
記住我

Screening and exit DBPCFC data from participants aged 4 to 17 years in the PALISADE (ARC003), ARC004 (PALISADE follow-on), and ARTEMIS (ARC010) trials who received PTAH or placebo were examined post hoc (Fig. 1). Challenge or maximum single peanut protein doses were prespecified for each trial. During the DBPCFCs, peanut protein doses were tested sequentially up to the challenge or maximum single peanut protein dose prespecified for the screening or exit DBPCFC in each trial. To be eligible for trial participation, individuals were required to experience dose-limiting symptoms at or before the prespecified challenge dose of peanut protein in the screening DBPCFC for PALISADE and ARTEMIS. Only participants from PALISADE were eligible for ARC004.
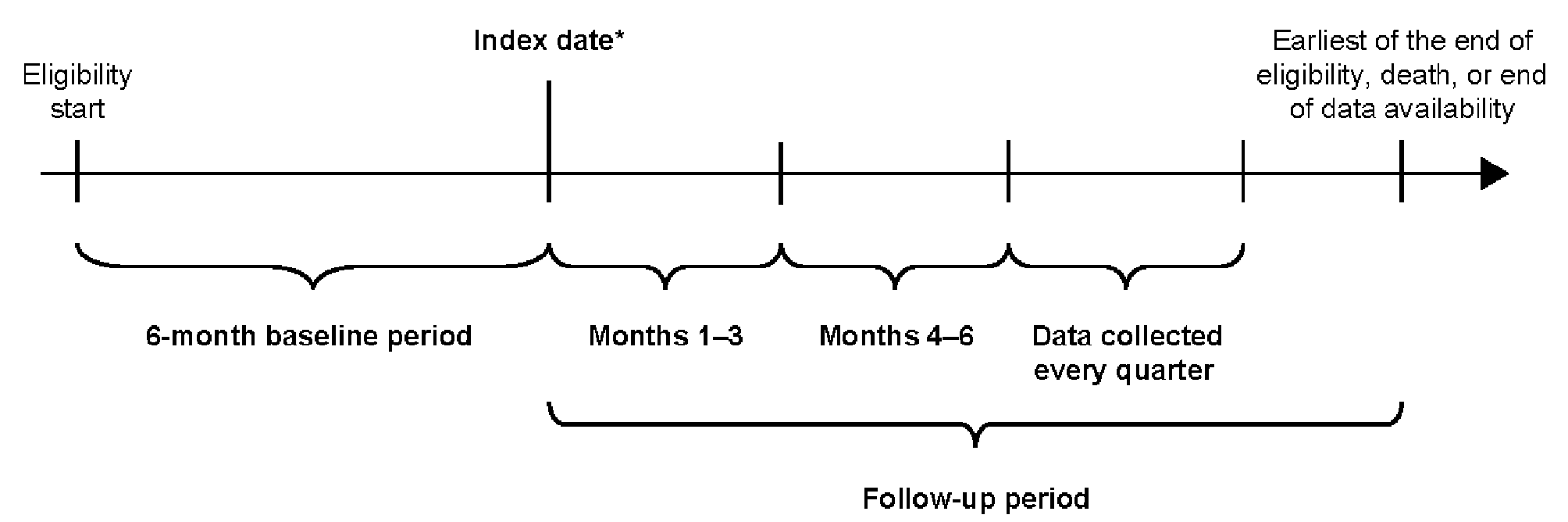
Fig. 1
Trial Design for PALISADE, ARC004, and ARTEMIS. Symptom data were recorded from the DBPCFCs across three PTAH trials of participants aged 4 to 17 years who received PTAH or placebo. Endpoints that were examined post hoc focused on evaluating freedom from symptoms and the reduction of symptom severity over time. aThe maximum single peanut protein dose tested for the primary clinical efficacy endpoint in PALISADE was 1000 mg in Europe (cumulative amount: 2043 mg) and 600 mg in North America (cumulative amount: 1043 mg). bFollowing PALISADE, participants treated with PTAH entering ARC004 could be allocated into one of five extended maintenance cohorts. Cohorts 1 and 3A were daily dosing cohorts and are evaluated in this analysis; the nondaily dosing cohorts (2, 3B, 3C) were not included. DBPCFC double-blind, placebo-controlled food challenge, PTAH peanut (Arachis hypogaea) allergen powder-dnfp
PALISADE was a 12-month, double-blind, randomized, placebo-controlled trial evaluating efficacy and safety of PTAH in individuals with peanut allergy in North America and Europe [21]. A maximum single challenge dose of 100 mg of peanut protein (cumulative dose of 144 mg) was tested in the screening DBPCFC, and the maximum single peanut protein dose tested during the exit DBPCFC was 1000 mg in Europe (cumulative dose of 2043 mg) and 600 mg in North America (cumulative dose of 1043 mg). Participants in PALISADE received ~ 6 months of dose escalation and ~ 6 months of maintenance therapy with PTAH 300 mg or placebo equivalent once daily. To give practical understanding of PTAH therapy in the context of potential real-world exposure, one peanut kernel (of which two are in a usual peanut pod) equates to about 250–300 mg of peanut protein; thus, PTAH 300 mg is equal to approximately one peanut kernel [26].
ARC004 was a 24-month (total duration, including the parent trial duration), open-label, follow-on trial of PALISADE to explore alternate dosing interval regimens and extended maintenance with PTAH [20]. Among the five extended maintenance cohorts enrolled in ARC004 of participants who had received PTAH in PALISADE and continued PTAH therapy in ARC004, only the cohorts receiving daily PTAH (Cohort 1 and Cohort 3A) were included in this post hoc analysis. Participants in Cohort 1 received PTAH 300 mg once daily for ~ 7 months (ie, ~ 13 months overall maintenance treatment), and participants in Cohort 3A received PTAH 300 mg once daily for ~ 14 months (ie, ~ 20 months overall maintenance treatment). A maximum single challenge dose of 2000 mg (cumulative dose of 4043 mg) of peanut protein was tested during the exit DBPCFC in ARC004.
ARTEMIS was a 9-month, double-blind, randomized, placebo-controlled trial evaluating efficacy and safety of PTAH in children and adolescents with peanut allergy in Europe [22]. A maximum single challenge dose of 300 mg peanut protein (cumulative dose of 444 mg) was tested in the screening DBPCFC, and the maximum single dose of peanut protein tested at the exit DBPCFC in ARTEMIS was 1000 mg (cumulative dose of 2043 mg). Participants in ARTEMIS received ~ 6 months of dose escalation followed by ~ 3 months maintenance therapy of PTAH 300 mg or placebo equivalent once daily.
Eligibility criteria varied across the three trials. In PALISADE, eligible participants were between the ages of 4 and 55 years, had clinical history of allergy to peanut or peanut-containing foods, dose-limiting symptoms at or before the 100-mg challenge dose of peanut protein at the screening DBPCFC, and had serum immunoglobulin E (IgE) to peanut of ≥ 0.35 kUA/L and/or a peanut skin prick test (SPT) wheal diameter ≥ 3 mm compared with control. Eligible participants who completed PALISADE and gave written informed consent were enrolled in the ARC004 trial. In the ARTEMIS trial, eligible participants were between the ages of 4 and 17 years, had clinical history of allergy to peanut or peanut-containing foods, had dose-limiting symptoms at or before the 300-mg challenge dose of peanut protein at the screening DBPCFC, serum IgE to peanut of ≥ 0.35 kUA/L and/or a peanut SPT wheal diameter ≥ 3 mm compared with control. Additional study design details for PALISADE, ARC004, and ARTEMIS have been previously reported [20,21,22].
In this analysis, the DBPCFC was used to demonstrate accidental peanut exposure in the real world (ie, simulation of exposure to peanut), and results from the screening and exit DBPCFC were used to provide insight into the amount of peanut protein a participant could safely consume before and after treatment. Endpoints were change in symptom severity and freedom from any symptoms during DBPCFC. The maximum tolerated dose (ie, single highest tolerated dose) was the highest peanut protein dose given during a titrated DBPCFC that elicited no symptoms or symptoms that were not considered dose-limiting (ie, clearly indicative of an allergic reaction; Fig. 2). The reactive dose was the peanut protein dose at which a participant showed dose-limiting symptoms and was one dose level after the maximum tolerated dose.
Fig. 2
Example to Illustrate the Reactive Dose. Step-up challenge dosing schedule for screening and exit DBPCFC for the PALISADE trial. Participants who were in the ARTEMIS (ARC010) trial had a maximum screening DBPCFC dose of 300 mg. Participants who tolerated doses of peanut protein had subsequently higher doses until a reactive dose was reached. The prior dose to the reactive dose was defined as the single highest tolerated dose, or maximum tolerated dose. DBPCFC double-blind, placebo-controlled food challenge
Change of symptom severity to peanut was assessed using maximum severity at any dose of peanut protein in the exit DBPCFC by system organ class (SOC) in the PALISADE trial and maximum severity of symptoms at the reactive dose of peanut protein in the screening DBPCFC compared with the same dose in the exit DBPCFC in the PALISADE trial. Severity of symptoms presenting during the DBPCFC were assessed using the PRACTALL (ie, dose-limiting symptoms) and the Consortium of Food Allergy Research (CoFAR) grading systems (ie, severity) for allergic reactions during the trial [20,21,22, 27]. The CoFAR grading system for allergic reactions defines five grades in ascending order of severity: mild (grade 1), moderate (grade 2), severe (grade 3), life-threatening (grade 4), and death (grade 5), each with specific definitions based on timing, limitations in activity, and presenting symptoms [27]. Severity of symptoms was also determined based on investigator’s judgment. Maximum symptom severity was assessed and reported as no symptoms, mild, moderate, or severe, and grouped by the following SOCs: respiratory, gastrointestinal (GI), cardiovascular/neurological, and dermatological. Maximum severity of symptoms was also assessed at the reactive dose in the screening DBPCFC and compared with the same dose in the exit DBPCFC for the PALISADE trial to evaluate dose-dependent changes of symptom severity at a patient-individual dose of peanut protein. For participants who reacted to a lower peanut protein dose during the exit DBPCFC than the screening DBPCFC, data from screening DBPCFC were classified as “with replacement” (WR). The maximum severity of symptoms reported during the screening DBPCFC was used as the exit DBPCFC maximum symptom severity because the reactive dose was lower during the exit DBPCFC than at the screening DBPCFC.
Freedom from any symptoms to peanut was assessed at doses ≤ 100 mg of peanut protein in the exit DBPCFC in PALISADE and ARTEMIS and at doses ≤ 1000 mg of peanut protein in the exit DBPCFC in the PALISADE, ARC004, and ARTEMIS trials. Freedom from any symptoms indicated participants were asymptomatic to peanut exposure at the tested peanut protein dose.
Statistical analysesDescriptive statistics were reported for each treatment group. Comparisons between treatment groups were conducted using relative risk (RR), which was the primary efficacy measure. The Cochran-Mantel-Haenszel statistic was used to test for treatment difference between screening and exit DBPCFC (if applicable) and difference between treatment groups. Analyses were conducted in the intention-to-treat population, wherein participants who dropped out during the trial were considered “not improved.” For evaluations of maximum symptom severity during DBPCFCs in PALISADE, exit DBPCFC data were analyzed WR, as previously described. Participants reacting to a lower peanut protein dose in the exit DBPCFC compared with the screening DBPCFC only occurred in the placebo group. The WR analysis also reported participants with missing data and dropouts.
留言 (0)