Study Design and Participants
A parallel-group randomized controlled clinical trial involving two groups: SGB and control, was conducted at the First Affiliated Hospital of Fujian Medical University in China, from 26 May 2021 to 23 March 2022. This study was approved by the ethics committee of The First Affiliated Hospital of Fujian Medical University (21 May 2021, FMU|2021|200), and was registered in the Chinese Clinical Trial Registry (ChiCTR2100046620) on 23 May 2021. The study protocol was performed in accordance with the Declaration of Helsinki. A total of 58 female patients aged 18–65 years with ASA I–II who were scheduled for modified radical mastectomy for breast cancer were included in this study. The exclusion criteria included rejection of participation, allergic to anesthetics, history of insomnia, abnormal coagulation disorders, and anatomical deformities of the neck or shoulders. Written informed consent was obtained from all enrolled participants.
Participants were randomized to receive preoperative single-injection SGB under ultrasound guidance (SGB group) or just an ultrasound scan (control group). A list of randomization sequences was generated in a 1:1 ratio by the statistical consultant using the random number table method and then sealed in opaque, sequentially numbered envelopes. All participants, anesthesiologists, outcome collectors, and data analysts were blinded to the group assignment throughout the whole observation period, including all postoperative follow-ups.
Stellate Ganglion Block Procedure
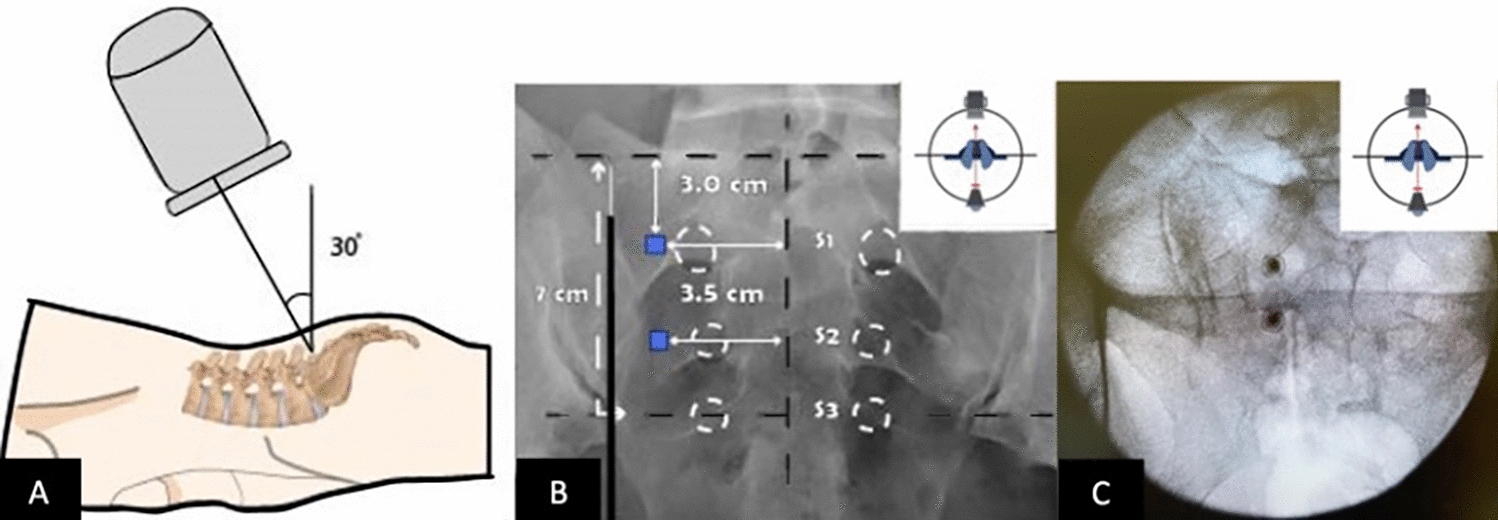
A skilled anesthesiologist who was blinded to group allocation performed all SGBs under sterile conditions using real-time ultrasound (Model Edge; Fujifilm SonoSite, Bothell, Washington, USA). The single-injection SGB began 15 min after the induction of anesthesia in the operating room. In the SGB procedure, patients were placed in the supine position with their necks slightly rotated to the left side. A linear transducer (6–13 MHz) was placed on the neck to achieve a clear visualization of the carotid artery, internal jugular vein, vertebral artery, vagus, thyroid gland, esophagus, longus colli, and anterior scalene at the C6 level. A 48-mm, 20-gauge needle (BD Medical, Sandy, UT, USA) was then inserted into the prevertebral fascia of the longus colli muscle in an “in-plane” direction [22]. Once the needle tip penetrated the prevertebral fascia with a negative aspiration, 3 mL of 0.5% ropivacaine was administered, followed by the spread of the local anesthetic being visualized under ultrasound.
General Anesthesia
After entering the operating room, all patients were monitored with electrocardiogram, invasive blood pressure, peripheral pulse oximetry, and bispectral index (BIS). General anesthesia was administered with midazolam 2 mg, propofol 1.5–2 mg kg−1, sufentanil 0.4–0.6 μg kg−1, and cisatracurium 0.2–0.4 mg kg−1. Flurbiprofen 1.5–2.5 mg kg−1 and tropisetron 5 mg were administered 30 min before the end of the surgery. The BIS values were maintained in the range of 40–60. Using pressure-controlled mechanical ventilation, an end-tidal carbon dioxide partial pressure of 35–45 mmHg was maintained. After the removal of the laryngeal mask/tracheal tube, the patients were transferred to the postanesthesia care unit (PACU) for further monitoring, where the first follow-up visit was carried out to assess Horner’s syndrome and adverse events. A successful sympathetic block can be diagnosed by the presence of Horner’s syndrome on the blockage side (i.e., fascial flush, enophthalmos, ptosis, miosis, and conjunctival congestion) [17]. During the first postoperative 48 h, patients received patient-controlled analgesia (PCA) pump, which consisted of flurbiprofen 4 mg kg−1, tropisetron 0.3 mg kg−1, and sufentanil 2 μg kg−1.
Outcomes
The primary outcome was postoperative sleep quality. The Pittsburgh Sleep Quality Index was used to assess patients’ baseline subjective sleep quality 1 day before the surgery. The SMHSQ and actigraphy (ActiGraph, Pensacola, FL, USA) were used to record subjective and objective sleep quality for 3 consecutive days (1 day preoperative, surgery day, and 1 day postoperative), respectively. The actigraphy was worn on the contralateral wrists of the patients to assess sleep efficiency (SE), sleep onset latency (SOL), total sleep time (TST), number of awakenings (NA), and wake after sleep onset (WASO) through a computer program. The SMHSQ scores from 6 to 38 were used to indicate how well the patient slept.
The secondary outcome was postoperative pain intensity. Cumulative analgesic consumption and numbers of PCA administration were documented. Rest pain intensity was evaluated at 6, 24, and 48 h after surgery using the visual analog scale (VAS).
A 5-mL sample of blood was drawn before surgery and 24 h after surgery to determine the serum concentrations of melatonin, cortisol, serotonin, tumor necrosis factor-α, and interleukin-6. Intraoperative vital signs, Horner’s syndrome, adverse events (i.e., postoperative delirium, cognitive dysfunction, nausea and vomiting, arrhythmia, nerve block complications), the incidence of breast cancer-related lymphedema (BCRL), and postoperative hospital stays were documented.
Statistical Analysis
The sample size calculation for this trial was based on the SE recorded by actigraphy on surgery day. The SE (mean ± standard deviation) of the control group and the SGB group in our pilot study (n = 5) was 80.60 ± 21.06 (%) and 93.88 ± 5.69 (%), respectively. On the basis of our power analysis (α = 0.05 and β = 0.1), a sample size of 23 participants per group was required. To allow for a 10% dropout rate, a sample size of 50 cases was determined.
All statistical analyses were performed using SPSS 26.0 software (IBM Corp., Armonk, New York, USA). The normality of the distribution of quantitative variables was assessed via the Shapiro–Wilk test and Q–Q plots. Normally distributed variables are represented as mean ± standard deviation and analyzed by using the independent-samples t-test. Non-normally distributed variables are represented as median [IQR] and analyzed using the Mann–Whitney U test. Categorical variables are summarized as number (%) and analyzed using the chi-square or Fisher’s exact test, as appropriate. Actigraphy performances, VAS scores, and serological parameters were evaluated using a two-way (between-group comparisons with time and group as two factors to be analyzed) repeated-measures ANOVA or generalized linear mixed model analysis. Correlation analysis was performed using Pearson’s or Spearman’s correlation. In addition, relative risk (RR) with 95% confidence intervals (CIs) was used to compare the incidence of BCRL between groups. P < 0.05 (two-tailed) was considered statistically significant.










留言 (0)