
記住我


Forty-five individuals with LGMD were identified for the study. Of those, 29 (64.4%) met eligibility criteria and 23 (51.1%) completed an interview. Of those who did not meet eligibility criteria (n = 16, 35.5%), the majority were excluded due to an unknown or ineligible subtype (n = 13, 28.9%). Participant characteristics are shown in Table 1. Participants were mostly ambulatory (n = 14, 60.9%), age 18 or older (n = 18, 78.3%), and diagnosed with LGMD subtype 2D/R3 (n = 12, 52.2%).
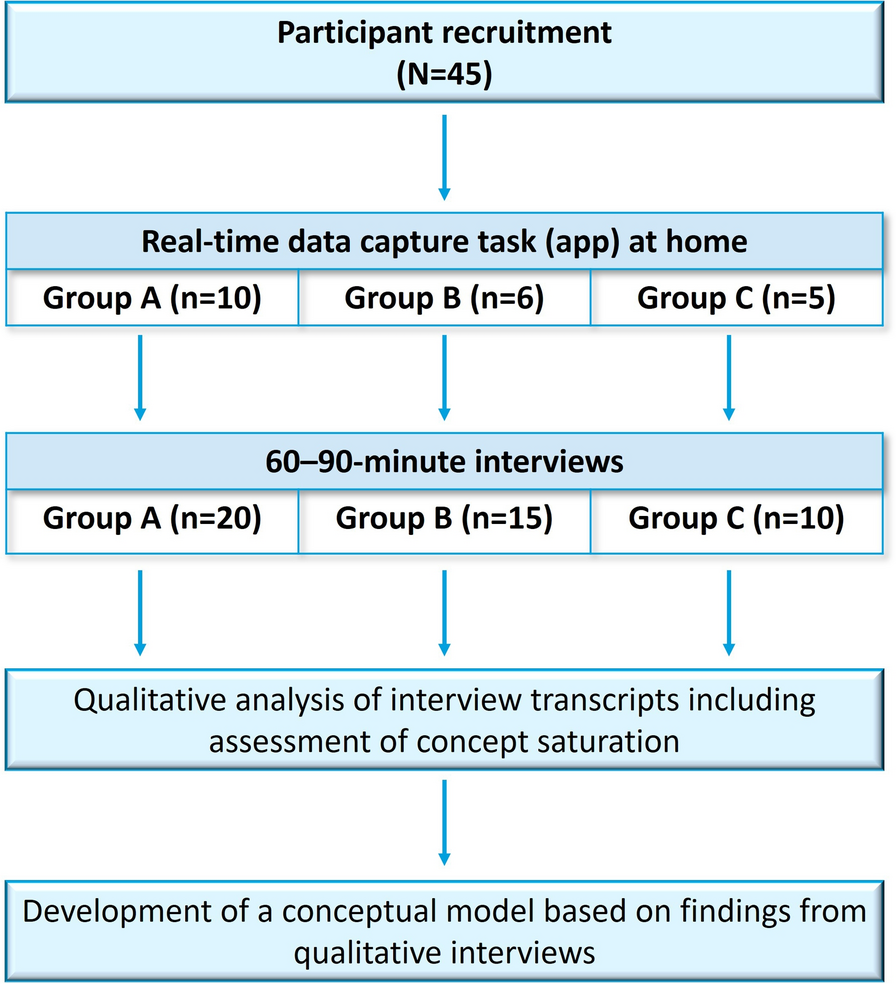
Table 1 Demographics and clinical characteristics of participants with LGMD (N = 23)Key Themes of LGMD Patient ExperienceDuring the interviews, participants identified a total of 40 symptoms and impacts (Table 2). Most symptoms and impacts (82.5%) reported appeared within the first group of 6 interviews. The remaining 17.5% appeared within the second and third interview groups of 6 interviews each (i.e., within the next 12 interviews). No new codes were identified in the final group of 5 interviews, demonstrating concept saturation.
Table 2 Symptoms and impacts of LGMD (N = 23)Key themes included mobility and function of the lower extremities (e.g., standing, walking, going up and down stairs) and upper extremities (e.g., reaching, bending, fine motor skills), ADLs (e.g., bathing, getting dressed, toileting), and physical transfers (e.g., getting in and out of bed, getting up off the floor, sitting down). There were no observed differences in symptoms reported by LGMD subtype. When asked to describe their “worst” or most bothersome symptoms, participants frequently discussed upper and lower extremity weakness (i.e., issues with physical strength; n = 7, 30.4%) and pain (n = 10, 43.5%). The LGMD patient experience differed based on ambulation status and is described below.
Ambulatory Participants with LGMDAmong ambulatory participants (n = 14), the most commonly reported issues were associated with physical strength (n = 14, 100%), lower extremity mobility (n = 13, 92.9%), and ability to transfer (n = 12, 85.7%). In terms of ADLs, difficulty getting dressed was the most frequently reported challenge (n = 8, 57.1%). Pain (n = 11, 78.6%), mood disturbance (n = 10, 71.4%), and fatigue (n = 9, 64.3%) were also reported by ambulatory participants with LGMD.
Similarly, the most bothersome symptoms reported by ambulatory participants were issues with physical strength, including weakness in the lower extremities (n = 7, 50.0%) and the upper extremities (n = 4, 28.6%). One participant mentioned that “[…] what bothers me the most is I’m not able to do… physical activity continuously, … [due to] weakness here in the shoulders and legs.” Difficulties with lower extremity mobility and function (e.g., running n = 4, 28.6%) and pain (n = 7, 50.0%) were also bothersome. Another participant described their pain as “some muscle discomfort and pain or nerve pain” and that “it feels like maybe a cramping, but it’s not really a cramp, and it feels more weak.”
Non-Ambulatory Participants with LGMDAll non-ambulatory participants (n = 9, 100.0%) reported issues with upper and lower extremity mobility and function and the ability to transfer. The majority also reported challenges with physical strength (n = 8, 88.9%). Challenges with ADLs were reported by all non-ambulatory participants (n = 9, 100.0%), including bathing and feeding self/preparation of meals (both n = 7, 77.8%). Social impacts were also reported by all non-ambulatory participants with LGMD (n = 9, 100.0%), including one participant who stated “…I can’t get out. I’m stuck here unless somebody drives me somewhere.” Yet another described their experience as impacting their “ability to go over to people’s houses” and “make friends” because “people look at you different, people treat you different.”
Likewise, the most bothersome symptoms included issues with upper and lower extremity mobility and function (both n = 3, 33.3%). One participant noted that “the most bothersome is not being able to stand or walk.” Issues with physical strength, specifically upper extremity weakness (n = 3, 33.3%), and pain and mood disturbance (both n = 3, 33.3%) were also reported as bothersome by non-ambulatory participants. Other health problems (e.g., gastrointestinal function and respiratory issues) (n = 4, 44.4%) were also discussed, as reflected by the following quote: “[B]reathing, eating… [I]t’s more difficult to eat, like chewing [and] things like that. Then I’d say my stomach problems. [I get] constipation and bloating…”.
Treatment Expectations and GoalsDuring this interview study, participants were asked to describe treatment expectations and desirable treatment benefits. All participants (n = 23, 100.0%) reported that a treatment that maintained their current functioning would be beneficial, including one participant who stated, “it’s better than having a progressive wasting.” Further, the majority (n = 20, 87.0%) reported that a treatment that slowed the worsening of their symptoms would be beneficial. In the words of one participant, “if it slows it, anything’s better than a free fall.”
Participants commonly reported that an increase in physical strength would signal a successful (n = 10, 43.5%) or moderately successful (n = 5, 21.7%) treatment. Slowing the progression of the disease was also a sign of a successful (n = 7, 30.4%) or moderately successful (n = 8, 34.8%) treatment. Treatments that increase lower extremity mobility (n = 6, 26.1%) were also considered meaningful.
When asked which symptoms they would like to improve first when considering a new potential treatment for LGMD, a clear difference emerged by ambulation status (Table 3). Ambulatory participants desired improvement in physical strength (n = 7, 50.0%) and fatigue (n = 5, 35.7%), while non-ambulatory participants were hopeful for improved upper extremity mobility and function (n = 4, 44.4%) and other health conditions (n = 3, 33.3%).
Table 3 Symptoms of LGMD that participants would like to improve first (N = 23)aConceptual Model for Symptoms and Impacts of LGMDPer FDA guidance, an initial conceptual framework can be hypothesized to support the measurement of the health-related quality of life concept(s) of interest in a given population (i.e., to determine what to measure) and should be supported by qualitative evidence [35]. For this study, a conceptual model was developed based on the concept elicitation interviews to provide a visual depiction of symptoms and impacts important to individuals with LGMD throughout disease progression (Fig. 1). The model includes ambulatory and non-ambulatory individuals with LGMD in order to display the salient symptoms as the disease progresses. Difficulty with physical strength is experienced throughout all phases of disease progression, whereas fatigue and difficulty with lower extremity mobility and function are important primarily in early stages of disease progression and loss of ambulation. The ability to transfer becomes important as ambulation wanes, and it continues to be important throughout the non-ambulatory phase. Upper extremity mobility and function become important in the non-ambulatory phase.
Fig. 1
Conceptual model of LGMD symptoms and impacts
留言 (0)