Clinical setup
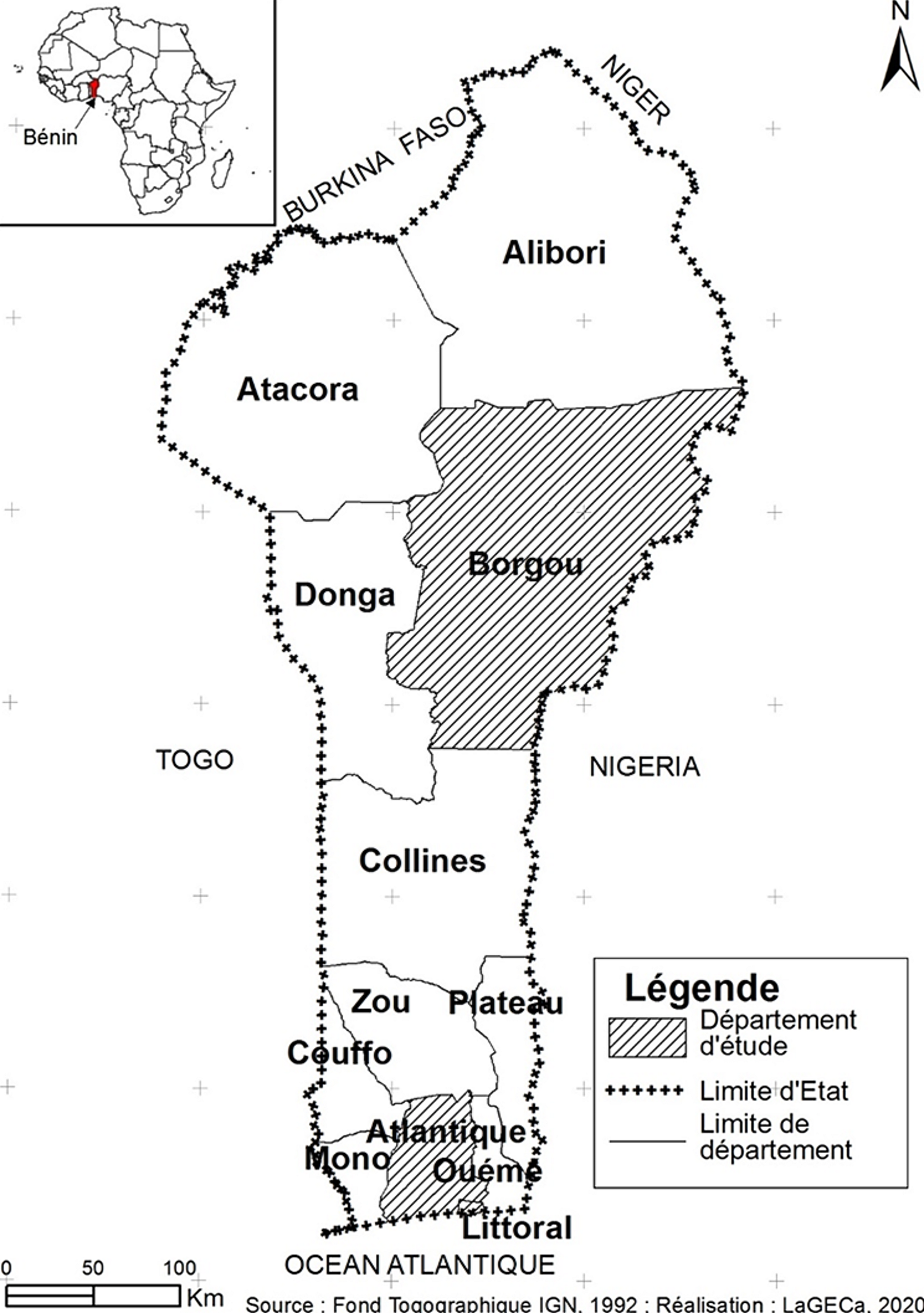
The Israeli National Health Insurance Law requires all citizens to join 1 of 4 official non-profit health insurance organizations (HMO), which cannot legally deny membership. The Clalit Health Services (CHS), the largest Israeli HMO, divides Israel into different geographic regions; access to health services is similar for residents of each region [5]. To eliminate supply-side heterogeneity [6], we included patients residing in the southern region in our study. The Negev is the southern region of Israel, and the largest city in that region, Beer-Sheva, is considered the capital. This region includes 730,000 residents, which represents 8.2% of the Israeli population; 75% of residents are Jewish and 25% are Bedouin. In the Negev, municipal communities are ethnically homogenous. The largest health care provider in that region is the CHS, which covers approximately 67% of the region’s residents and has primary clinics available in every city, town, or settlement. The largest regional hospital in the Negev is the Soroka University Medical Center (SUMC), which is part of the hospital network for the CHS. SUMC is a tertiary 1100-bed care medical center that has > 65,000 yearly hospitalizations and approximately 200,000 yearly emergency department visits. This setup, with a single hospital serving a large region, permitted a population-based analysis, with few patients lost to follow-up and limited referral bias.
Study population and data collection
This population-based retrospective, observational, cohort study included adults (≥18 years) with migraine in the southern district of the CHS. Patients with migraine were dentified using the CHS computerized database based on a recorded physician diagnosis (International Classification of Diseases, Ninth Revision [ICD-9]) of migraine (with or without aura) and/or claims for specific anti-migraine medication (triptans) at any time from 2000 to 2018. The study cohort was created in 2 steps: first, patients with physician-diagnosed migraine by a primary care provider or neurologist were identified (16,675 patients with or without triptans prescription), and second, of those without physician-diagnosed migraine, patients with a triptan prescription were identified (14,091 patients). Overall, 71.8% of patients with physician-diagnosed migraine were also prescribed triptans. Although used off-label for cluster headache treatment [7], triptans are migraine-specific [8] and are only approved in Israel for the acute treatment of migraine, which is the far more common indication. Thus, it can be assumed that the included patients with triptan prescriptions were being treated for migraine. Physician-assigned migraine diagnosis was given by either a primary care physician or neurologist. Migraine diagnoses assigned by primary care physicians were found to be highly reliable. The Landmark Study demonstrated that clinic-assigned diagnosis of migraine was validated by an expert panel based on diary data in 98% of cases [9].
The following patient demographic and clinical characteristics were collected from the central CHS computerized database: gender, age at the time of diagnosis, ethnicity, family status, education, social state score, immigrant status, comorbidities, medications, hospitalization notes, diagnostic imaging, and primary care physician visits.
Municipality characteristics were identified using data published by the Israeli Central bureau of statistics 2018 [10]. Geographic, demographic, socioeconomic, and environmental data were used for these analyses. The socioeconomic index (SEI) was used to define socioeconomic characteristics for each municipality. Each municipality was scored on the following 14 variables on a scale of 1 to 255 (1 is the lowest): average monthly income, vehicle class, new vehicle percentage, percentage of high school graduates, students, percentage of residents seeking work, percentage of residents with minimum monthly income, percentage of residents with > 2 times the average monthly income, median age, dependency ratio, percentage of families with ≥4 children, percentage of unemployment benefit recipients, percentage of income support beneficiaries, and percentage of old-age pension recipients. Based on this score, municipalities were aggregated into SEI clusters from 1 to 10 (low [1–3], medium [4–6], and high [≥7] socioeconomic status). We also used the Gini index, a measure of statistical dispersion intended to represent income inequality. The characteristics of primary care physicians practicing in CHS clinics in the different communities were provided by CHS administration.
Statistical analysis
Data for the main variables were summarized as means and standard deviations (SDs) for normally distributed quantitative variables, medians and ranges for non-normally distributed quantitative variables, and distribution in percent for qualitative variables.
Univariate analyses were primarily used for analyses of initial personal data record datasets. For categorical variables, we used a chi-square test, with a Fisher’s exact test when needed. For continuous variables, we used a t-test for normally distributed variables, and a Mann-Whitney U-test for non-normally distributed variables.
The 2018 migraine prevalence per 10,000 adults was calculated for the overall population and each individual municipality; all calculations were made by division into the total population and female and male subgroups separately. The prevalence for each 5-year age interval was also calculated, and a standardized (age and gender) mortality ratio (SMR) approach was used for comparison among the municipalities. In addition, we calculated the female-to-male ratio of the various municipalities. These calculations were performed to examine the linear and non-linear correlation between the results of the SMR and female-to-male ratio analysis and number of variables from the Israel Central Bureau of Statistics using Pearson and Spearman tests, respectively. We also examined the correlation between the same results and a number of the physicians’ variables.
This analysis also looked at current management practices and potential gaps in the management for migraine using this study cohort. The migraine population was stratified by the source of the migraine diagnosis: physician diagnosis and/or triptan prescription. Rates of acute medication use were compared for specific (triptan [Anatomical Therapeutic Chemical (ATC) code NO2CC01–7]) and non-specific (combination pain drugs including Acamol Focus, Excedrin, Migraleve, and Rokacet Plus [ATC code NO2BE72 and NO2CX50] and opioids drugs [ATC code NO2AJ17, NO2AX02, and NO2AA55]) medications used ≥1 time during the study period for each indication.
In the last step, we performed a univariate logistic regression. The outcomes of interest were high-rate SMR (cutoff, 1.0) or high female-to-male ratio (cutoff, 3.0). The cutoff point was based on the average adjusted prevalence in the region. We have dichotomized all regional municipalities into 2 groups: high and low migraine prevalence and high and low female-to-male ratio. The model presents municipality-related characteristics associated with equal or higher than average SMR and equal or higher than average female-to-male ratio. Point estimates of association were presented by the odds ratio (OR) along with their 95% confidence intervals (95% CI).
RStudio®, version 1.4.1717 (Boston, MA), was used for these analyses. A 2-sided P value < 0.05 was considered statistically significant for all analyses.
Ethics approval
Clinical investigations were conducted in accordance with the Declaration of Helsinki. The SUMC Ethics Committee (EC) provided approval for this study (reference number 0284–19). Informed consent was waived by the SMC Institutional Review Board based on the EC approval, which determined that informed consent was not needed based on the retrospective nature of the study and use of fully anonymized and deidentified patient data for analysis.



留言 (0)