
記住我










The practice of self-medication has received considerable attention as a major public health challenge in low-income and middle-income countries (LMICs).1 2 The median prevalence of self-medication is estimated to be 55.7% in Africa and 70.1% in West Africa.3 Also, the WHO estimates that 20%–50% of all antibiotics in LMICs are inappropriately used.4 The high prevalence of self-medication in LMICs is mainly due to the limited access to healthcare, high cost of healthcare, poor conditions of health facilities and inappropriate health-seeking behaviours in the general population.5 6
Although self-medication is known to reduce the pressure on healthcare systems,7 it is associated with severe challenges, particularly in countries where health literacy is low.8 Key among these challenges include the development of antimicrobial resistance, increased morbidity, rising costs of healthcare services,9 foetal malformations, maternal deaths, psychopathological symptoms among pregnant women,10 11 drug addiction, toxicity and drug–drug contraindications.12
In Ghana, the practice of self-medication is associated with massive health system costs. Antimicrobial resistance attributable to self-medication in Ghana is high.13 14 Annually, an estimated cost of US$20 million is incurred in the Ghanaian healthcare system as a result of inappropriate antibiotic use for upper respiratory tract infections alone.15 Also, recent studies have reported a high prevalence of self-medication among pregnant women in Ghana,16 17 and this could lead to fetal malformation and maternal deaths18; derailing Ghana’s efforts towards promoting safe motherhood and improving maternal and neonatal health outcomes.19
Despite the above concerns, evidence on the practice of self-medication in Ghana is disjointed. Although several primary studies have reported different proportions and reasons for self-medication in Ghana, there has been no systematic review providing a comprehensive report on the prevalence and reasons for self-medication in Ghana. The only available review on self-medication focused solely on pregnant women.20 This paper, therefore, sought to determine the prevalence of self-medication and to identify the reasons for its practice in Ghana. This work significantly contributes to the existing knowledge on the practice of self-medication in Ghana and informs policies in the fight against this public health menace.
MethodsSearch strategyPubMed, Science Direct and African Journals Online were searched for observational studies published from the dates of inception to March 2022. The search strategy for this review included a combination of MeSH terms and free text words. Google Scholar and the websites of the Ministry of Health (https://www.moh.gov.gh) and the Ghana Health Service (https://www.ghanahealthservic.org) were searched for grey literature. The full search strategy and the terms used have been included in online supplemental Table S1). Additionally, to reduce the possibility of missing studies, the reference lists of relevant studies were manually inspected for additional records. The literature search began on 10 October 2021 and ended on 5 April 2022. This review is not associated with a registered protocol and the study reporting followed the 2020 statement of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).21
Eligibility criteria and study selectionThe population-intervention-comparison-outcome-context framework was used to select studies for inclusion (see table 1). Studies qualified for inclusion if they were observational studies and presented primary results on the prevalence and/or reasons for self-medication in Ghana. Studies were excluded if they reported intervention(s) on the use of prescribed medicines, multiple publications of the same study (in which case only the first publication is retained), or studies that did not present primary results on either prevalence or reasons for self-medication in Ghana. Also, opinion papers and commentaries were not included in this review. We did not limit the review to any specific subpopulation or time since the goal was to provide a comprehensive account of the prevalence and reasons for self-medication in Ghana.
Table 1Framework for determining the eligibility of studies
Guided by the eligibility criteria, two authors screened the titles and eligible titles were exported into a Microsoft Excel file. Two authors independently applied the eligibility criteria to select studies for inclusion. The remaining authors were consulted in the event of disagreements in the selection of studies. Also, three authors independently confirmed the justifications for the exclusion of studies after the full-text screening. The list of the excluded studies can be found in online supplemental table S2.
Quality assessment and data extractionThe Mixed Methods Appraisal Tool22 22 was used to assess the methodological quality of studies. The tool is used to assess the quality of primary studies based on seven (7) questions. Reviewers answered ‘yes’, ‘no’ or ‘can’t tell’ to each question and studies that received a ‘yes’ on 6–7 questions were judged as high quality, 4–5 as moderate quality and 1–3 as low quality. Three reviewers independently assessed the quality of the studies and disagreements were resolved through consultation with the other reviewers. Details on the risk of bias assessment can be found in online supplemental table S3 (qualitative studies), online supplemental table S4 (quantitative studies) and online supplemental table S5 (mixed-methods studies).
Data were extracted using an Excel spreadsheet to complete the following information about the selected studies: author and year of publication, study location (region, geopolitical zone and setting), sample size, study design, study year, age of respondents, the prevalence of self-medication and reasons for self-medication. Data extraction was done by three authors independently and was checked by the remaining authors for completeness and accuracy.
Data analysisMeta-analytical techniques were used to estimate the pooled prevalence of self-medication in Ghana using MetaXL23 in Microsoft Excel and OpenMeta (Analyst).24 A random-effects model25 was selected over fixed-effect models since the assumption of functional equivalence among studies was violated.26 The Freeman-Tukey double arcsine transformed proportions were used to stabilise the variance of individual studies.27 The results of the meta-analysis were presented visually using a forest plot. Heterogeneity was examined using the I2 statistic; where I2 is the percentage of the total variability in the pooled estimate explained by heterogeneity.28 Values of I2<50%, 50%–70% and >70% were interpreted as low, moderate and high heterogeneity, respectively.29 A leave-one-out sensitivity analysis was used to evaluate the influence of individual studies on the pooled estimate of the prevalence of self-medication.30 The risk of publication bias was assessed by visually inspecting the funnel plot and Egger’s regression test of funnel plot asymmetry.31 Subgroup analyses were performed using interest populations (pregnant women, patients and tertiary students), geopolitical zones (northern belt, middle belt and coastal belt) and study setting (urban and rural) to explore the potential sources of heterogeneity. All statistical analyses were conducted at a 95% confidence level.
The data on reasons for self-medication were synthesised using inductive thematic analysis32 where reasons identified in the various studies were reclassified under key themes (such as ‘long waiting time at health facility’, ‘previous use of drugs’, ‘perceived unserious nature of diseases’, ‘drugs affordable’, ‘high cost of healthcare’). For instance, ‘long delays at clinics/hospitals’33 and ‘spending long hours at health facility’34 were reclassified under the key theme ‘long waiting time at health facility’. Simple counts (tallying) of distribution3 were used to summarise the evidence available from the studies reporting on reasons for self-medication in Ghana.
Patients and public involvementPatients and members of the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
ResultsSearch resultsWe identified a combined total of 1174 studies through the database and manual search for evidence. After removing duplicates, 749 records were left for screening. After title and abstract screening, a total of 713 articles that were not relevant to the review were removed, leaving 36 articles for full-text screening. A total of 30 articles qualified for inclusion after the full-text screening. Our decision to exclude Bonti35 from the analysis was based on the lack of primary evidence (eg, quotes, text excerpts, field notes) to back the study results. Since this reporting practice is not in line with the standards for reporting qualitative research36 37 and does not allow for confirmation of the interpretations made, we excluded it from this study. The study selection results have been presented in figure 1.
 Figure 1
Figure 1 PRISMA flow chart showing the study selection process and results. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studiesThe characteristics of the studies are shown in table 2 (full details in online supplemental table S6). Twenty (66.7%) of the studies were published peer-reviewed journal articles and 10 (33.3%) were grey literature. Three (10.0%) of the studies were of low quality, 10 (33.3%) were of moderate quality and 17 (56.7%) were of high quality. The studies were conducted in 10 (62.5%) of the 16 regions in Ghana. In terms of geopolitical zones, 19 (63.3%) of the studies were conducted in the coastal belt, 6 (20.0%) were conducted in the middle belt and 5 (16.7%) were conducted in the northern belt of Ghana. The majority of the studies were conducted in an urban setting (22, 73.3%), 6 (20%) were conducted in a rural setting and 2 studies (6.7%) covered both urban and rural populations. Twenty-six (86.7%) of the studies were quantitative, 3 (10.0%) were qualitative and 1 study implemented a mixed-methods design. Except for two qualitative longitudinal studies, the remainder of the studies were cross-sectional. All the 30 included studies had a combined sample size of 9271.
Table 2Characteristics of included studies
Prevalence of self-medication in GhanaA total of 27 out of the 30 studies with a combined sample size of 9117 were included in the meta-analysis since 3 of the included studies were qualitative studies. The pooled prevalence of self-medication was 53.7% (95% CI 46.2% to 61.0%) (figure 2). Heterogeneity among the studies was high (I²=98%, p<0.001). The funnel plot (figure 3) and the results of Egger’s test (Z=0.637; p=0.524) showed that there was no evidence of publication bias. The sensitivity analysis showed that the pooled estimate of self-medication was not significantly impacted by any individual study (figure 4).
 Figure 2
Figure 2 Forest plot of the prevalence of self-medication in Ghana.
 Figure 3
Figure 3 Funnel plot for assessing the risk of publication bias.
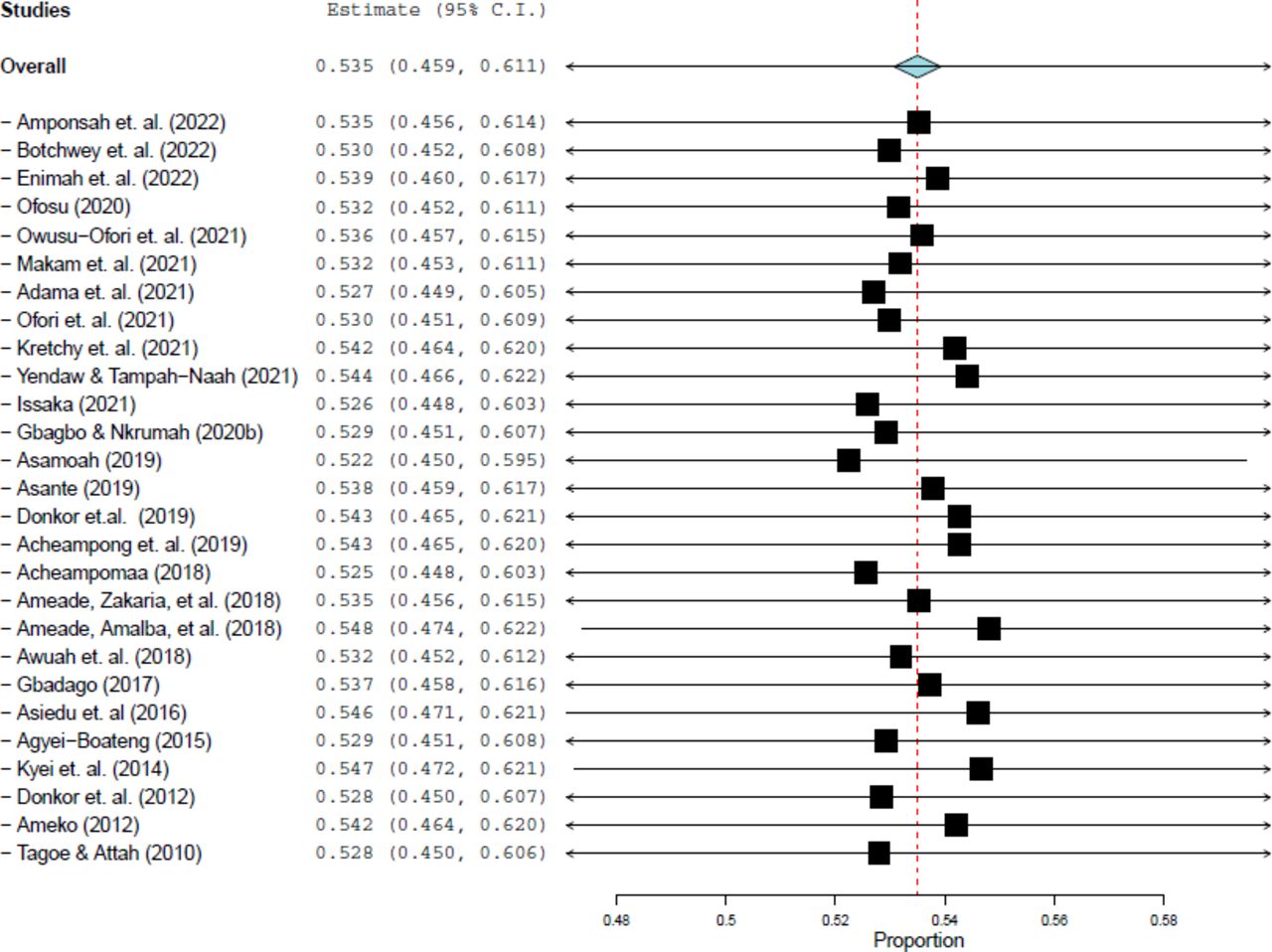 Figure 4
Figure 4 Leave-one-out sensitivity plot.
Subgroup analysisThe prevalence of self-medication by the categorical moderators (interest populations, geopolitical zones and study setting) have been presented in table 3. The prevalence estimates were 65.5% (95% CI 58.1% o 72.5%; I2=88%) among pregnant women, 46.5% (95% CI 26.7% to 66.9%; I2=98%) among patients and 44.1% (95% CI 27.5% to 61.3%; I2=99%) among tertiary students. In terms of geopolitical zones, the highest prevalence of self-medication was estimated in the middle belt (62.1%, 95% CI 40.9% to 82.0%; I²=98%; p<0.001), followed by the coastal belt (52.1%; 95% CI 43.5% to 60.6%; I²=98%, p<0.001) and the northern belt (50.6%; 95% CI 26.8% to 74.4%; I²=99%; p<0.001). For study setting, the prevalence estimate was higher in the rural setting (61.2%; 95% CI 36.5% to 84.5%; I²=98%; p<0.001) compared with the urban setting (52.0%; 95% CI 44.0% to 59.9%; I²=98%; p<0.001).
Table 3Results of subgroup analysis
Reasons for self-medication in GhanaFifteen studies reported data on the self-reported reasons for self-medication in Ghana. The reasons have been presented in descending order based on the proportion of studies reporting them (table 4). The results show that the most commonly reported reasons for self-medication in Ghana were long waiting times at health facilities (73.3%), previous use of drugs (66.7%) and the perceived unserious nature of diseases (53.3%). Other reported reasons for self-medication included drugs affordable (33.3%), high cost of healthcare (33.3%) and long-distance to a health facility (33.3%).
Table 4Reasons for self-medication in Ghana
DiscussionIn the public health literature, self-medication is a phenomenon that has been widely discussed.3 38 A careful analysis of the included studies revealed that out of the 30 included studies, the majority of them (56.7%) were of high quality. This situation is promising as high-quality research serves as a benchmark for societal development.39 The studies included in this review were conducted in ten out of the sixteen regions of Ghana and self-medication in the rural areas remains underinvestigated, as evidenced by the paucity of literature in rural communities. The paucity of literature on self-medication from some regions and the rural setting in Ghana could be due to existing sociocultural and economic constraints that make the conduct of research in these areas challenging.40 41
The results of this review indicate that self-medication is indeed an unresolved menace in Ghana which requires urgent attention. Approximately, 54% of Ghanaians have engaged in self-medication at one point in time. This prevalence estimate in Ghana is similar to prevalence estimates from other LMICs. For instance, prevalence of self-medication was estimated to be 53.57% in India,42 53.3% in Pakistan, 51.5% in Sudan and 49.5% in Saudi Arabia.43 This combination of findings demonstrates that the practice of self-medication is a common phenomenon in LMICs. In LMICs, regulation of the pharmaceutical market is lax, there is poor access and suboptimal utilisation of healthcare and health literacy is low.3 44 These factors could explain the high prevalence of self-medication in LMICs.
The results of the study showed that close to 66% of pregnant women self-medicate in Ghana. This proportion is more than twice the prevalence estimated by a recent global review (ie, 32%).5 Also, lower rates have been reported among pregnant women in Iran (38.46%),45 in Mexico (21.9%)46 and in Ethiopia (26.6%).47 The high prevalence of self-medication among pregnant women in Ghana is all the more a matter of public health concern because self-medication is associated with maternal death, premature birth, low birth weight and fetal malformations.10 11 The findings of the current review support earlier findings that the free maternal healthcare policy in Ghana is not effectively enforced, limiting access to maternal healthcare.48 49
Another population of interest in this review was patients receiving care in health facilities. The current study estimated the proportion of self-medication among patients to be 46.5%. This is consistent with the findings of a recent review that found self-medication among patients in sub-Saharan Africa to be within the range of 45%–89%.38 Like in most LMICs, Ghanaians are likely to try home remedies as the initial health-seeking behaviour and are likely to self-medicate while taking prescribed medicines.50 51 Alarmingly, this practice could lead to drug toxicity, drug–drug contraindications and reduced efficacy of prescribed medicines.12 52
Self-medication was relatively lower among tertiary students (44.1%). This is likely the case because of increased health literacy among this section of the population. Evidence suggests that people with higher levels of education are less likely to self-medicate compared with those with low levels of education.8 12 53 However, the proportion of self-medication among tertiary students is still not desirable given the risk of drug addiction among this cohort of the population.54 Therefore, regardless of the high level of education among this subpopulation, health education may be needed to promote the appropriate use of medicines among students.
The few studies conducted in rural communities revealed that the prevalence of self-medication in the rural setting (61.2%) was higher than in the urban setting (52.0%). In Ghana and most LMICs, rural communities are often characterised by a lack of healthcare facilities, low socioeconomic status, poor transportation systems and suboptimal access and utilisation of healthcare.41 44 55 These factors could explain the high prevalence of self-medication in rural Ghana.
This study estimated the highest prevalence of self-medication in the middle belt of the country (62.1%), followed by the coastal belt (52.1%) and the northern belt (50.6%). The proportions of studies conducted in the urban setting could explain why self-medication was found to be lower in the northern and coastal belts compared with the middle belt. All 5 (100%), 14 (82.4%) and 3e (60%) of the studies included in the meta-analysis from the northern, coastal and middle belts, respectively, were conducted in urban areas. Since self-medication is lower in urban areas, it is not surprising to have a lower prevalence of self-medication in the northern and coastal belts of the country where the proportions of urban-based studies were higher.
Another focus of this study was to identify the reasons for self-medication in Ghana. The results of the current study have revealed that the most common reason for self-medication was the long waiting time in health facilities. In Ghana, most healthcare facilities are still grappling with long patient waiting times as a result of high patient-to-healthcare staff ratios, limited material resources, and poor environmental and design issues.56–58 Patient waiting time is negatively associated with patient satisfaction57 59; and since customer satisfaction is positively related to customer loyalty,60 people are likely to self-medicate or seek alternative care when they are not satisfied with the formal healthcare system.
Previous use of drugs was another common reason for self-medication in Ghana. This finding is not surprising because anecdotal evidence suggests that some Ghanaians tend to restock previously received prescriptions in an attempt to continue the dosage even without their prescriber’s consent.35 In an environment where there is easy access to over-the-counter drugs, people are likely to rely on their past successful experiences with a drug with the hope that they will have the same outcomes as previously.3 Self-medication with previously used drugs is usually without the professional guidance of a healthcare worker,38 making it a very risky practice, especially among vulnerable groups such as pregnant women and patients who are receiving care.
Also, the perception that some disease conditions are not severe to warrant a hospital visit was a commonly reported reason for self-medication from the results of this review. In Ghana, people are likely to underestimate disease conditions since most Ghanaians have limited knowledge of diseases and their symptoms,29 61 62 As such the self-ascribed severity of disease conditions may be tricky since people are likely to disregard important clinical symptoms and delay seeking appropriate and timely medical care. This could lead to poor treatment outcomes and prognosis.63
Additionally, affordability of drugs, high cost of healthcare and long-distance to health facilities were found in this review as common reasons why Ghanaians self-medicate. These concerns have been reported by other studies as contributing to the high prevalence of self-medication in LMICs.3 6 Healthcare systems in many LMICs like Ghana have several challenges including limited access to care, poor quality of care and lack of affordability due to high levels of poverty and poor social support systems.41 44 64–66 These challenges influence the health-seeking behaviours of people, turning them away from the formal healthcare system.67
This review has strengths that are worth mentioning. First, the risk of bias assessment showed that the majority of the included studies were of high quality and there was no evidence of publication bias in this review. In addition, the adherence to the 2020 PRISMA checklist in the reporting of the study gave credence to the study methodology. However, we note the following limitations: (1) the use of interviewer-administered questionnaires by primary studies for data collection might have introduced recall and social desirability bias into the primary evidence used in this review; (2) this review could not make a distinction between responsible self-medication and irresponsible self-medication due to the lack of such distinction in the included primary studies and (3) there was still unexplained heterogeneity after the subgroup analysis due to the limited number of variables we were able to explore from the limited data reported in the primary studies.
Implications for practice, policy and future researchThis review has estimated a high prevalence of self-medication in Ghana, highlighting the need for a renewed focus on the promotion of the rational use of medicines in Ghana. Section 6.3.5 of the Ghana National Drug Policy68 provides four strategies for ensuring patient compliance to prescribed medicines and preventing self-medication in the country. Three of these strategies mainly focus on patient and public education and the remainder on the promotion of research on inappropriate drug use.68 However, nearly two decades after the adoption of this policy, research has shown that Ghanaians are still either ignorant about or disregard the adverse effects of self-medication.69 70 There is, therefore, the need to have a relook at the four strategies; to ensure their effective implementation or review them to match the available evidence on the reasons for self-medication as revealed in this study. The Ministry of Health should resource and encourage health professionals to intensify public education on the perceptions that drive self-medication. Healthcare facilities must adopt innovative strategies to reduce patient waiting times and enhance access to quality healthcare.
Since this study is limited to some extent by inadequate data and/ or information covering the entire country, comprehensive studies across the country could be warranted especially in the regions where little or no information exists including the rural setting. Also, future research needs to implement strong qualitative methodologies to produce findings that provide an in-depth account of the existing practices. Additionally, longitudinal study approaches are needed to investigate how self-medication changes over time as well as assess the effectiveness of interventions that are implemented. All these aforementioned studies will provide representative data and a rounded in-depth understanding of self-medication in Ghana for informed practice and policy direction including any necessary reviews.
留言 (0)