A clerk for the adolescent medicine program identified twenty people who met the study inclusion criteria and who agreed to have their e-mail contact shared with the research team. The clerk then gave our team a list of these patients and their emails. All twenty were sent an e-mail invitation to participate in the study by our research team. Of these twenty, nine participants responded (8 females and 1 male) to our e-mail: eight accepting and one who declined our invitation to participate. The person who declined to participate left ED care as a youth and never experienced treatment as an adult and therefore deemed herself to be ineligible. Of the eight people who agreed to participate, two participants did not attend their interview and did not respond to subsequent requests to arrange an alternative time. Six participants (5 females and 1 male) completed interviews for the project.
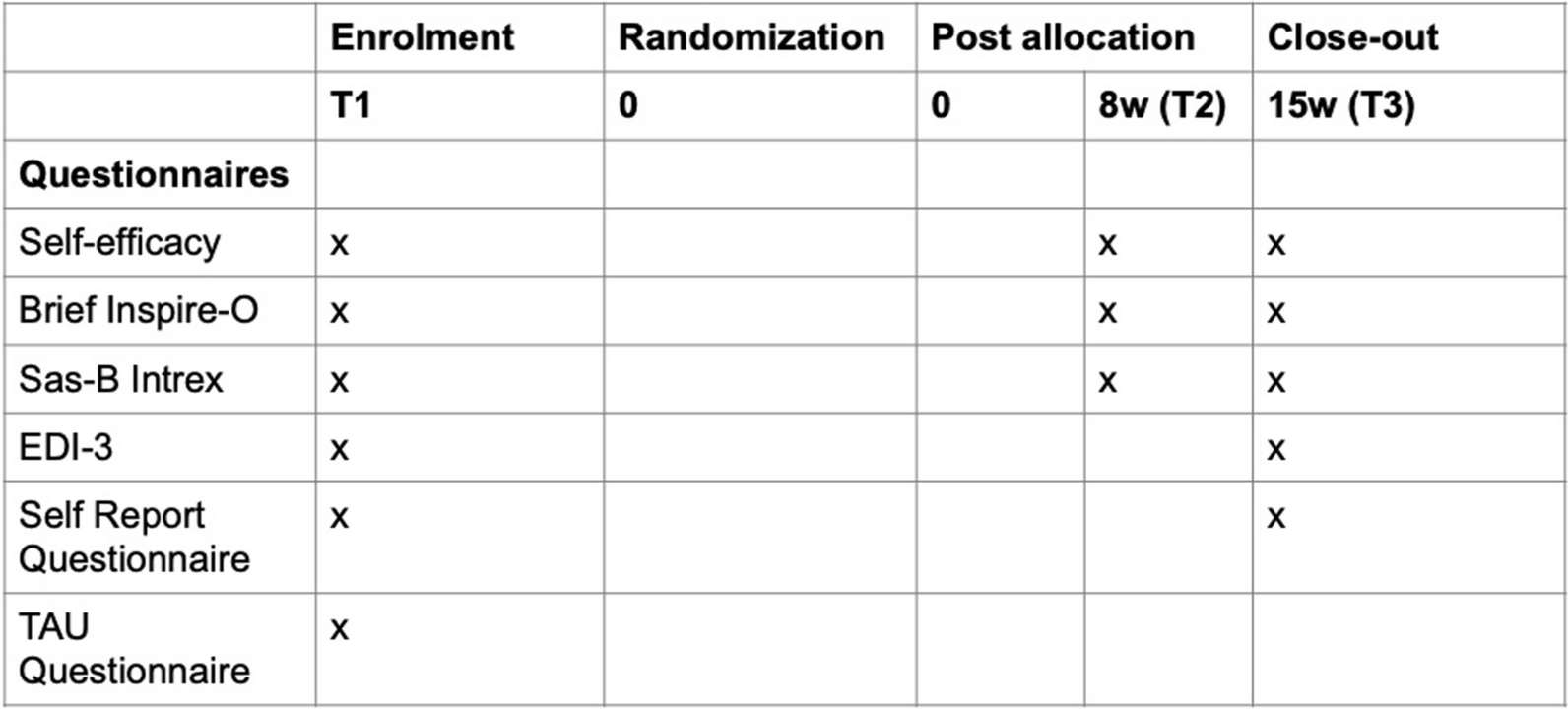
Our analysis identified three main themes with seven subthemes (Table 1). Themes refer both directly to the issues related to transition process and to patients’ health status/needs during this period. The main themes related to the unique challenges faced by ED patients during their transition to adult care, the issues they encountered within adult care, and the value they saw in the development of an educational resource. Although these themes were not discussed in every interview, likely reflecting variation in patient experiences, none of the interviews conflicted with the themes presented below. Supporting quotes are provided from all six transcripts.
Table 1 Summary of ThemesTheme 1: unique challenges for ED patients
All participants found at least parts of their transition to adult medicine difficult. Some of the issues discussed are similar to issues reported by patients with other chronic conditions, e.g., not understanding the transition process or not being familiar with the adult healthcare system. Those who transitioned during the COVID pandemic said that this period caused additional challenges, particularly related to long wait times for adult services. Other challenges that participants identified were unique to the ED population.
Subtheme 1: late age of onset
“I started the pediatrics program when I was 17, I got referred there. About a year after, I got transferred to the adult system.” [Participant 3]
In comparison to other medical conditions seen within pediatrics, the relatively late age of onset for ED means that the patient may not have a long relationship with their care team.
There are potentially both advantages and disadvantages to this situation. For other chronic diseases, the fact that families and patients have built, and now have to break, their long relationship with their child’s healthcare providers has been reported as an added burden during transition [26]. The lack of a long therapeutic relationship may lessen the emotional burden of some ED patients as they leave pediatric care. On the other hand, depending on the patient, because of this relatively short therapeutic relationship, they could be left without feeling a strong connection to either their pediatric or adult care team. This situation could lead to adverse outcomes if the patient needs added support during their transition. Another factor is the intensity of the caring relationship. Some patients reported having extensive periods of in-patient hospital care, which could help them form a close connection with their providers over a short period. Finally, this relatively short period of treatment may result in suboptimal weight restoration, symptom control, and cognitive rehabilitation required to fully comprehend and retain education about eating disorders, long-term impacts, and the recovery process. It is unclear how this relatively short duration of illness before transition impacts a patient’s knowledge of and ability to self-manage their condition, but may lead to increased educational needs during this period.
Subtheme 2: cycle of symptoms
“Comparable to a wave. So sometimes they [the symptoms] were stable and sometimes they were up and down.” [Participant 2]
Recovery is not a linear process. It is common for ED patients to go through cycles during which their symptoms worsen or improve. This fluctuating road to recovery may impact their transition experience, particularly if they are doing well at their time of transition and did not require close follow up. Four of the six participants said that the severity of their symptoms changed in the period after leaving pediatric care, a time when they may not have had specific ED follow up in place yet and were trying to navigate a new healthcare system. The transition experience itself can also negatively impact patients’ symptoms due to the change in independence, as expressed by Participant 5.
“After you’ve been discharged, there’s a point, where I guess, you don’t really receive direct care anymore… and there’s not really anyone watching you as closely, kind of thing. So, I would definitely say the symptoms worsened.” [Participant 5]
Subtheme 3: transition versus discharged
“When I was discharged from the Janeway, I think one of the hardest things after that… so once I went home, I had my appointments that I was supposed to go to and stuff, but I still felt like a bit of disconnect, if that makes sense. I kinda didn’t really know what to do and what I was able to do and I don’t know… just mentally, it was very challenging.” [Participant 5]
The patients interviewed all discussed being hospital inpatients as part of their ED treatment. The discharge from an in-patient hospital-based ED program can be quite dramatic for patients, possibly even more so than their transition into adult care. After leaving hospital, for those under 18, they would return home but continue to be regularly seen on an outpatient basis by the ED team. Because ED patients are seen in Newfoundland through the Adolescent medicine program, there is no clear corresponding program on the adult side, as there is for example between pediatric and adult endocrinology. At the age of 18, depending on the status of the patient, they would have most likely been referred to a community-based eating disorder program or discharged from care. Within the context of the late age of onset and the cycle of symptoms, patients interchanged discussions of being discharged and transitioned. Other participants contrasted transitioning with discharge.
“The process was very abrupt.… I basically had an appointment, and she [the healthcare provider] said… ‘You’re discharged.’ And I was like, oh okay. Sounds good. And that was pretty much the discharge process. I wasn’t transitioned over.” [Participant 6]
Overall, it is important for patients to understand that discharge does not mean recovery. If there are signs of relapse, patients should know where to reach out for care and be encouraged to maintain regular medical follow up with their family physician.
Theme 2: issues in adult care
Unique issues related to EDs also impacted the participants’ experiences of adult care. These issues included their current understanding of adult care and the impacts brought about by the change in treatment care models.
Subtheme 1: new autonomy
“I know from personal experience, there is a difference in how they treat you. In regards to when you’re an adult with an eating disorder, it’s treated as it’s your responsibility and it’s your choice, however, that’s not necessarily the case. Whereas in the Janeway, they get families involved to help with the program, so there are some differences.” [Participant 3]
A significant change between pediatric and adult care is that in the adult system, the patient is expected to take responsibility for managing their own care after transition, whereas in pediatric care, family-based therapy is the mainstay of treatment, which involves the caregivers taking over complete responsibility of their child’s nutrition, ED symptoms, and medical follow up for some amount of time. Without proper education, this new autonomy can be an unexpected change: “it was surprising to me that I had so much choice in the matter of my treatment” [Participant 4]. For a condition like ED for which some patients may choose not to seek treatment due to ambivalence about recovery or denial about their illness, this new autonomy can be a significant issue. As Participant 1 said, “I felt really confident during my treatment when I was an adolescent, however… I found it was a lot more self assessment as I got older, which was harder for me.”
In the above quote from participant 3, there is also the sense that adult providers inadvertently imply that the ED and recovery process is the patient’s choice. This perspective and way of communicating would be significantly different from that taken by pediatric providers, particularly within the context of an ED program. If adult providers did imply the person’s ED as their choice, this view could put added pressure on the therapeutic relationship. It also points to the need for some education directed towards adult providers who may support patients with ED but who may not have a deep understanding of the ED population and how to communicate with them appropriately.
Subtheme 2: co-morbidities
“I think regardless if you’ve had an eating disorder, if you’ve been admitted to the hospital or whatever they do, because this is obviously a mental health disorder” [Participant 2].
Some participants classified ED as a mental health disorder. Other participants said that mental health conditions are common comorbidities for patients with an ED. Participants expressed the view that the adult resources available to them through community programs only focused on the patient’s ED symptoms, while not addressing any co-morbidities. As Participant 3 said: “the primary focus in an ED program is an ED, but they shouldn’t just deny or sum it all to one illness, when there are other illnesses at stake.” Even if it did not impact the patient’s ED symptoms, participants said that transition and the period of being a young adult can still be difficult on patients’ mental health.
“I believe that my [ED] symptoms remained pretty stable during the transition…. I think the more generalized mental health got worse. You know, things that come with EDs, other symptoms like depression and anxiety, things like that, got a little bit worse.” [Participant 4]
Theme 3: the value and content of educational resource
All the participants said that it would be “definitely” or “absolutely” helpful to have an educational resource to better support transition. Some were surprised that such a resource does not already exist. Participants also discussed the potential of an educational resource beyond it being just a static source of information directed towards young adult patients.
Subtheme 1: resource as a connection tool
“I found it a little bit difficult because I kinda felt like I didn’t know where all my information was and it was harder to get all that information from the Janeway and bring it to the Adult care… it would give the Adult team a little bit more understanding of what you had previously gone through and what treatment you had received. Because it would help them understand… what has worked for you and what has not worked for you.” [Participant 4]
When the research team initially considered the educational resource, we saw it as a static way to present information to young adults with ED as a means of better informing them about their condition and their move to adult care. A common theme was that participants saw the value of this type of education resource as a way of better engaging with providers on the adult side. Participants envisioned the resource having a summary of their previous interactions with the pediatric system, e.g., drugs prescribed, providers seen. While they still wanted standard information about ED included, patients also wanted this resource to be a kind of personal health passport which they could share with their new providers. “It would be helpful for the new professionals to understand you better” [Participant 3]. Some of this information would be in the patient’s electronic health record, but it is not clear which providers could access the patient’s records, particularly if post-transition treatment is received through a community-based program. Having this information in a resource that the patient has would also allow them to be more engaged in discussions about their past care and future directions.
Subtheme 2: resource as a benchmark
“I had a bunch of tests done when I first got admitted to the Janeway and I honestly would like to see where my body is now compared to where it was then. Yes, I think it would be very helpful.” [Participant 2]
Participants saw value in having a history of their medical record, including professionals they saw, diagnostic imaging reports and bloodwork results, as a way of benchmarking where they are with their condition. As mentioned above, one of the features of having an ED is that the symptoms often go in cycles. Some patients also make significant progress in treating their condition. Being able to clearly see the improvements in their physical state may help both with the appreciation of the progress and as a motivator for maintaining their positive health gains. For patients who see signs of deterioration in some health measures, providers could discuss ways that patients can return to their previous state of health. Of note, some patients’ distorted ED thoughts applaud them for being ‘sicker’ therefore, this should be a consideration when sharing results with the patient.
Contents of the educational resource
We asked participants about the type of content that they thought should be included in any educational resource. Specifically, we ask whether patients thought it would be useful to include either a summary of their previous treatments, information regarding the transition process, a list of main healthcare providers they saw for their ED, a list of previous and current medications, results of tests completed before transition, a description of the differences and expectations of the adult system, a list of follow up appointments and a list of community and emergency mental health resources. Overall, participants felt that all this information would be useful to include in an educational resource. The benefit that patients saw about including this information mostly related to the benefits for engaging with new providers and benchmarking their physical state versus their performance on previous tests.









留言 (0)