
記住我


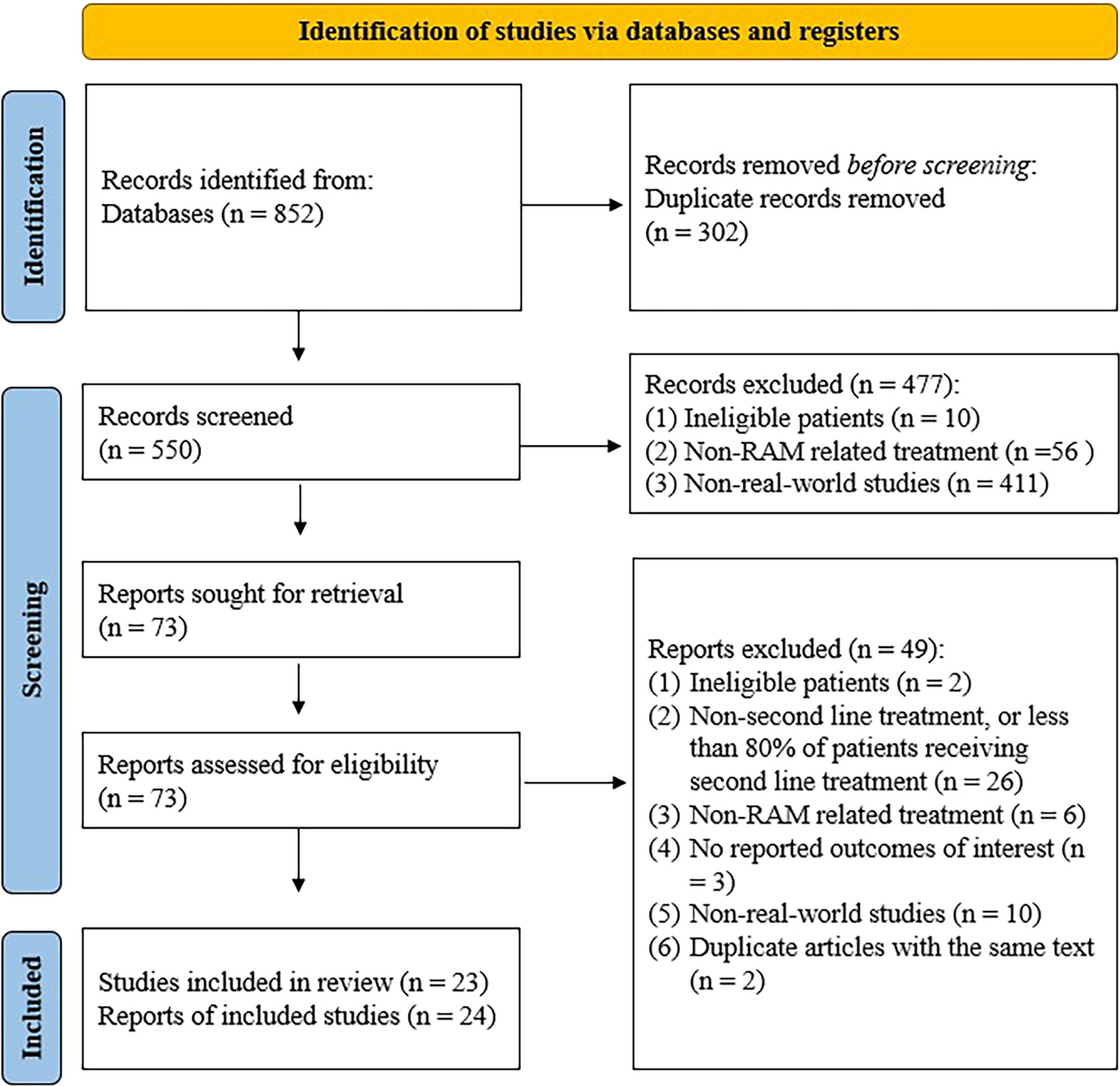
The original and updated database searches identified a total of 1886 publications of connection-enabled insulin platforms and their comparators, while the searches of conference proceedings identified 12 relevant conference abstracts (Fig. 1). Of these, 292 were retained for full-text screening; 267 were excluded, leaving 25 for inclusion. The gray literature search identified one report of interest [27]. Therefore, the final number of publications included was 26, representing 10 unique studies (Fig. 1).
Fig. 1
PRISMA flow diagram of study selection. PRISMA Preferred Reporting Items for Systematic Reviews and Meta-analyses, RCT randomized controlled trial
A search of the European Union’s Clinical Trials Register did not identify any relevant studies; however, the search of ClinicalTrials.gov identified 24 records of completed (n = 12), ongoing (n = 6), or discontinued/unknown (n = 6) trials of interest, all but one of which were discarded (no results, n = 22; duplicate publications, n = 1). One clinicaltrials.gov entry with a data presented as a conference abstract was used for additional information on one of the included RCTs [28, 29]. One Eli Lilly clinical study report was also included to support one of the included observational studies [30, 31].
Study Characteristics and Interventions/ComparatorsStudy design details of the ten unique studies are summarized in Supplementary Material Table S3. Two open-label RCTs were identified, both of which assessed a connected insulin cap (Insulclock®); one was fully published [32] and one was a conference abstract [28, 29]. The six observational studies included were prospective cohort studies that assessed connected caps (Insulclock®, GoCap®), connected insulin pens (NovoPen® 6; Bravo pen®, InPen®), or a connected insulin platform (ESYSTA®). Of these, one subgroup analysis (evaluating NovoPen® 6) was fully published [33], four, with an additional subgroup analysis, were conference abstracts [31, 34,35,36,37], and the one evaluating a connected insulin platform (ESYSTA®) was a white paper [27]. These core publications were associated with several supporting publications [32, 38,39,40,41,42,43,44,45,46,47,48,49,50]. Features of the devices evaluated in these studies are summarized in Table 1.
Table 1 Features of connection-enabled devices included in this reviewOf the two economic studies, one assessed a connected insulin pen (NovoPen® 6) and was fully published [51] with a conference abstract [47] and the other investigated the connected insulin platform (ESYSTA®) and was a conference abstract [52].
The outcomes investigated in all the studies are summarized in Supplementary Material Table S4.
Characteristics of the Participants with DiabetesBaseline characteristics of the populations of people with diabetes are summarized in Supplementary Material Table S5. Of the studies evaluating Insulclock®, two included people with type 1 diabetes mellitus (T1DM) [32, 36] and one included people with type 2 diabetes mellitus (T2DM) [29]. Single studies evaluated GoCap®, Bravo pen®, InPen®, and ESYSTA® in people with T1DM or T2DM [27, 31, 34, 35], and two parts of one study [40] evaluated NovoPen® 6 (one in adults with T1DM and the other in children and adolescents with T1DM) [33, 37].
Across all studies, people with T2DM were generally older than those with T1DM. Baseline demographics and disease characteristics were infrequently reported in these studies. In studies conducted in adults, 39–56% of people were female and mean age was 39–60 years. Current use of CGM was reported in six studies (Supplementary Material Table S5) [31,32,33,34,35, 37].
Clinical and PROsConnected CapsIn RCTs, clinical outcomes indicate that the introduction of connected insulin caps resulted in improved glycemic outcomes (Table 2; details are provided in Supplementary Material Table S6) [29, 32]. In 16 people with T1DM, Insulclock® was associated with significant improvement from baseline in CGM metrics in the overall (active use plus masked use) population, including time in range (TIR), time above range (TAR), and glycemic variability (p < 0.05 for all) and mistimed insulin doses (p = 0.032) [32]. There was a numerically greater improvement in HbA1c from baseline to 4 weeks in the overall and active-use populations. In the ten people with full use of the Insulclock®, significant improvements from baseline were observed for TIR and glycemic variability (p < 0.05 for both). Of note, this study showed no difference in clinical outcomes between groups using the Insulclock® device with or without reminders and app alerts (active and masked groups, respectively).
Table 2 Results of clinical studies evaluating connection-enabled insulin platformsIn the RCT of 80 people with T2DM [28, 29], there was a significant improvement in HbA1c and glycemic variability from baseline to 12 weeks with the use of Insulclock®. People with T2DM reported a slightly higher number of hypoglycemic events during the study period with full use of the Insulclock® device compared to the masked device (29 vs. 25). However, the number of severe hypoglycemic events was equal in both arms (n = 1) [29].
PROs were reported in both RCTs evaluating Insulclock® (Table 2; details are provided in Supplementary Material Table S7). Overall, connected insulin caps were associated with improvement in the satisfaction of people with diabetes. In one RCT, people with T1DM reported improvements from baseline in most items of the Insulin Treatment Satisfaction Questionnaire (ITSQ) after 4 weeks of Insulclock® use, with the largest improvements observed for the items “perception of insulin treatment interference in work/school activities” (p < 0.05 in overall, active, and masked groups) and “potential of current insulin treatment for avoiding severe hypoglycemic episodes” (p < 0.05 in the masked group) [32]. People with T2DM were equally satisfied with Insulclock® with or without feedback, as assessed by the Diabetes Treatment Satisfaction Questionnaire change (DTSQc) survey [29]. Treatment adherence in this study (number of insulin injection irregularities) was reported to be similar for the device with and without feedback (Supplementary Material Table S7).
Similarly, improvements in PROs were observed after introduction of the Insulclock® or the GoCap® in observational studies (Table 2; details are provided in Supplementary Material Table S7). People with T1DM using Insulclock® reported a general benefit at follow-up as assessed by the ITSQ score [36]. Most people with T1DM or T2DM using the Bluetooth-enabled GoCap® found the cap was easy to use and useful in the management of their diabetes [34].
Connected Insulin PensOverall, results of observational studies in people with T1DM or T2DM showed improvements in clinical outcomes after introduction of a connected insulin pen (Table 2; details are provided in Supplementary Material Table S6). Use of NovoPen® 6 improved various clinical outcomes, such as HbA1c, missed bolus dose (MBD), TIR, time below range (TBR), and TAR, from baseline and/or blinded use periods (p < 0.05) in adults with T1DM or T2DM [33]. When evaluated in children and adolescents with T1DM, use of the NovoPen® 6 was associated with a significant decrease in incidence of hypoglycemia (p < 0.001) and TBR (p = 0.03) at 12 months [37].
Adults and children with T1DM or T2DM who used the InPen® also reported a significant decrease in TBR 60 days post-InPen® initiation compared with 60 days pre-initiation (p = 0.0002), without a significant decrease in TIR [35].
People with T1DM or T2DM using the Bravo® pen plus blinded or unblinded CGM had fewer MBDs per day, fewer days with MBDs per month, a higher percentage of daily time in TIR, and lower HbA1c levels during the unblinded CGM study period when compared with baseline and to the blinded CGM study period [30, 31]. In this study, people with diabetes were more likely to have a higher confidence in hypoglycemia (measured by the Hypoglycemic Confidence Scale), less fear of hypoglycemia (measured by the Adult Low Blood Sugar Survey), increased health problem-solving skills (measured by the Hypoglycaemia Problem-Solving Scale), and lower illness perception (measured by the Problem Recognition in Illness Self-Management survey) during the unblinded real-time CGM study period than at baseline (Table 2; details are provided in Supplementary Material Table S7) [30, 31]. However, these improvements in PROs, measured using a variety of tools, were not significant.
Connected Insulin PlatformIn people with T1DM or T2DM who used the connected insulin system ESYSTA®, there was a significant reduction in HbA1c from baseline to 15 months (p < 0.001), without an increase in the number of hypoglycemic events or insulin dose [27]. These people also had improved QoL as measured by the Short-Form 36, with the greatest improvements observed in “physical pain” and “emotional role function” domains (Table 2; details are provided in Supplementary Material Table S7). The majority of people with diabetes (84%) and health care providers (93%) reported they would recommend the platform to others, and > 75% of people with diabetes continued using the system after the study [27].
Economic OutcomesThe two studies reporting relevant data indicated that use of connected pens and systems is potentially cost saving from an economic perspective (Supplementary Material Table S8) [51, 52].
In people with T1DM, the direct and indirect medical costs per person with diabetes were lower by €11,309 (Swedish Krona [SEK]124,270) and €34,009 (SEK373,725), respectively, for NovoPen 6® versus a nonconnected standard of care over a person with diabetes’ lifetime [51]. Higher treatment costs (due to a higher bolus insulin dose) with the connected insulin pen were offset by a lower cost of complications compared with standard of care. In the cost-effectiveness analysis, NovoPen 6® was a dominant treatment option relative to standard care from a health care payer and a societal perspective. The results of the base-case analysis were supported by the results of the sensitivity analysis, where changes to input parameters and assumptions did not affect the dominance of NovoPen 6® over standard care.
Using Markov model simulations, the use of the connected ESYSTA® platform by people with T1DM or T2DM was associated with €1238.85 per person savings when HbA1c was reduced by 2% (from 8 to 6%) in Germany [52]. The potential savings with the use of ESYSTA® accumulated to up to €31,852.48 for an individual with diabetes over time (time period not specified in the report).
Assessment of RCT and Observational Study QualityQuality assessments were conducted on fully published studies only, so that enough information was available to complete the assessment.
Using the NICE checklist, the published RCT of Gomez-Peralta and colleagues [32] was ascertained to be of low quality. The study was unclear regarding randomization and similarity of baseline characteristics between groups. There were imbalances between groups in study discontinuations and the authors did not specify how discontinuations were handled [32].
The quality of the two fully published cohort studies, assessed using the Newcastle-Ottawa Scale, was ascertained to be fair [33]. The studies were largely select groups, and none of the studies were truly representative of the general population. However, in these studies, secured records were used for the ascertainment of exposure. The studies were generally small with a limited number of people with diabetes. Follow-up of the cohorts was considered to be adequately long, and all the subjects were accounted for in the assessment of outcomes.
留言 (0)