
記住我





The protocol of this review follows the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols checklist (online Supplemental file 1) [32], and was registered at PROSPERO international register of systematic reviews (No. CRD42020205127). The method used for this protocol will be performed under the criteria of the Cochrane Handbook of Systematic Reviews of Interventions [33].
Criteria of studiesThere is no restriction on publication language or types. When there are studies reported in different languages other than Chinese or English, we will ask professionals for help.
Type of studiesWe will include all RCTs and quasi-RCTs of acupuncture for peripheral facial palsy. If there is a cross-over trial, we will only use the first phase data and outcomes for analyzing.
Type of participantsAccording to TCM theory, the causes of PFP such as Bell’s palsy or Ramsay Hunt syndromes are inseparable from “wind-evil”, so there are same features in treatment. All participants who are in the acute phase of PFP will be included regardless of gender, age, or race.
Type of interventionAcupuncture therapy including manual acupuncture, electroacupuncture, moxibustion, bloodletting, and fire needle around acupoints will be eligible, there will be no limitation on acupuncture points, stimulation techniques, stimulation methods, the depth of needle insertion, needle retention time, stimulation frequency, and so on. If there is a co-therapy with acupuncture, it is necessary to be consistent with the control group.
Type of controlBlank control, placebo, or treatment such as antiviral therapy, nutritional nerve therapy will be eligible. If both groups involve acupuncture, it is acceptable for the control group not to undergo acupuncture in the acute phase. Or if the control group applies a different acupuncture method from no matter techniques or depth, will all be eligible. To avoid interference from other TCM medication, the combination of Herbal treatment will be ruled out.
Type of outcomeWhen facial symmetry can be restored and how to reduce the sequelae of facial palsy are the most common concerns of outpatients. Thus, the primary outcomes will be the recovery rate of facial function, the time it takes to restore facial function and the odds of sequelae occurring (use House-Brackman scales, Facial Nerve Grading 2.0 and other related scales). Chronic facial discomfort can cause anxiety or depression, and emotional factors are integral to the treatment in Chinese medicine, our secondary outcomes will be psychological well-being and quality of life (use Facial Disability Index scale (FDI), World Health Organization Quality of Life Scale-Brief Form Questionnaire(WHOQOL-BREF)).
Patient and public involvementNo patient involved in the design, conduct parts of the research. Four of our outpatients permitted us to use their photos during acupuncture treatment as a more intuitive explanation of different kinds of acupuncture manipulation.
Search strategyEight major English and Chinese electronic databases will be searched: PubMed, Embase, Cochrane Library, Web of Science, CNKI (China National Knowledge Infrastructure), VIP (China Science Technology Journal Database), Wanfang Database, Sino-Med Database (including China Biology Medicine disc (CBM)). Search dates: from their inception to December 31th, 2022. LC will apply several strategy exercises in different electronic databases to adjust the sensitivity and specificity (online Supplemental file 2, the detailed search strategy in PubMed). Unpublished literatures such as conference report, dissertation, ongoing studies that meet the eligibility criteria will also be searched. CADTH Grey matters cheklist (www.cadth.ca/resources/finding-evidence/grey-matters), Chinese Clinical Trials Registry (www.chictr.org.cn) and Us National Institutes of Health Ongoing Trials Register (www.clinicaltrials.gov) will be searched to reduce potential publication bias.
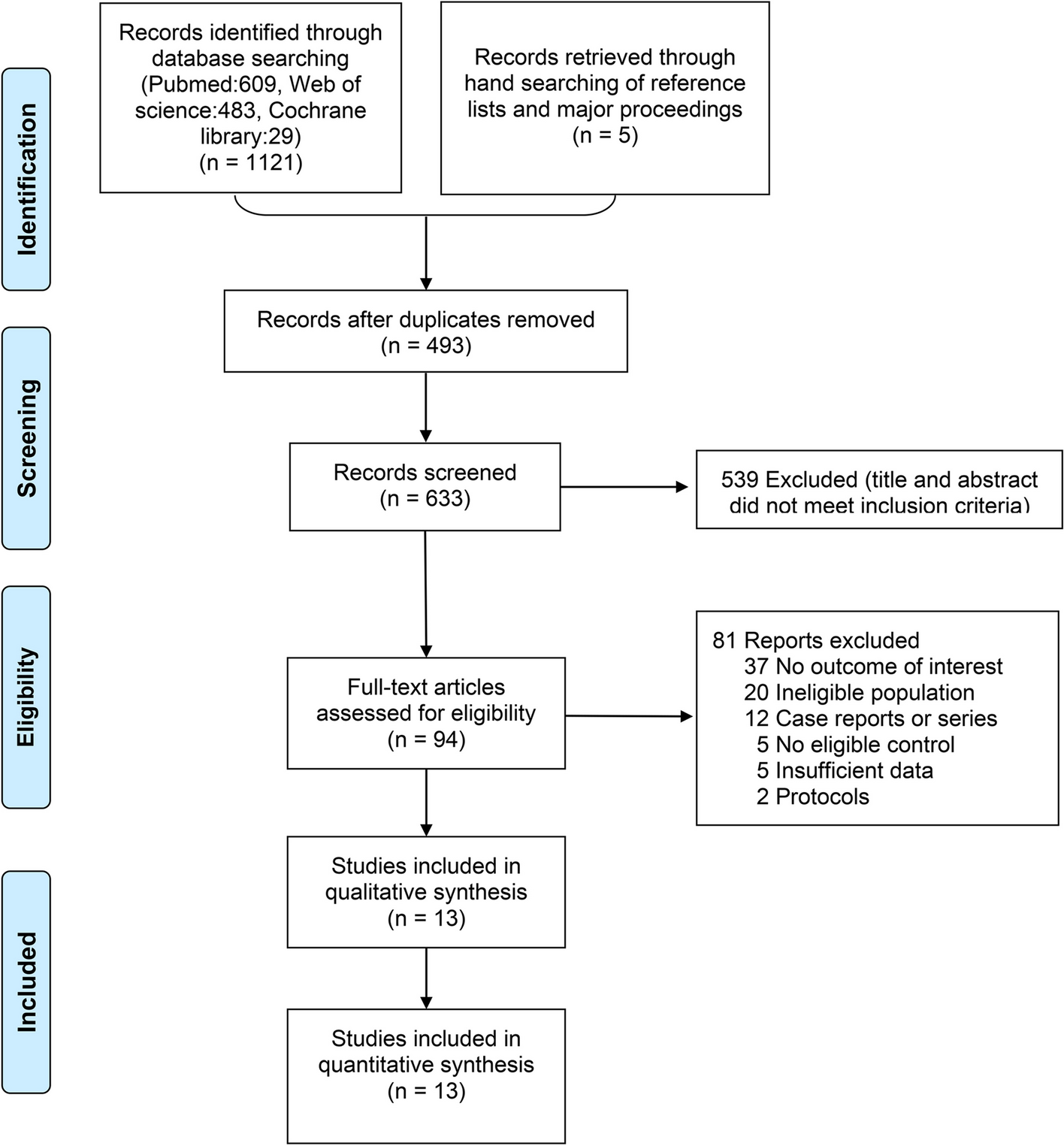
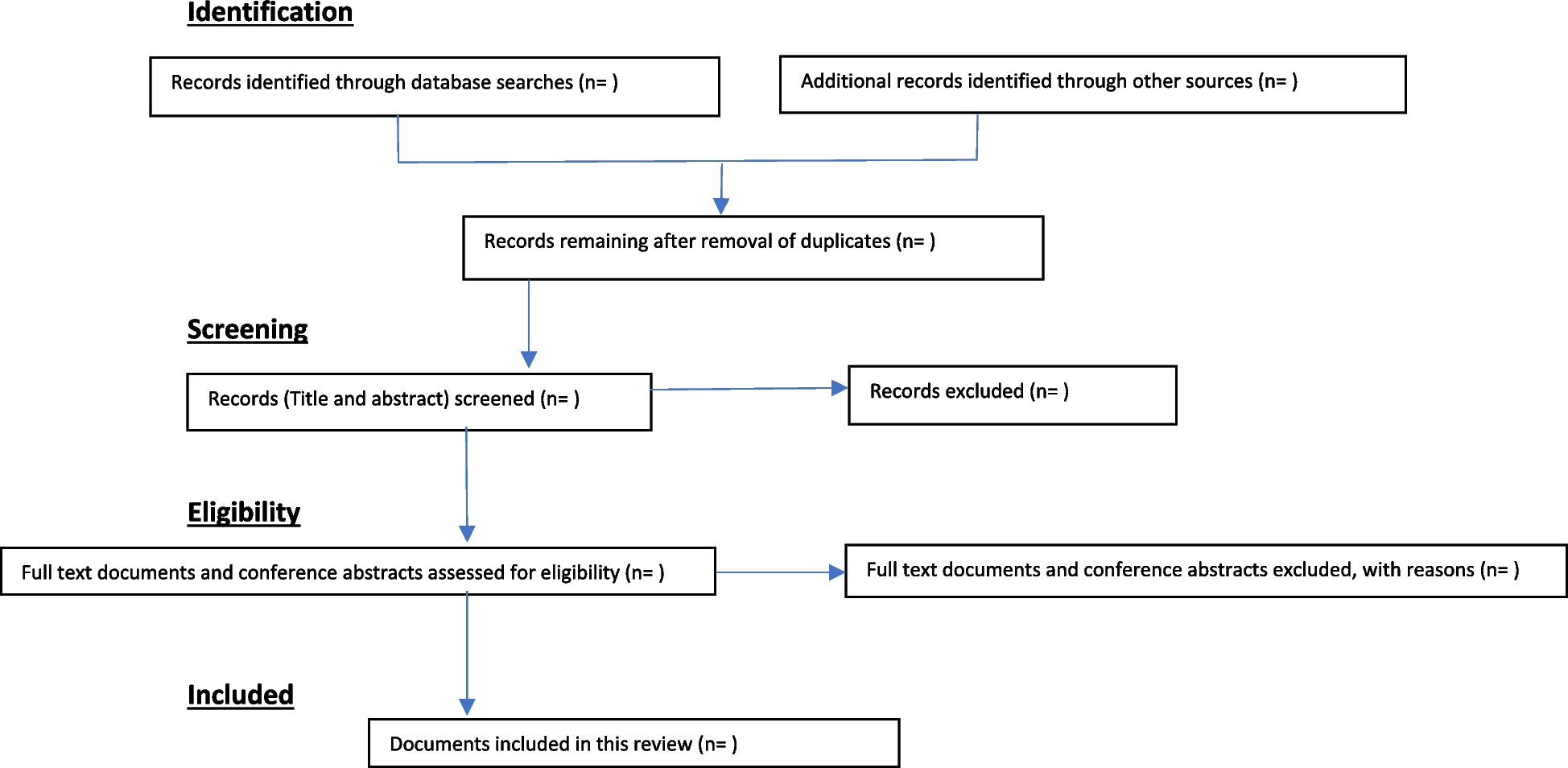
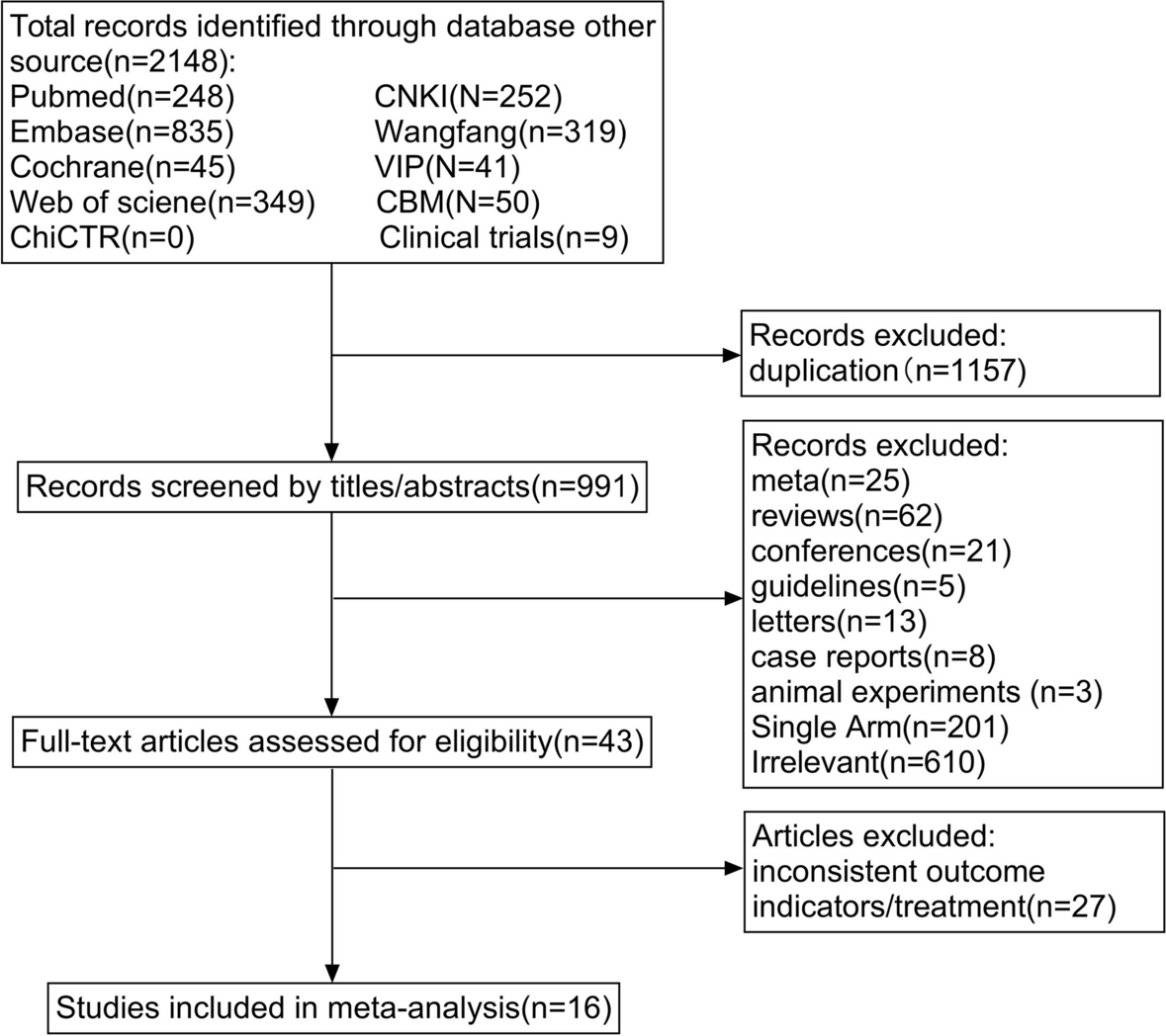
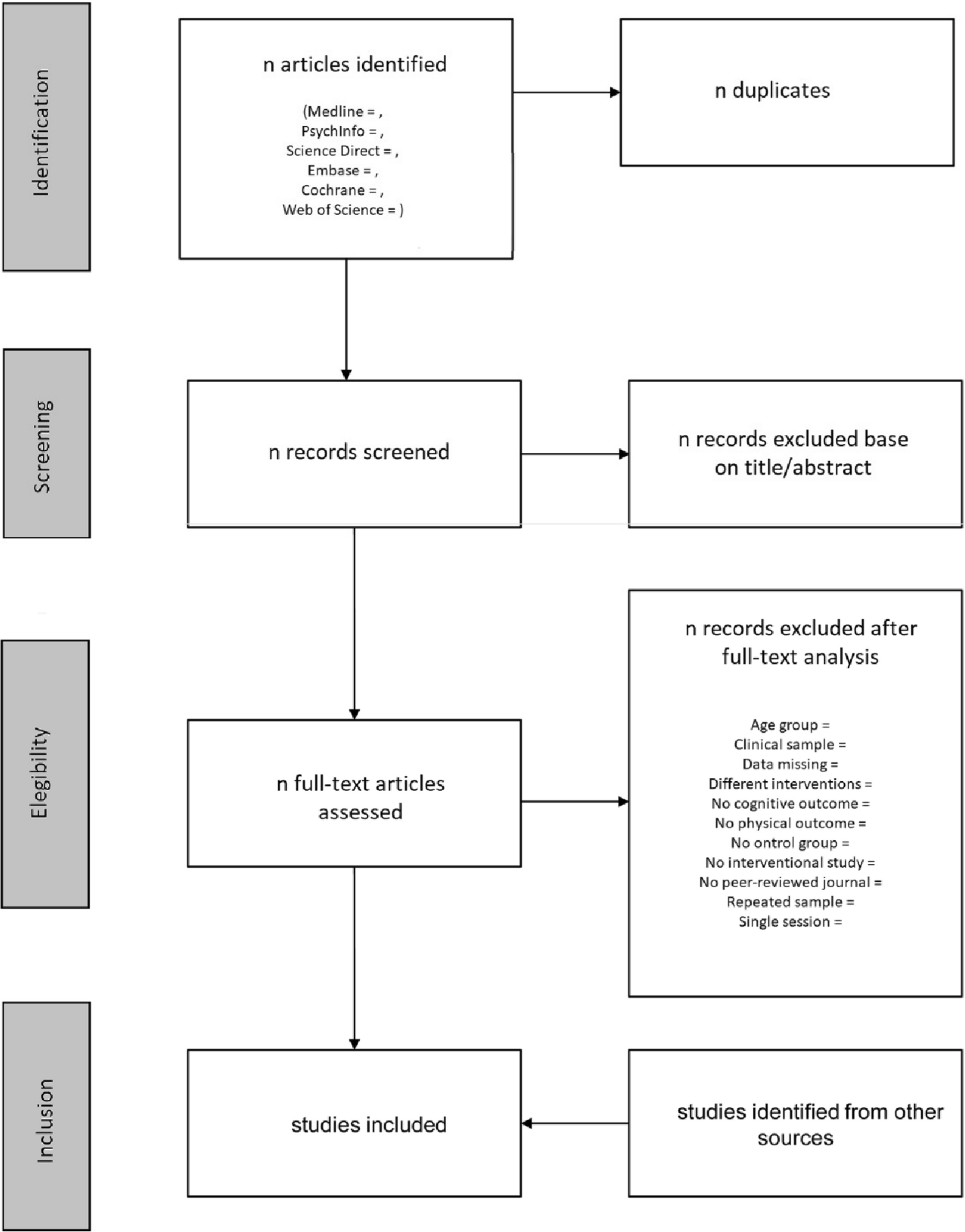
Selection of studiesWe will choose software such as EndNote and NoteExpress to manage studies searching from different databases. Two reviewers (XLL and YY) will respectively screen the title and abstracts according to the predefined criteria. Then full-text phases of the review will also be done by these two authors. If there are any disagreements, a third reviewer will join in and resolve them after discussion (Fig. 3).
Fig. 3
Flow chart of literature selection
Data extractionTwo reviewers (XLL and SQM) will extract the data independently from the included RCTs and quasi-RCTs by using EXCEL. The following information will be included: (1) Basic information of research: authors, year, title, diseases, corresponding author, contact details, reviewer’s ID, time of extraction. (2) Study designs: type of study, sample size, method of random number generation and allocation concealment, blinding, incomplete outcome data, selective reporting. (3) Patient characteristics: inclusion and exclusion criteria, age, gender, diagnostic criteria, severity, race, institution, baseline comparability. (4) Intervention group: type/form of acupuncture therapy, acupuncture points, manipulation, frequency, course of treatment. (5) Control group: control treatment, operation, frequency, course of treatment. (6) Outcomes: effectiveness outcome, safety outcome, efficiency. The discrepancies will be resolved by a third reviewer through consensus.
Quality assessmentTwo reviewers (SHD and SQM) will evaluate the quality of the selected studies independently according to the version 2 of the Cochrane risk-of-bias tool (RoB 2) for randomized control trials. The following domains of bias will be assessed: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, bias in selection of the reported result. By response signalling questions, and then give the risk of bias judgement [34].
Data synthesis and analysisIf studies are judged to be homogeneous, we will perform a meta-analysis. We will pool the data using risk ratio or odds ratio with 95% confidence interval (CI) for dichotomous outcomes, as for continuous outcomes, we will use standard mean difference or mean difference with 95% CI. The clinical heterogeneity will be assessed according to the characteristics of the included studies and participants, details of the intervention or control, types of outcome measurements will also be analyzed. The I2 statistic will be used to assess the heterogeneity. According to the Cochrane handbook, when I2 is between 0 and 40%, 30 and 60%, 50 and 90%, and 75 and 100%, the heterogeneity will be regarded as not important, moderate, substantial, and considerable. We will use the random-effects model to conduct the meta-analysis unless the I2 statistic is 75%. When there is substantial heterogeneity, we will try to investigate possible causes from clinical perspectives. Subgroup and sensitivity analysis will be conducted. Forest plots will show the results of the meta-analysis, and if there are more than 10 included studies, funnel plots willed be used to identify publication bias.
Subgroup analysisFor facial paralysis, there are different severity and TCM syndrome; for intervention, there are different types of acupuncture therapy; and there are different types of the control group. These all can lead to heterogeneity. To explore the treatment effects respectively, we plan to conduct subgroup analysis for different severity, syndromes, acupuncture techniques (such as manuacupuncture, electroacupuncture, a combination of a different method, different stimulate of acupoint, different acupoint selection, different depth of needling), control group, and other possible factors.
Sensitivity analysisFor the main outcome with important positive significance, when the literature conditions are met, the random method is compared according to the methodological quality of the literature. Clear/unclear, double-blind use or not; when the combined results are in a critical state and the heterogeneity is small, compare results of random effects model and fixed effects model. If necessary, leave each study out to assess the weight of the research.
Quality of the evidenceSummary of Findings (SoF) table will be generated by the GRADEpro Guideline Development Tool (GDT). The SoF tables will show the overall quality of the body of evidence. Whether to upgrade or downgrade the level of the evidence will according to the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) criteria [35]. Study quality limitations, inconsistency of effect, imprecision, indirectness and potential publication bias will downgrade the quality of the evidence.
留言 (0)