
記住我


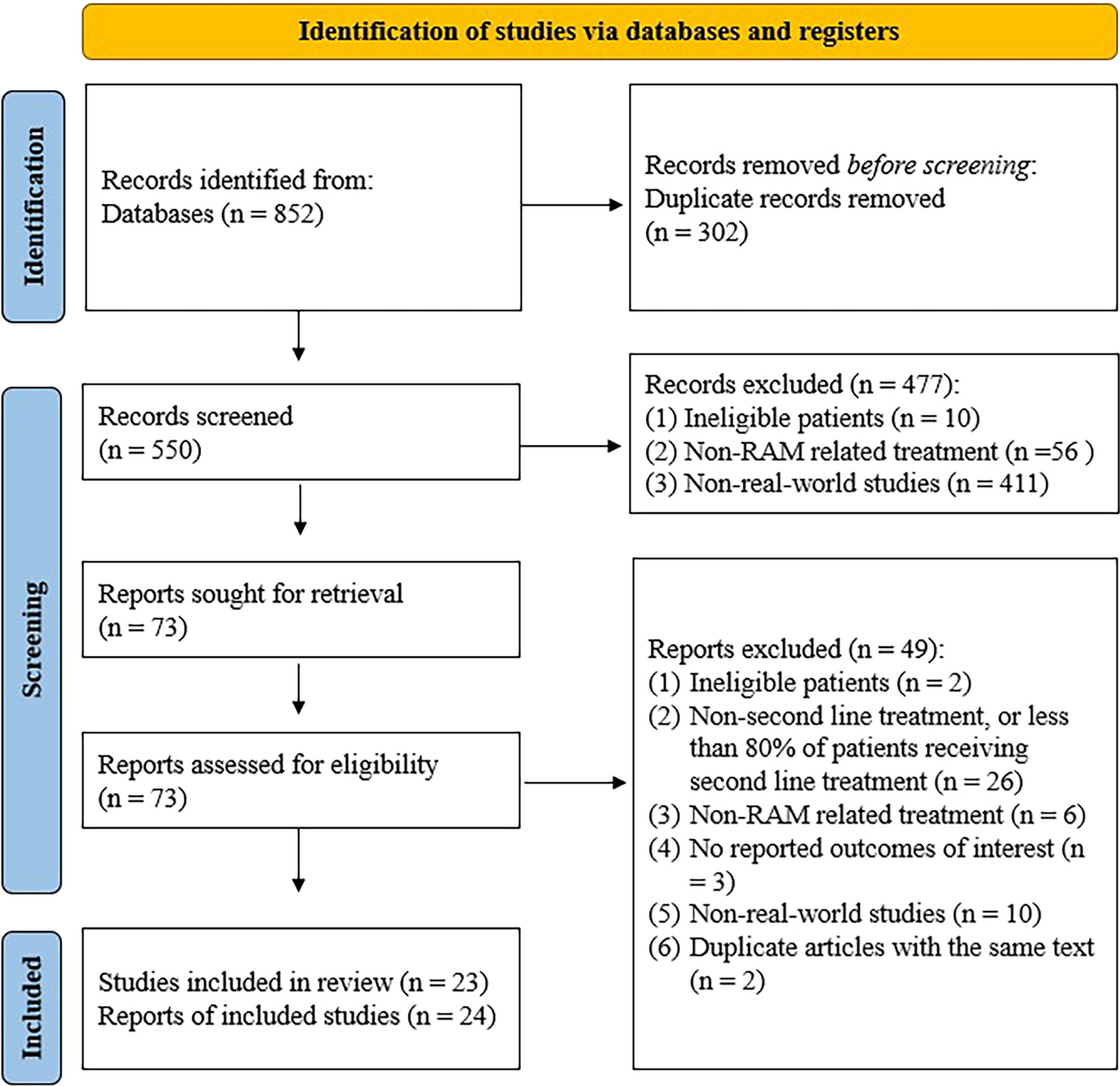
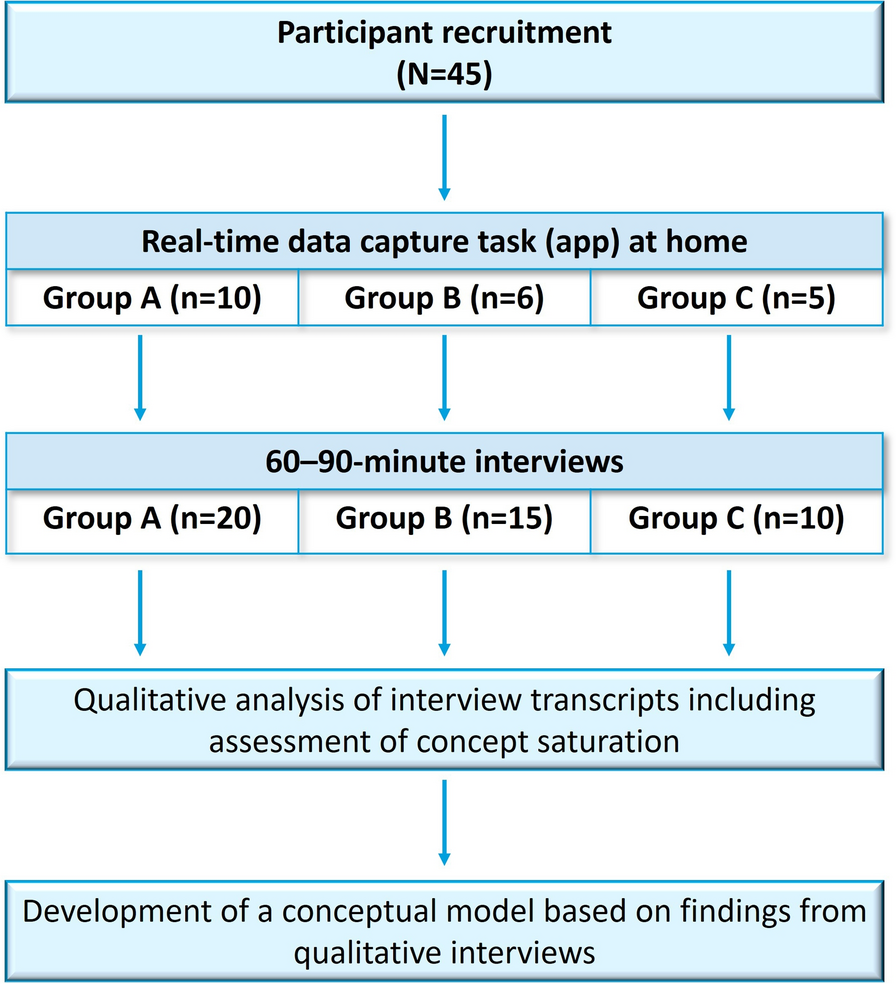
Of a total population of 549 patients with hypertension on combination therapy, 377 (68.7%) participants were on two-drug fixed-dose combinations at baseline, including 123 on CCB + DIU, 96 on RAASi + CCB, and 158 on RAASi + DIU (Fig. 1). Their mean age was 54.6 (± 11.3) years, similar across the different subgroups of SPCs. There were 187 (49.6%) male participants. Also, half of the participants reported a history of hypertension, and the median duration was 2.0 (IQR 1.0–7.0) years. The baseline SBP was 168.3 (± 12.5) mmHg and was slightly higher in participants on RAASi + CCB combinations compared to the other two subgroups. In addition, the baseline DBP was 99.2 (± 10.0) mmHg, with no significant differences between the different subgroups of SPCs. Table 1 summarizes the baseline characteristics of study participants by subgroup of SPCs used for treatment of hypertension.
Fig. 1
Flowchart of participant recruitment. CCB calcium channel blockers, DIU diuretics, RAASi renin–angiotensin system inhibitor, SPCs single pill combinations
Table 1 Baseline characteristics compared between three subgroups of patients treated with two-drug single pill combinationEffectiveness of Different Dual Therapy Combinations on Blood PressureThe distribution of active molecules in the different SPCs is shown in Fig. 2. Of the 283/377 (75.1%) patients taking an SPC containing a diuretic, 212/377 (56.2%) were taking indapamide and 71/377 (18.8%) were on hydrochlorothiazide. An SPC containing perindopril was prescribed in 59.8% of the 254 (67.4%) on RAASi, while amlodipine was prescribed in 95.9% of the 219 (58.1%) patients receiving an SPC with CCB.
Fig. 2
Proportion of use of medications in the different drug classes
A decrease of 34.3 (± 14.2) mmHg units of SBP was observed at week 16, with no significant difference between the three groups of SPCs (p = 0.118). There was a slightly higher decrease in SBP in participants on SPCs containing a CCB compared to participants on SPCs comprising RAASi + DIU . However, this was not statistically significant across the different time periods of follow-up (Table 4).
A mixed linear model adjusted for age, gender, and baseline SBP revealed that the different follow-up period had a significant main effect on the change in SBP from baseline to 16 weeks, F3,1122 = 36.03, p < 0.001, but there was no significant main effect on the type of SPC and SBP change. Similarly, no significant interaction effect was observed between the follow-up period and the type of SPC. From week 4 to week 16, there was a linear trend in SBP change, with a mean change at 4 weeks and 16 weeks of 28.7 (16.6) mmHg and 34.3 (14.2) mmHg, respectively. A post hoc analysis of the various follow-up periods revealed a significant difference in SBP change between weeks 4 and 16, p < 0.01.
Further analysis of the BP changes from baseline across the different time points revealed no significant interaction effect between follow-up time and type of SPC on SBP (Fig. 3).
Fig. 3
Systolic blood pressure change from baseline through week 16. CCB calcium channel blockers, DIU diuretics, RAASi renin–angiotensin system inhibitor, PWC pairwise comparisons. CCB calcium channel blockers, RAASi renin–angiotensin system inhibitor
There was no significant interaction effect between follow-up time and the group of SPCs on SBP F5.5,1028.3 = 1.55, p = 0.16. Likewise, the main effect of the type of SPC on BP control was not statistically significant F2,374 = 3.1, p = 0.05 (Fig. 4). However, there was a significant main effect of the period of follow-up on SBP F2.75,1028.3 = 943.3, p < 0.001. Pairwise post hoc comparisons for follow-up time and SBP were statistically significant across the different follow-up periods.
Fig. 4
Systolic blood pressure during 16 weeks of follow-up. CCB calcium channel blockers, DIU diuretics, RAASi renin–angiotensin system inhibitor
Furthermore, no significant interaction effect was observed for the SPC type and follow-up time on DBP change F5.7,1073.9 = 0.7, p = 0.6 Similarly, there was no significant main effect of the class of SPC on BP, F2,374 = 1.0, p = 0.3 (Fig. 5). There was a significant main effect of follow-up time on the DBP, F2.9,1073.1 = 594.4, p < 0.001.
Fig. 5
Diastolic blood pressure during 16 weeks of follow-up. CCB calcium channel blockers, DIU diuretics, RAASi renin–angiotensin system inhibitor
Rate of BP ControlTwo-thirds of patients had their BP controlled at 16 weeks of treatment, with a slightly higher percentage in the participants on combination with CCB (Table 2). Logistic regression models were fitted to estimate the effect of SPCs on blood pressure control at week 8, while controlling for baseline SBP, gender, and age. With the RAASi + DIU group used as the reference group, the odds ratio of BP control at week 8 was 1.40 (95% CI 0.85, 2.33) and 0.79 (95% CI 0.46, 1.36) for the CCB + DIU and RAASi + CCB groups, respectively. Similarly, the odds ratio for BP control at week 16 were 1.27 (95% CI 0.75, 2.17) and 0.83 (95% CI 0.48, 1.45).
Table 2 Control rate of the office blood pressure across different follow-up periods for the three subgroups of patients treated with two-drug single pill combinationAdverse EventsRates of adverse events (Table 3) were not statistically significant among the three listed groups. The overall incidence of adverse events was 3.4%, and fatigue was the most frequently reported. Unproductive cough was reported by three participants.
Table 3 Side effects of the three subgroups of patients treated with two-drug single pill combination
留言 (0)