A monofocal intraocular lens (IOL) is a medical device implanted in the eye to restore distant vision in eyes with cataract. Beyond monofocal IOLs, other technologies such as simultaneous vision lenses (SVL) have also been developed to restore intermediate and/or near vision. SVL have been historically classified as multifocal IOLs, for which the light is split into multiple foci, and extended depth of focus lenses (EDoF), for which the far-distance focus is extended [1, 2].
A new technology named Tecnis Eyhance (Johnson & Johnson) was introduced in 2019 which as EDoF lenses extend the far distance focus [3]. Since this technology extends the depth of focus in a similar way to EDoF lenses, some confusion emerged among anterior segment surgeons, some declaring this lens as EDoF even though the IOL was launched as a new generation of monofocal intraocular lens. Subsequently, other IOLs with hypothetical similar visual performance were launched, and a new category popularly known as plus monofocal, mono-EDoF, or enhanced monofocals appeared. The new generation of monofocal IOLs that enhance intermediate vision might include Tecnis Eyhance (Johnson & Johnson), IsoPure (Physiol), Xact (Santen), Zoe (OphthalmoPro GmbH), RayOne EMV (Rayner), Lentis Quantum (Teleon Surgical), Evolux (Sifi), Vivinex Impress (Hoya), and Extend HP (Hanita Lenses).
Standards have not yet considered these lenses as a new category of SVL; therefore, they should still be classified as monofocal or EDoF lenses. The definition of EDoF has been reported by the American National Standard Z80.35–2018 (ANSI) [4], and describes up to four effectiveness end-points that should be met in full for classifying an IOL as EDoF, between them: (1) to demonstrate a statistical superiority over a control monofocal group on mean, monocular photopic distance-corrected intermediate visual acuity at 66 cm; (2) to demonstrate at least 0.5 D greater monocular photopic negative lens induced distance-corrected depth of focus compared to the monofocal control IOL at 0.2 logMAR visual acuity threshold; (3) the median, monocular distance-corrected photopic intermediate visual acuity at 66 cm is at least 0.2 logMAR, and (4) the mean, monocular photopic best corrected distance acuity for the EDoF IOL is statistically non-inferior to the control using a non-inferiority margin of 0.1 logMAR [4].
Unfortunately, the standard described by the ANSI requires comparison with a monofocal IOL in a randomized clinical trial, [4] and common published post-marketing studies are case series without a control lens. A case series without a control group does not allow for the evaluation of requirements 1, 2, and 4, as described by the ANSI. In addition, the descriptive statistic of the median described in the third requirement is not always reported since clinical studies usually offer a mean value. The inclusion of other absolute end-points instead of a relative comparison with a monofocal intraocular lens would help to describe the functional performance of the IOL from case series studies without a control group. Furthermore, these absolute values are expected to be included in future standard updates [5].
A preliminary search was conducted and two systematic reviews on the topic were identified [6, 7]. The purpose these reviews was to assess the efficacy, spectacle independence, patient satisfaction, and adverse event rates in comparison with monofocal IOLs. These systematic reviews concluded that new enhanced monofocal IOLs increased the intermediate and near vision in comparison to conventional monofocal IOLs, [6, 7] without compromising the contrast sensitivity or inducing photic phenomena [6]. These reviews required a narrow scope including only an intervention IOL (Tecnis Eyhance) in comparison of other monofocal IOLs, [6] or even a particular monofocal model [7]. Conversely, this is the first scoping review covering a wide scope that explores not only the clinical results of enhanced monofocal IOLs in comparison to standard monofocal IOLs, but also in comparison to EDoF lenses and laboratory studies. In the absence of a standard definition for these new lenses and to avoid confusion with EDoF lenses, the aim of this scoping review was to summarize the clinical and laboratory outcomes provided by enhanced monofocal IOLs (Concept) and to determine which of the endpoints, described by the ANSI for EDoF lenses and some additional endpoints that might be included in future standards (Context), are fulfilled in patients undergoing cataract surgery (Population).
Review question
The following questions were addressed in this scoping review.
What are the optical quality and profiles described in laboratory studies of enhanced monofocal lenses?
What are the functional outcomes of patients implanted with enhanced monofocal IOLs for cataract surgery?
Which efficacy endpoints, described by the standard (ANSI) and additional ones, are fulfilled for enhanced monofocals?
Keywords
Enhanced monofocal, monofocal plus, mono-EDoF, EDoF, simultaneous vision.
Eligibility criteriaParticipants
This scoping review considered studies involving patients who underwent cataract surgery with bilateral implantation of an enhanced monofocal IOL in the capsular bag, and studies evaluating IOLs in the laboratory through the measurement of optical quality or optical profile. The following exclusion criteria were applied for the clinical studies: age < 19 years, comorbidities, history of corneal laser refractive surgery, postoperative complications as the main study purpose, eyes requiring toric IOL implantation or additional corneal incisions (astigmatism > 1.5 D), combining different targets (micro-monovision), or different IOL models (mix-and-match) between eyes.
Concept
The main purpose of the eligible clinical studies was to provide monocular and binocular postoperative clinical results considering the following outcomes: visual acuity at several distances, defocus curves, contrast sensitivity function, and patient-reported outcomes such as the percentage of patients achieving spectacle independence, satisfaction, positive photic phenomena perception, positive dysphotopsia, and recommendation or decision to undergo the same IOL implantation. Eligible laboratory studies reported the results of optical quality or surface profiles.
Context
At least one of the following IOLs was included in the study: Tecnis Eyhance (Johnson & Johnson), IsoPure (Physiol), Xact (Santen), Zoe (OphthalmoPro GmbH), RayOne EMV (Rayner), Lentis Quantum (Teleon Surgical), Evolux (Sifi), Vivinex Impress (Hoya), and Extend HP (Hanita Lenses).
Types of Sources
This scoping review considered original studies, either case series (CS) or randomized clinical trials (RCT), systematic reviews, meta-analyses, case reports, and comments. The sources of gray literature were excluded. No language restrictions were applied.
Methods
The scoping review was conducted in accordance with the JBI methodology for scoping reviews, [8] and following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [9]. This review was conducted in accordance with the a priori protocol registered in the Open Science Framework (https://osf.io/m7wcu). A stakeholder and experts in IOLs were consulted when preparing the study protocol and when discussing the scoping review results as recommended by the JBI Manual for Evidence Synthesis [10]. The following deviations occurred from the a priori protocol: inclusion of the Extend HP (Hanita Lenses) in the Context, the addition of new key references found through snowballing techniques for manuscript published from the search date to the data extraction date starting on 3th of November 2022, and a third independent reviewer was included to resolve discrepancies.
Search strategy
The search strategy and the initial and secondary searches were conducted by one of the reviewers using the 2Dsearch tool (UXLabs Limited) and checked for adequacy by a second reviewer. The search strategy aimed to locate only published studies. An initial limited search of MEDLINE (PubMed) and Google Scholar for the first 200 references was performed by using several keywords to identify relevant and irrelevant studies. A keyword search was performed to identify commonly used words in titles and abstracts, and the index terms assigned to these references were explored using PubReMiner (Jan Koster (AMC)). In the second stage, the scope of the search was optimized to maximize sensitivity such that all previously identified relevant references were retrieved, and the major possible number of irrelevant references was omitted. The text words contained in the titles and abstracts of the articles and the index terms used to describe the articles were used to develop a full search strategy for PubMed on October 2, 2022. The search strategy, including all the identified keywords and index terms, was adapted for EMBASE (Elsevier) and Web of Science (Isi Web of Knowledge). Specific year ranges were applied to retrieve studies on enhanced monofocal IOLs from 2020 to 2022. Language filtering was not applied. A detailed search strategy is presented in supplemental file A. New references published from the systematic search to the date of data extraction on November 3, 2022, were identified through snowballing search techniques, executing the search algorithm again, and looking for those published in the last month.
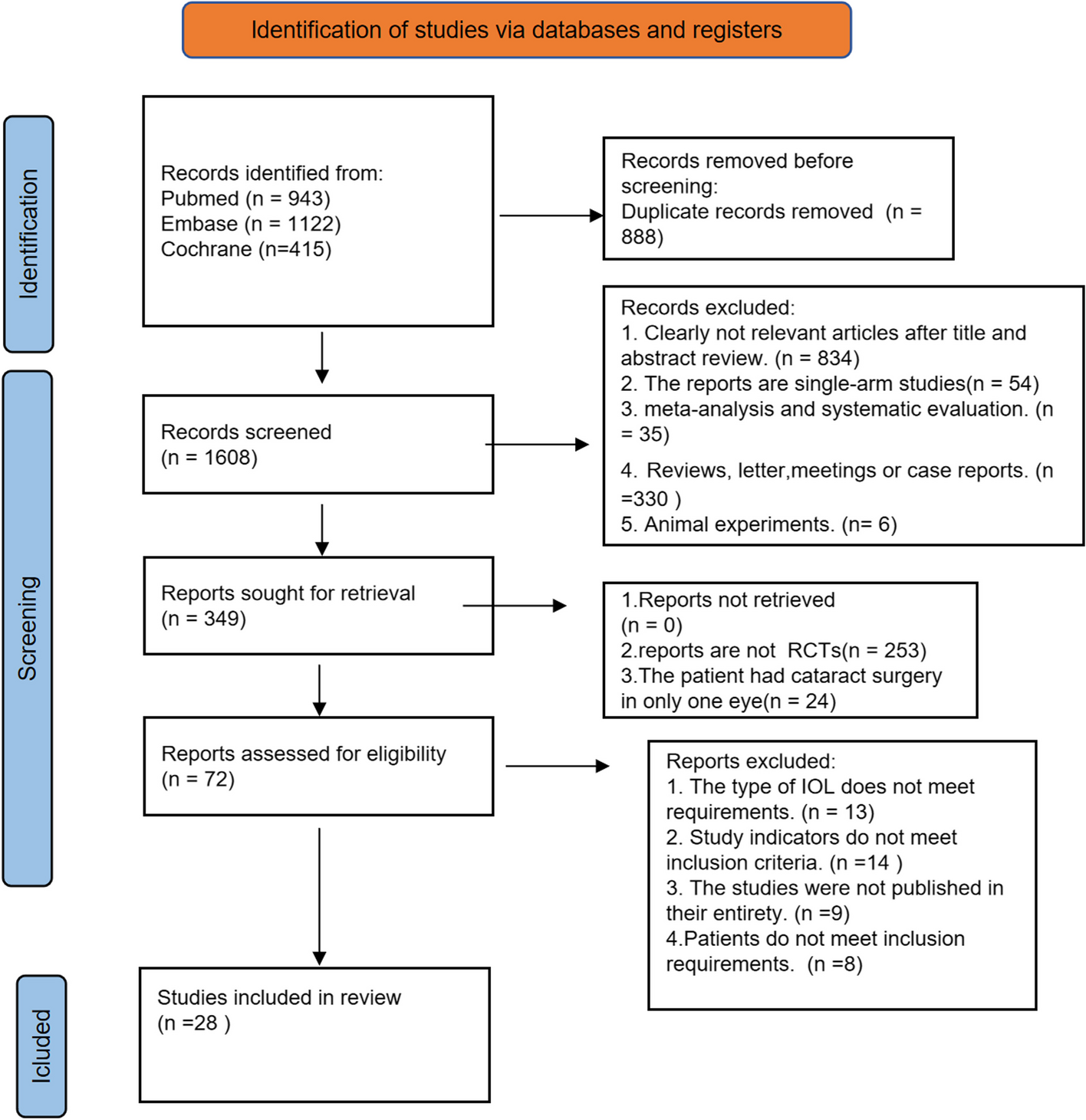
Study/source of evidence selection
Following the search, all identified citations were collated and uploaded to the Rayyan platform (Qatar Computing Research Institute, Doha, Qatar) for screening. Two independent reviewers screened titles and abstracts to assess the inclusion and exclusion criteria. The full text of the selected citations was assessed in detail against the inclusion criteria by the same two independent reviewers. The reasons for excluding sources of evidence at first and full-text screenings that did not meet the inclusion criteria were recorded and reported in this scoping review. Any disagreements between the reviewers at each stage of the selection process were resolved by a third independent reviewer.
Data extraction
Data were extracted from the papers included in the scoping review by two independent reviewers using a data extraction tool developed by the reviewers and described in the protocol. The extracted data included specific details about the participants, concept, context, study methods, and key findings relevant to the review questions. For studies that included plots for reporting results, as is habitual for defocus curves and contrast sensitivity, data were extracted from the images by one of the reviewers using the WebPlotDigitizer (Ankit Rohatgi) tool.
A new draft data extraction tool, not included in the protocol, was developed during the course of the review for laboratory studies because of the non-uniformity of the reported results for this concept. Any disagreements between the reviewers in data extraction were resolved by discussion. Missing data was filled as “Not Available” (NA), and no requests were made to authors for missing or additional data. Critical appraisal was not conducted, because it was not required for scoping reviews.
Data analysis and presentation
Tables and figures were used to present the data and illustrate the scoping review findings, as described in the protocol for clinical studies. A narrative summary describes how the results relate to the objectives and review questions. Different metrics were reported in the laboratory studies; therefore, the organization for presenting these data was decided during scoping review writing, instead of the protocol. The criteria for selecting the indices shown in the results section were the capability of the information to be summarized in single indices and the uniformity shown in the included manuscripts to describe common indices.
Patient and public involvement
There was no patient or public involvement in this scoping review.





留言 (0)