thus it must be reserved for exceptional cases, when the spread of recurrent lesions cannot otherwise be managed or in cases of a short vagina post-hysterectomy. The complications of total vaginectomy could be decreased with adequate patient selection and meticulous surgical procedure.73
Cavitational ultrasonic surgical aspiration (CUSA) is a safe and effective option for VaIN, with effectiveness similar to classical surgery. Ultrasonic surgery allows exact removal of epidermal or mucosal lesions without thermal or mechanical damage to the surrounding structures or underlying stroma. It is a minimally-invasive procedure which requires general or spinal anesthesia. However, CUSA requires expensive equipment, training, and is not available in most settings.
After a median follow-up period of 4.5 years, the cure rate in 92 patients who underwent CUSA for VaIN was 80.4%.74 There are no reports of adverse effects in patients treated with CUSA.
In a study involving 46 patients treated with CUSA for recurrent disease, a significantly greater proportion of those who were treated with CUSA had no further recurrence (52%) compared with patients treated with other methods (9%) (p<0.001).75 Similar effectiveness was reported for the treatment of recurrent disease (50%).74
The loop electrosurgical excision procedure is not a treatment of choice for vaginal lesions due to the difficulty in controlling the depth of excision. Deep necrosis is reported as one of the possible late complications.76
Still, the loop electrosurgical excision procedure has been reported in treating upper vaginal vault VaIN.77 When the loop electrosurgical excision procedure was used for the treatment of 23 patients with histologically confirmed VaIN (VaIN 1–3) a complete response rate of 86.96% at 12 months of follow-up was reported, while at 24 months of follow-up it was 75%.78 The advantage over knife, laser, or diathermy excision is not clear.
Ablative MethodsThe major disadvantage of using ablative methods for the treatment of VaIN is the risk of missing an invasive cancer, since they do not provide tissue specimens for histopathological evaluation. Occult invasive cancer has been reported in 2.6–30% of patients.16,62,67,68,71,79
Special attention is needed in patients with prior hysterectomy for cervical HSIL extending to the upper vaginal vault scar. In these cases, a buried residual lesion (VaIN or occult cancer) cannot be reached by local ablative treatment (Figure 5).
 FIGURE 5:
FIGURE 5: VaIN 3 (HSIL of the vagina) buried within the vaginal cuff. HSIL, high-grade squamous intraepithelial lesions; VaIN, vaginal intraepithelial neoplasia.
For this reason, ablation should not be performed if the entire area of abnormal epithelium cannot be visualized or if there is any suspicion of invasion on colposcopic assessment, with multiple biopsies recommended before ablation to rule out an invasion.
When using ablative techniques an attempt should be made to achieve a depth of destruction to include epithelium affected by VaIN, because it directly relates with the outcome of the treatment. Exploring the depth of the involved and non-involved vaginal epithelium in 246 patients with VaIN, Cui et al found that the thickness of the lesion was generally <1 mm for patients of all ages, except in rare cases of visible lesions with papillary hyperplasia. The mean thickness of the epithelium involved was 0.4 mm and it did not differ between the grades of VaIN.80
CO2 laser vaporization can be performed under local anesthesia. Epithelial destruction to a depth of 1–1.5 mm, including the zone of thermal necrosis, seems to be sufficient to destroy the epithelium containing SIL, without damage to the underlying structures. Larger spot sizes and the superpulse mode are used to avoid deep penetration and the conduction of excessive heat.
Reporting the treatment of 65 patients with all grades of VaIN by laser vaporization, Jentsche et al confirmed relapse of the disease in 57 % cases.81 Cure rate in patients treated once with CO2 laser vaporization for high grade (VaIN 2/3) is between 73.5%59 and 86%.82–84 In a study involving 24 patients with VaIN 3, the lesion was completely eliminated in 17 (70.8%) patients after one session of treatment, and 19 (79.2%) required multiple sessions.85
Disadvantages of laser vaporization include an inability to treat buried vaginal cuff epithelium and technical difficulties in applying the laser to a distorted space within vaginal foldings. Also, expensive equipment, technical support, and surgical expertise are required, which are not easily available in all centers.
Photodynamic therapy (PDT) is an ablative, highly selective, and effective method for treating intraepithelial lesions and HPV lesions of the lower genital organs. It combines a medical and physical approach, which relies on a photosensitizer. The photosensitizer (5-aminolevulinic acid (ALA)) is selectively absorbed by abnormal cells and can be activated by light at a specific wavelength to produce singlet oxygen, which kills the target cells.86,87 Only mild local adverse reactions were recorded (burning sensation, pain, slight discomfort in the lower abdomen, and increased vaginal discharge), which were bearable and resolved in 3–5 days after treatment. At the end of follow-up, both the cervix and the vagina of all patients had maintained their integrity with regards to anatomical structure and function.88
Evaluation of the efficacy and safety of ALA-PDT for treatment of hr-HPV-positive patients diagnosed with VaIN showed complete remission rates ranging between 88.64% and 90.9%.86,88,89 The HPV clearance rate ranged from 38.1%89 to 60.98% and 67.1% at 12 months of follow-up.86,88
Electrocoagulation (fulguration) has also been used in the therapy of VaIN. Diathermy can reach and control the desired depth of ablation of 1.5 mm. However, it is less precise than laser.
A retrospective study of 184 patients with VaIN whose main treatment was electrofulguration with focal resection showed a primary remission rate of 87.62%.90 It was also safe, with few complications. Some patients complained of discomfort after surgery.
Plasma energy ablation is an ablative technique which vaporizes tissues, similarly to CO2 laser ablation, with advantages in terms of safety and the need for training and expertise. Kinetic and thermal energy generated by this technology can dissect, vaporize, and coagulate tissue, in the same manner as the CO2 laser. In contrast with laser, the energy transferred with plasma ablation decreases rapidly with increased distance of the handpiece to the tissue, significantly reducing the risk of both fire and retinal injury.
After a median follow-up of 29.3 months of 41 patients treated for vulvar or vaginal HSIL, a similar rate of complications (4.8% vs 9.5%) and recurrence rates (33.3% vs 28.6%) were reported in the plasma and laser ablation groups.91 Plasma energy ablation is considered a viable alternative to CO2 laser ablation, which may be particularly important in countries with limited access to the latter.
Finally, proper selection of patients, but also the skills of the surgeon, have a significant influence on the outcome.62,92
Medical TherapyTopical application of therapeutic agents has the advantage of treating the entire vaginal mucosa with good coverage of multifocal disease and disease in folds and recesses of the vagina. However, local vaginal creams cannot reach buried epithelium in the vaginal cuff scar. Also the effect on the lower vagina may not be consistent when the cream is applied using a standard vaginal applicator. As with ablative methods, prior to medical treatment invasion must be ruled out.
Imiquimod is an immune response modifier that induces cytokines which stimulate the activity of natural killer cells, promotes maturation and activity of Langerhans cells, and increases the effectiveness of T-cell-mediated response.16,93
Being proved useful in the treatment of vulvar intraepithelial neoplasia, imiquimod has recently gained much interest for the treatment of vaginal lesions. Applied for persistent HPV infection after treatment of cervical or vaginal SIL (VaIN), after a median follow-up of 33.6 months, imiquimod led to cytological/histological regression and negative HPV in 51.4% of the 72 treated patients.94 Of the 26 patients with normal cytology but persistently HPV-positive tests for at least 1 year, a complete regression was achieved in 65.4%. Chen et al reported an even higher clearance rate of HPV: 76.3% of the 76 patients cleared the HPV infection and had a normal cytology following the use of imiquimod cream.93 In most cases of persistent HPV infection, the severity/grade of VaIN decreased following the use of imiquimod.
A very low dosing regimen of imiquimod 5% cream (0.25 g, once a week for 3 weeks) appeared to be an effective and well-tolerated treatment for low grade VaIN. Thirty-six of 42 (86%) patients from a study by Buck et al achieved clearance of vaginal lesions on completion of the initial course of treatment. After the follow-up for at least 6 months, 92% of patients remained clear of VaIN.95
Results from a randomized clinical trial showed that vaginal imiquimod appeared to be as effective as laser treatment for the treatment of VaIN. Histological regression was observed in 80% of the cases in the imiquimod arm, 100% in the laser arm, and 67% in the expectant management arm (p=0.628).96
The most recent systematic review, including 28 patients from five articles and nine cases of VaIN 2/3 treated with imiquimod, reported a pooled complete response rate of 76% and a response rate of 89%, regardless of a history of hysterectomy.97 The authors concluded that imiquimod seemed effective for treatment of VaIN 2/3. The treatment itself is demanding since it must be carried out at least three times a week for 8 weeks and requires a significant commitment by health professionals. However, self-administered vaginal imiquimod, as used in a randomized prospective study by Tainio et al, appeared to be an acceptable mode of treatment, which would certainly lead to a better compliance from patients96
5-Fluorouracil (5-FU) was considered promising in the local therapy of VaIN. In a study by Fiascone et al, 104 patients with VaIN were treated initially with 5-FU, excision, or laser ablation. Patients who received 5-FU had the highest cure rate (74% compared with 57% and 41%, respectively).98 An even higher cure rate (81–86%) was shown in another study involving 30 patients treated with 5-FU.99 On the other hand, there are studies reporting lower cure rates, such as 62.5%.100 Among patients treated with 5-FU for recurrence of VaIN, 62% did not experience a second recurrence.98 Although treatment with 5-FU is effective, its local side-effects including vaginal discharge, burning, pain or ulcers may be highly uncomfortable and reduce compliance. Approximately 16% of patients treated with 5-FU reported a side effect, most commonly irritation and dyspareunia.98
Trichloroacetic acid, a powerful keratolytic agent confirmed to have a therapeutic effect on HPV-induced genital warts,101 was used in the past in an attempt to treat VaIN. Its use was abandoned as other effective types of treatment have emerged.
Rhodes at al evaluated the effectiveness of intravaginal estrogen therapy as a potential primary treatment modality for VaIN. In a study involving 83 patients with VaIN 1–3 treated by different modalities with or without additional local estrogen, the overall regression rate was 85.5%. In the group of 40 patients treated with intravaginal estrogen only, 90% had regression or cure.102 At the same time, 32 patients who underwent treatment with intravaginal estrogen in addition to one or more other treatment modalities experienced regression or cure in 81.3% of cases, while in patients undergoing treatment without intravaginal estrogen, lesions regressed in only 71.4% of cases.102
RadiotherapyExternal beam radiotherapy is not indicated for the treatment of VaIN. Brachytherapy is a good option, though it is usually not proposed as the first-line therapy because of the risks of long-term radiation effects. It also compromises the possibility for secondary surgery in case of recurrence and makes the colposcopic examination extremely difficult. Nevertheless, it may be effective for selected patients with VaIN 2/3 whose disease relapsed after conservative therapies or with conservative surgery not being feasible. Both low-dose rate and high-dose rate intracavitary brachytherapy have been used for treatment of VaIN. There is no standardization of dose prescription in VaIN and patients should be referred to expert centers. The common dose prescription is 60 Gy to 5 mm below the surface of the vaginal
留言 (0)