
記住我









Four major themes that emerged from the qualitative data were: 1) Strong parental control, 2) Compulsive asexuality, 3) Perceived negatively different from peers, and 4) Angry ALPHIV.
Strong parental controlCaring of a child having a chronic, life-threatening, and socially stigmatized illness was a challenge for the parents/guardians, inciting fear which provoked overprotective and hypervigilant parenting practices, and over-controlling behaviors among the parents. Both the ALPHIV and the parents/guardians reported similar controlling behavior towards their HIV-positive wards such as putting restrictions on peers, school trips, and other social activities. These were also endorsed by the health care providers.
“My mother does not allow me to go with friends as she is scared because ART is going on.” (AD-03, ALPHIV)
A mother shared, “I do not send her [/daughter/] anywhere because if someone would do bad behavior with us [/stigmatize us/]. Whenever [she] has to go somewhere, anywhere like has to go on a trip, I go with her. I do arrangements like this so that I stay with her.” (CG-08, Mother).
“Only thing is there has been a lot of over protection from the parents where they are worried… anxiety is the reason for the overprotection by the parents.” (HCP-18, Adolescent physician).
It has been found that parents/guardians become so hypervigilant that they tried to keep an eye on the activities of adolescents because of the inherent stigma associated with HIV.
“She [/daughter/] does not go anywhere alone I always accompany her… No, I do not send her… I always accompany her wherever I take her… do not send her [/daughter/] alone.” (CG-10, Mother).
Similarly, a guardian of ALPHIV shared: “We send him = XXX = [/brother’s name/] or uncle with her [/ALPHIV/]… to see what she is doing at friend’s place. She [/grand-daughter/] is not allowed to go alone”. (CG-04, Guardian).
The controlling behavior of parents/guardians emerged in the need to maintain secrecy about HIV diagnosis to protect their wards from stigma and discrimination. This hypervigilant behavior of parents/guardians seemed to result in captive isolation of ALPHIV.
Compulsive asexualityHCPs explained that sexuality is one of the crucial elements of adolescent development and ALPHIV is no exception.
“It’s a normal phenomenon. Getting involved in sexual relations during teenage. Because the adolescence is the phase to explore and experiment”. (HCP-16, Mental Health Expert).
“This [/sexuality/] would be [same]. They [/ALPHIV/] do the same as any other adolescent. It is not related to HIV, it [/sexuality/] would be same [/for all adolescents irrespective of HIV/].” (HCP-08, Programme Personnel).
The parents/guardians not only controlled ALPHIV's social activities but also seemed to control their sexuality and intimate relations.
“See, your father had done such and such [/multiple sexual relations/]… So this [/HIV/] happened because of going outside [/by keeping sexual relations outside/]. So you do not do this mistake.” (CG-03, Guardian).
One of the ALPHIV also shared that her mother controls the intimate relationships.
“Mother has warned me before only that if she comes to know anything about this [/about having boyfriend/], she will not talk to me. I am scared about this” (AD-01, ALPHIV).
Another ALPHIV shared her worries on marriage and stress of unfulfilled dream.
“I am crazy about my marriage from my childhood. Means marriage is my dream. I want to do this and that is my marriage. Now [/after knowing about HIV/] my marriage will not happen…Only I was feeling that I will not get married now.” (AD11, ALPHIV).
The uninfected counterparts of ALPHIV also had strong views about an ALPHIV thinking of having intimate sexual relationships. Stigma seemed to emerge. On asking what would be their reaction if an ALPHIV approached him/her for intimate relationships; the adolescent shared she would admonish as follows:
“I would have told her [/HIV positive friend/] 'No' [/for intimate relationships/], and tell her not to make a physical relationship like this [/in presence of HIV/]”. (AD-07, HIV-uninfected adolescent).
“There are chances of others getting infected then. The person with whom the infected person marries will get infected. And then when married, they will have kids as well and then they [/children/] will be infected too. That’s the reason they shouldn’t marry”. (AD-09, HIV-uninfected adolescent).
Any reference to safe sexual behavior was missing. ALPHIV pointed out the gap in counseling sessions on safe sexual practices.
“They [/ART counsellor/] did not talk about precautions [/for safe sex/], just told how it [/HIV/] spreads and in that only told about sexual relations [/as one of the modes of HIV transmission/]” (AD-12, ALPHIV).
Some parents/guardians of ALPHIV tended to communicate on developmental changes, especially, reproductive and sexual health (RSH) during adolescence with their ward to caution them about transmitting the infection to others. However, communications about RSH are not initiated with uninfected adolescents. A parent of an ALPHIV son and uninfected daughter responded:
“We have this [/HIV/] but it should not happen to others. So if a girl is normal and you make relations with her, then it is wrong. I told my son [/about not having sexual relations/], not my daughter.” (CG-07, Mother).
It is only to keep the ALPHIV asexual or to abstain from sexual exploration, it was evident that parents/guardians of ALPHIV communicated with them about sexual relations. However, such communications in general are avoided and considered taboo in Indian society.
“A larger number of parents-they maintain a distance with their adolescent children. Sometimes they do not feel like answering their queries, [as] it might be related to a sensitive issue.” (HCP-16, Mental Health Expert).
Perceived negatively different from peers (PNDP)ALPHIV felt that they were different from their peers. Developmental delay, fear of being identified as sick or HIV positive and captive isolation by parents/guardians instilled fear of losing peers and the possibility of rejection from peers resulting in negative self-perception. Frustration, isolation, and self-stigma were voiced by the ALPHIV in this study.
“Why only I have this disease? Why do you [/uninfected sister/] not have it as well?” (AD-03, ALPHIV).
An HCP brought this feeling of being different in a negative sense very eloquently: “Diseases which are long term in their course, which has an impact not only on their [/adolescents'/] day to day life but also, on their functioning. So, because of this, many of these [/HIV infected/] children might see themselves as little different from their peers or siblings.” (HCP-07, Mental Health Expert).
Another HCP echoed the same: “There is this peer pressure. So they do not want to be different from the crowd. Therefore, they do not want to be seen taking medicines by their friends.” (HCP-20, Paediatrician).
HCPs concurred with the voices of ALPHIV and explained that the impact of disease on their daily routine and peer pressure brought the feeling of being ‘different’.
“Adolescents, otherwise, is a very healthy phase of life, and therefore, if you are sick, having to take medicines; you are going to always feel that you are different from all other peers and that might affect your self-esteem, and affect your sense of self.” (HCP-19, Mental Health Expert).
HCPs emphasized that peers are critical for adolescents' social development and that is why fear and stigma of being identified as HIV positive exists strongly among ALPHIV. This impacts their psychosocial functioning and results in social withdrawal and anger.
Angry ALPHIVAdolescence is a phase of knowing about the unknown. Of course, ALPHIV become curious about their illness, medications, and their impact on their future aspirations. The following subtheme ‘blaming/questioning parents' behavior’ reflects anger against parents.
Blaming/questioning parents' behavior: Once ALPHIV understands the modes of HIV acquisition, especially the sexual transmission mode; it brings curiosity into the mind of adolescents which raises suspicion about the parents' behavior. A mother shared the questions asked by her son:
“Mother, this HIV I got from you or because of father? You have this [/HIV/], means did you get it from father or outside?” (CG-07, Mother)
Adolescents start blaming their parents, especially their father as the source of illness in the family. This affects their relationship with their parents.
“I came to know that it [/HIV/] came through him [/father/] to me. Then, inside, I thought why he did it?” (AD-01, ALPHIV)
“About my parents… I was too much angry with my father. Because of him [/father/], mother got [HIV] and they both went [/died/]. But I feel that if my father had not got it [/HIV/] then my mother also would be alive and I also would have been ok. Why would I have to take these two tablets?” (AD-11, ALPHIV)
Key informants tried to explain how an ALPHIV processes the information about HIV transmission:
“Given the huge stigma around HIV, if an adolescent comes to know that s/he is infected because of his parents, the very first issue that s/he would face is to deal with the information that why did my parents get infected? Why not the other’s parents? So, is there anything wrong with my lineage itself, and who was wrong? My mother was wrong or my father was wrong? And it all depends on where it comes from and at what stage it is [/how disclosure was done/]. He might feel that others and peer groups will feel that he comes from parents who are not 'morally correct'. That’s the shaming and blaming…” (HCP-12, Social scientist)
“This is the basic problem when at that [/adolescence/] age if they [/adolescents/] get to know their [HIV] status; they [/adolescents/] always know now something about sex. So every time they know that their parents have done some ‘bad activity’; that is why they [/parents/] got [HIV] and we [/adolescent/] got [HIV] because of that.”(HCP-03, Program Personnel)
HIV impacts not only the adolescent-parent relationships; it also affected their future aspirations viz. academics, peer relations, intimate relations, and marriage. This reflects in another subtheme 'Unfulfilled aspirations'.
“There is too much effect on my studies so I get angry, irritated. That's why I have started this [/ART/]. It also scares me that what if I will not be able to achieve my goal.” (AD-01, ALPHIV)
The interruptions in education are common as shared by an HCP:
“A lot of children leave school because of issues related to stigma and discrimination. That is the first impact. Number 2 impact is a lot of times especially before they [/ALPHIV/] start ART and in the initial time they deteriorate despite taking medicine, school absenteeism because of repeated illnesses [/opportunistic infections/]… not only missing school if they just don’t have the energy how do they study. The third impact could be just related to their [/HIV acquisition through parents/]… because perinatal HIV impacts upon the mental development of a child.” (HCP-11, Paediatrician)
“They [/ALPHIV/] are not able to go to school regularly when they have to come to the hospital frequently…They are very intelligent children but they are not able to spend that much time on their studies.” (HCP-10, Mental Health Expert)
When adolescents start understanding HIV as a sexually transmitted disease, they worry about their marriage and the transmission of their infection to their offspring. Visualizing unfulfilled dreams and fear of secondary transmission tended to provoke angry feelings among ALPHIV.
“I was very much angry on father. But now in my marriage, it [/HIV/] is a barrier and I have only the tension of this thing.” (AD-11, ALPHIV)
A mother shared the conversation that she had with her HIV-infected son:
“My son became very angry and said because of father, you got HIV and I also got this. Now my children will also get this [/from me/].” (CG-07, Mother)
The HCPs agreed with the emotions of ALPHIV pertaining to their sexuality.
“In adolescents, sexuality is a very key element of identity and if that issue of sexuality is going to be inevitably influenced by the fact that you have a disease that can be transmitted sexually, how that impacts on your mental health particularly.” (HCP-19, Mental Health Expert)
The dilemma, fear, concerns, and anger led to a critical need for counseling aptly indicated by an HCP as follows:
“I think they [/ALPHIV/] also need to be counseled about that they can have a normal life, they can get married; they can have children who can be negative. So they can be absolutely normal individuals like anyone else in the society.” (HCP-20, Paediatrician)
Using these evidences from qualitative research, a survey instrument was developed to conduct a cross-sectional survey to understand the relationship between emotional distress and other psychosocial factors among ALPHIV.
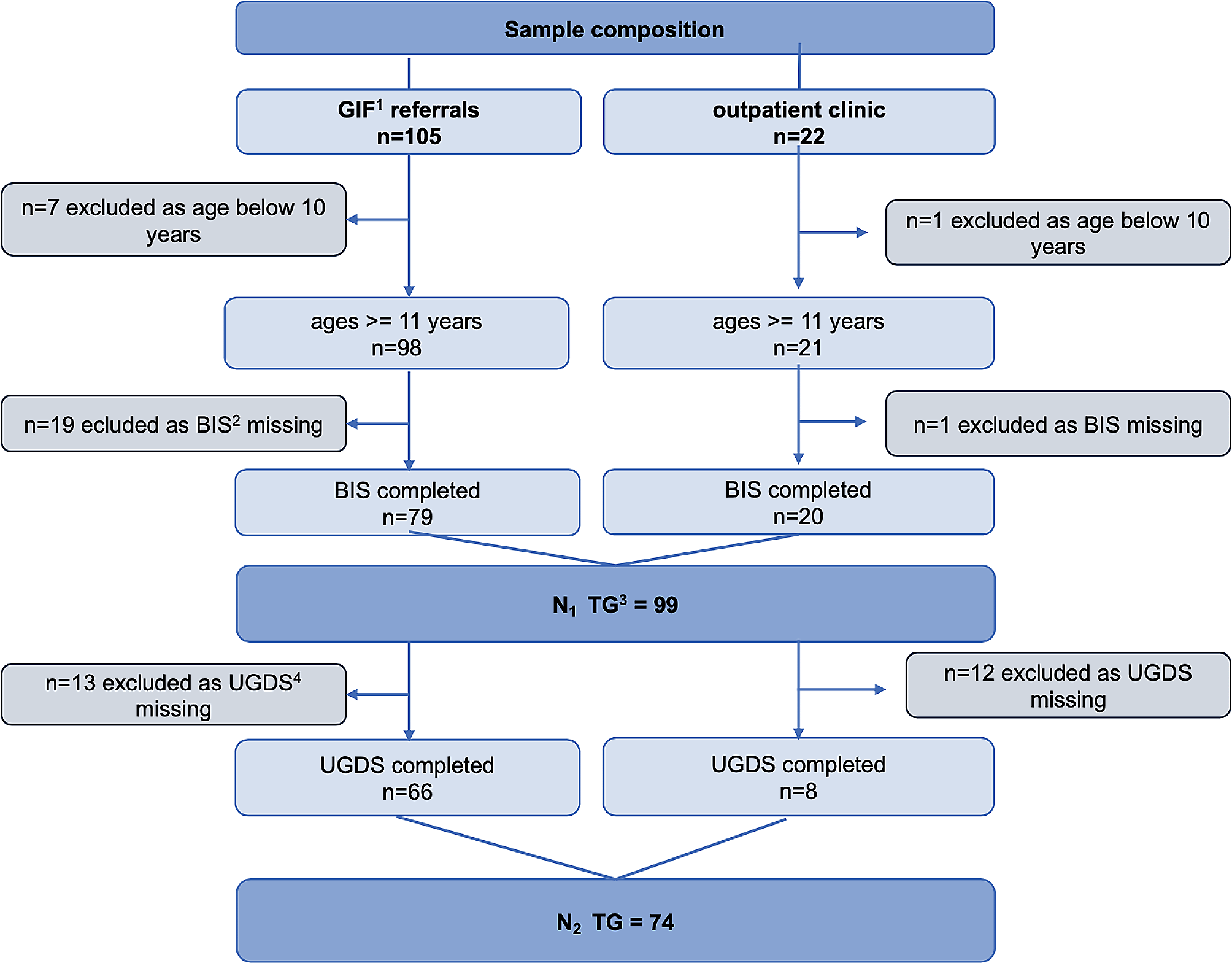
Profile of quantitative survey participantsA total of 117 ALPHIV were screened, eligible 100 ALPHIV participated in the survey. The mean age of adolescents was 14.95 years (2.57 SD), 18% had dropped out of school, 67% lived in a nuclear family, and 24% considered themselves ill; 69% were aware of having a chronic illness, 52% were aware of their HIV infected status, and 17% had negative perception; hence categorized as PNDP. The mean score for ED was 23.38 (7.81 SD). Table 1 presents the mean scores of psychosocial domains. In the bivariate analysis, PNDP, body image, anger, APR, hypervigilance, and parental control were significantly associated with ED (Table 1).
Table 1 Participant demographics and correlates of emotional distress among adolescents living with perinatally acquired HIV (ALPHIV)In the multivariable analysis (Table 2), PNDP predicted an increase of 0.19 standard deviations in ED compared to the adolescents who did not perceive themselves as different from their peers.
Table 2 Association between emotional distress (ED) and correlates using multivariable analysisThe relation between PNDP and ED was evident in the qualitative phase as an ALPHIV shared: “Sometimes it feels like we are different from others because others do not accept us freely…If we can share about this with somebody, then they may not be [/friends/]with us.” (AD-12, ALPHIV).
Anger and ED coexisted as an HCP narrated about his ALPHIV patient who shouted at his parent saying: “I got my disease because of you [/parent/]”. In response, the HCP shared with the interviewer:“Because they [/ALPHIV/] start getting to know how HIV has happened?” (HCP-09, Paediatrician).
In the multivariable analysis, this fact was confirmed. Experiencing anger was associated with ED, meaning an increase of one unit in ‘anger’ was predicted to be an increase of 0.25 SD in ED. Additionally, body image and hypervigilance were significantly associated with ED. A mental health expert opined that parents’ hypervigilance could translate into mental health issues among ALPHIV:
“For HIV even if parents are supportive, they themselves have fear about the larger societal acceptance because of which that [/fear/] might get translated in their reactions to the child… it might develop into some kind of behavioral problems or depressive or anxious personality.” (HCP-07, Mental Health Expert).
Informed by the theoretical evidence [29,30,31], qualitative findings from our study, and factors identified in regression analyses, we explored separate mediation and moderation models to assess whether anger, body image, and hypervigilance explained the relationship between PNDP and ED.
PNDP had a statistically significant effect on anger (path a). The effect of anger on ED was also statistically significant (path b) (Table 3). The indirect effect (path ab) of anger was found to be statistically significant on the relationship between PNDP and ED. The total effect (path c) of PNDP on ED was also statistically significant when anger was tested as a mediator. The ALPHIV did demonstrate their distress and anger because of their body image in the qualitative interviews as follows:
“He [/son/] tells about his height as his height is less. So, he asks always what did you eat when [uninfected] sister was in your stomach and what did you eat when I was in your stomach? So he tells me that I had not taken proper care at his time [/during pregnancy while when daughter was conceived she had taken proper care/]”. (CG-07, mother).
Table 3 Total, direct, and indirect effects of psychosocial factors on the relationship between PNDP and emotional distress using mediating effect analysisFigure 1 shows the pathways explaining the role of anger as a mediator between PNDP and ED.
Fig. 1
Mediating Effect of Anger on Emotional Distress
Subsequently, body image and hypervigilance were tested for the potential role of mediator. In the model testing body image as a mediator, a statistically significant mediating role between PNDP and ED emerged. However, as PNDP is not causally antecedent to body image, a condition that is required to consider a variable to be a mediator [32]. Therefore, the role of body image as a mediator was rejected. For the model testing hypervigilance as a mediator, the indirect effect (path ab) on the relationship between PNDP and ED was not statistically significant.
ALPHIV seem to be traumatized about their bodies. Most of them were dissatisfied and worried as seen in the following excerpt:
“People at home used to say that I looked very much like a bamboo stick, dresses do not look good on me.” (AD-11, ALPHIV).
In the moderation analyses too, body image was identified as a significant moderator for the relationship between PNDP and ED as the product term (PNDP x body image, XM1, Path c) was statistically significant (Table 4).
Table 4 Moderating effect analysis of psychosocial factors on the relationship between PNDP and emotional distressThe conditional effects of PNDP on ED were significantly different at the three levels of body image. Among the ALPHIV who had body image scores one SD higher than the mean, the relationship between PNDP and ED was statistically significant (5.80, 95% CI: 1.87 – 9.71). However, the relationship between PNDP and ED at the mean score (2.40, 95% CI: -1.53 – 6.33) and one SD below the mean (-0.98, 95% CI: -6.85 – 4.90), were not statistically significant (Fig. 2a).
Fig. 2
Moderating Effect of body image and hypervigilance on Emotional Distress. Figure 2a. Conditional effects of PNDP on Emotional distress at values body image. Figure 2b. Conditional effects of PNDP on Emotional distress at values of hypervigilance
Parental control and assuming ALPHIV to be asexual being had led to the emergence of ED in the qualitative phase. Hypervigilance emerged as a significant moderator for the relationship between PNDP and ED (Table 4).The conditional effects of PNDP on ED were significantly different at three levels of hypervigilance (Fig. 2b).
For the ALPHIV who reported hypervigilance one SD more than the mean (9.82, 95% CI 5.59–14.05) and at the mean (6.70, 95% CI 3.40–10.00), the relationship was significant. However, the effect of PNDP on emotional distress at hypervigilance score one SD below the mean (3.58, 95% CI − 0.98–8.14) was not significant. Therefore, among ALPHIV with mean and greater than mean levels of hypervigilance from parents/guardians, the effect of PNDP on ED was significantly stronger.
Anger was not found to be statistically significant as a moderator (PNDP x Anger, Path c, B = 0.32, p = 0.093) for the relationship between PNDP and emotional distress. Therefore, the final emerging model shows that anger explains the mediating mechanism while body image and hypervigilance have moderating effects on the relationship between PNDP and emotional distress (Fig. 3).
Fig. 3
Model showing pathways leading to Emotional Distress among ALPHIV
留言 (0)