The main finding of this study was that novel biomarkers are a reliable predictor of poor neurological outcomes at 6 months after CA. Cutoffs from two large existing studies (TTM and COMACARE substudy) were applied to this study, resulting in specificity at or close to 100% and sensitivity comparable to the existing studies. This provides clear evidence that these cutoffs are valid for different patient cohorts and laboratories. The AUC for predicting poor neurological outcome was the highest at 72 h after CA for all novel biomarkers. The AUCs for the novel biomarkers were higher than those for conventional biomarkers at 72 h after CA. Among them, the NFL at 72 h after CA had the highest AUC (0.946) and the highest sensitivity (77.1%) with 100% specificity.
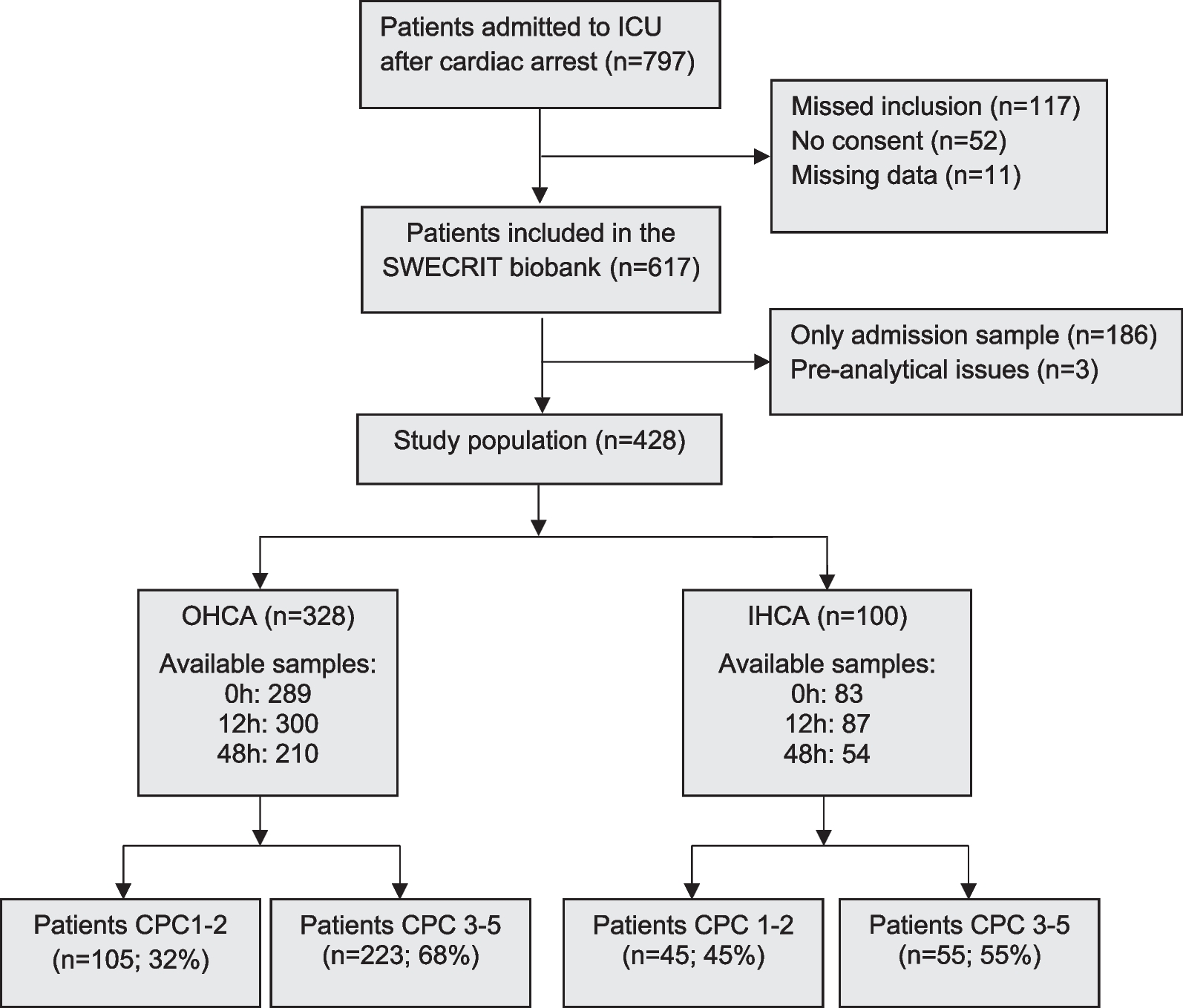
Our study had several strengths compared with previous studies [4, 9,10,11,12, 16]. First, WLST was not performed on patients included in this study, which minimized the self-fulfilling prophecy. Among the 54 patients with poor neurological outcomes included in this study, 3 (5.6%) patients had a CPC score of 3, and 14 (25.9%) patients had a CPC score of 4, which provided clear evidence that WLST did not influence the results of this study. In addition, since the treating physician was blinded to the novel biomarker results, bias was minimized. Second, this study enrolled patients of Asian ancestry with OHCA with a different etiology than that of previous studies. There were 50 patients (50%) with cardiac-induced OHCA and 36 patients (36%) with initial shockable rhythm. The causes of CA in patients with noncardiac causes were asphyxia in 29 cases, other noncardiac causes in 20 cases, and drug intoxication in 1 case. This contributed to the generalizability of novel biomarkers.
Tau is mainly located in the white matter of the central nervous system and functions to stabilize the structure of microtubules [22]. Mattsson et al. used TTM trial data and reported that tau predicted poor neurological outcome more accurately than NSE at 24 to 72 h after CA and that tau's predictive power increased over time (the AUC at 24, 48, and 72 h was 0.81, 0.90, and 0.91, respectively) [9]. The half-life of tau is approximately 10 h, and a late rise in tau concentrations likely reflects ongoing neuronal damage. In this study, the tau concentration increased over time in the poor neurological outcome group, and the AUC for predicting poor neurological outcome was the highest at 72 h after CA (the AUCs at 24, 48, and 72 h were 0.767, 0.837, and 0.906, respectively). This was consistent with Mattsson's study.
Neurofilaments composed of neurofilament light chains, neurofilament medium chains and neurofilament heavy chains form the cytoskeleton of neurons and are expressed exclusively in neurons [23]. Moseby-Knappe et al. used TTM trial data and reported that the diagnostic performance of NFL was stable from 24 to 72 h (AUC, 0.94), and its performance did not increase significantly when combining serum NFL at different time points [12]. Wihersaari et al. used COMACARE trial data and reported that NFL had excellent prognostic accuracy at 24 h (AUC 0.983) and was a more accurate biomarker for prognostication after CA than NSE [20]. However, in this study, the prognostic power of NFL was the highest at 72 h, contrary to previous studies. One possible explanation is due to differences in the patients included in the study. Both the TTM trial and COMACARE trial included only patients with cardiac causes of cardiac arrest and the patient population was different from that in this study in several aspects, such as the rate of witnessed arrest and total anoxic time. Additionally, this study only included 100 patients, which is a small number compared to the number of patients included in the study by Moseby-Knappe et al.
GFAP is a structural component of intermediate filaments in the astrocyte cytoskeleton, and GFAP production is upregulated after ischemia, which is considered a neuroprotective mechanism [24]. The accuracy of GFAP in predicting neurological outcomes after CA appears to be better at 48 and 72 h after CA compared to earlier time points, with AUC values reported between 0.65 and 0.89, respectively [16, 25, 26]. Ebner et al. used TTM trial data, and thresholds with 100% specificity for predicting poor neurological outcome at 24–72 h after CA were reported as 3425, 2952, and 3581 pg/mL, with sensitivities of 17, 19, and 12%, respectively [21]. On the other hand, thresholds with 100% specificity for predicting poor neurological outcome at 24–72 h after CA were 1970, 9520, and 1180 pg/mL with sensitivities of 44, 44, and 55%, respectively, in this study. However, the cutoff of 9520 pg/mL at 48 h has the potential for laboratory error that requires careful interpretation. Excluding this patient, the cutoff at 48 h is 1880 pg/mL. The reason for the higher sensitivity in this study compared to that in previous studies is difficult to explain, suggesting that more research is needed.
UCH-L1 is a very abundant protein in the brain and consists of 223 amino acids. Ebner et al., using TTM trial data, reported that UCH-L1 had good accuracy in predicting poor neurological outcome after CA (AUC between 0.85 and 0.87). UCH-L1 was significantly better at predicting poor neurological outcome after CA than NSE at 24 and 48 h but not at 72 h. This was explained by the shorter half-life of UCH-L1 compared to that of NSE [21]. However, in this study, the prognostic power of UCH-L1 was the highest at 72 h, which differed from a previous study. As mentioned previously, the TTM trial only included patients with cardiac-caused cardiac arrest and the patient population was different from this study in several aspects, such as the rate of witnessed arrest and total anoxic time. In other words, it is possible that the results differed due to differences in disease severity.
The Additional file 1: Table S2 presents the p value of the De-long test comparing the AUC curves of novel biomarkers and conventional biomarkers for predicting poor neurological outcomes after CA. The AUC of GFAP was superior to that of NSE and S100B in predicting poor neurological outcomes after CA at 0 h (p = 0.0307 for NSE and p = 0.0029 for S100B), and the AUC of NFL and UCH-L1 were superior to S100B at 48 h (p = 0.0333 for NFL and p = 0.0135 for UCH-L1). Both NFL and UCH-L1 predicted poor neurological outcomes after CA better than NSE and S100-B at 72 h (p = 0.0168 for NFL vs NSE, p = 0.0148 for NFL vs S100-B, p = 0.0361 for UCH-L1 vs NSE and p = 0.0069 for UCH-L1 vs S100B). These results comparing the novel biomarker with the conventional biomarker require further validation.
Predicting a good outcome is as important clinically as predicting a poor outcome in comatose PCAS patients. In this study, the biomarkers within the normal range at 24 h showed good neurological outcome at 71.7–100%, and the biomarkers within the normal range at 24–72 h showed good neurological outcome at 80–100%., which is consistent with the results of the TTM trial substudy [4]. Especially, patients with NFL or GFAP levels within the normal range do not have hypoxic-ischemic encephalopathy (HIE) with a very high probability. This provides evidence for preventing erroneous WLST and providing more critical resources to patients with good outcomes.
There were 29 patients with an NFL level of 500 pg/mL or higher at 72 h, and 28 of them had a poor outcome. There were 25 patients with an NFL level of 1000 pg/mL or higher, and all of them had poor outcomes. Therefore, patients with an NFL of 1000 pg/mL at 72 h have a very high probability of having HIE.
Our study had several limitations. First, this was an observational study with a small sample size, which raises the concern of type II errors. In addition, the comparison of prognostic ability between biomarkers was not possible due to the small sample size. Second, although there was no WLST in this study, 11 patients died before 72 h. Missing data caused by early deaths may have increased the possibility of bias. Third, the analysis methods for novel biomarkers are not standardized. We used the highly sensitive SIMOA immunoassay, which is not available in most laboratories. In addition, it is impossible to compare our results with previous studies that did not use this method. Forth, due to the nature of observational studies, the results of our analysis and the cutoff values for novel biomarkers require further validation. Finally, we could not prove whether the novel biomarkers could be more useful in clinical practice than the conventional biomarkers. Several modalities are used to predict neurological outcomes in patients with CA, and the current guidelines recommend using a combination of several modalities. Therefore, the clinical usefulness of the novel biomarker must be demonstrated in a combination of several modalities suggested in the current guidelines.


留言 (0)