
記住我
Chronic hepatitis B (CHB) is a major public health problem in the United States,1 which has an estimated 840,000 to 2.4 million people living with CHB and at risk for premature death from cirrhosis and hepatocellular carcinoma (HCC).1–6 In 2018, there were 1649 hepatitis B virus (HBV)-related deaths reported, although the true number could be 5 times higher.7 CHB disproportionately affects Asian and Black Americans; Asian people are 9 times and Black people 2.5 times more likely to die from hepatitis B-related complications than non-Hispanic White Americans.8 Most of the deaths can be prevented with disease monitoring and antiviral therapy to prevent and reverse liver inflammation, fibrosis, and cirrhosis, and liver imaging for hepatocellular carcinoma (HCC) surveillance for early detection and treatment. The World Health Organization's global hepatitis elimination strategy, endorsed by the US Government, aims to reduce new HBV infections by 90%, reduce deaths from viral hepatitis by 65%, diagnose 90% of persons living with CHB, and treat 80% of treatment-eligible patients to reduce HBV-related mortality by 2030.9
The American Association for the Study of Liver Diseases (AASLD) recommends patients diagnosed with CHB should receive regular monitoring for liver inflammation and viral activity. The initial tests recommended after CHB diagnosis should include blood tests for ALT, HBV DNA, and HBeAg.10 Patients who experience increased risk for HCC, including patients with cirrhosis or a first-degree relative with a history of HCC, Asian and Black men older than 40 years, Asian women older than 50 years, and patients with hepatitis D co-infection, are recommended to undergo HCC surveillance with liver ultrasound every 6 months. Antiviral therapy is recommended for any patient with cirrhosis regardless of ALT and HBV DNA levels and patients without cirrhosis who have active hepatitis and elevated HBV DNA.10
Several studies suggested patients with CHB in the United States received inadequate monitoring and treatment. Cohen speculated that CHB was undertreated in the United States based on Gilead Sciences estimates that ~50,000 of an estimated 1.4 to 2 million persons living with CHB in 2010 were prescribed HBV antiviral medications.11 Wong reported that only 37.3% of treatment-eligible patients received antiviral therapy between 2010 and 2015 in 4 urban safety-net health systems.12 Spradling reported only 37% of 2338 patients enrolled in the Chronic Hepatitis Cohort Study during an 8-year follow-up period from 2006 to 2013 had≥one HBV DNA test annually, only 14% with cirrhosis had≥1 annual liver imaging study and only 56% with cirrhosis were prescribed antiviral therapy.13Two studies examined CHB treatment using the MarketScan Commercial Claims and Encounters Database. Ogawa reported between 2007 and 2014, only 34.8% of CHB patients with cirrhosis received antiviral treatment.14 Harris reported between 2008 and 2016, only 34% of CHB patients received ALT and either HBV DNA or HBeAg tests more than 12 months after CHB diagnosis, and 26.4% with cirrhosis and 17.5% without cirrhosis received antiviral treatment.15 Harris’s study included patients with HIV, HCV, HCC, and liver transplants and likely underestimated the proportion of patients who received ALT tests because the comprehensive metabolic panel with ALT was not included in the analysis.
Prior studies have not examined what proportion of patients with new CHB diagnoses received timely monitoring, HCC surveillance, and treatment. The goal of this study was to evaluate the rates of monitoring, HCC surveillance and antiviral treatment within 12 months of initial CHB diagnosis in adults with HBV mono-infection and without HCC or liver transplant, and the factors, including race associated with these outcomes to identify gaps and disparities to guide the development of recommendations to improve CHB management in the United States.
METHODSData used in this study were obtained from deidentified patients’ demographics, enrollment, medical diagnosis, and insurance claims in the Optum Clinformatics Data Mart (Optum 4.0) database at Stanford Center for Population Health Sciences that included privately insured patients and Medicare Advantage enrollees. According to Optum, in 2014, ~19% of the US population in commercial health plans and 19% of those in Medicare Advantage plans were represented in Optum’s administrative data assets.16 Each person was assigned a unique identification number which allowed linkage between the data tables. Enrollees aged older than 18 years who were in the Optum database between January 1, 2016 and December 31, 2019 were included. To eliminate the potential impact of the COVID-19 pandemic on CHB disease monitoring and treatment within 12 months of diagnosis, patients with new CHB diagnoses after December 31, 2018 were excluded. Patients with CHB were defined as unique persons with≥1 ICD-9 or ICD-10 diagnosis code for CHB (Appendix Table 1, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). In this study of HBV mono-infected patients, patients with HIV, HCV, HCC, or liver transplant were excluded, as they are likely to have different rates of treatment and monitoring than mono-infected patients. Patients with newly diagnosed CHB were defined as patients with no CHB diagnosis code documented before January 1, 2016. To assess the monitoring and treatment of patients with a new CHB diagnosis within 12 months of initial diagnosis, the 5978 patients with newly diagnosed CHB who were continuously enrolled≥6 months before and≥12 months after their CHB diagnosis were included (Fig. 1).
 FIGURE 1:
FIGURE 1: Monitoring and treatment of 5978 patients with new CHB diagnosis between January 1, 2016 and December 31, 2018 (n=5978). CHB indicates chronic hepatitis B; HBeAg, hepatitis B e-antigen; HCC, hepatocellular carcinoma.
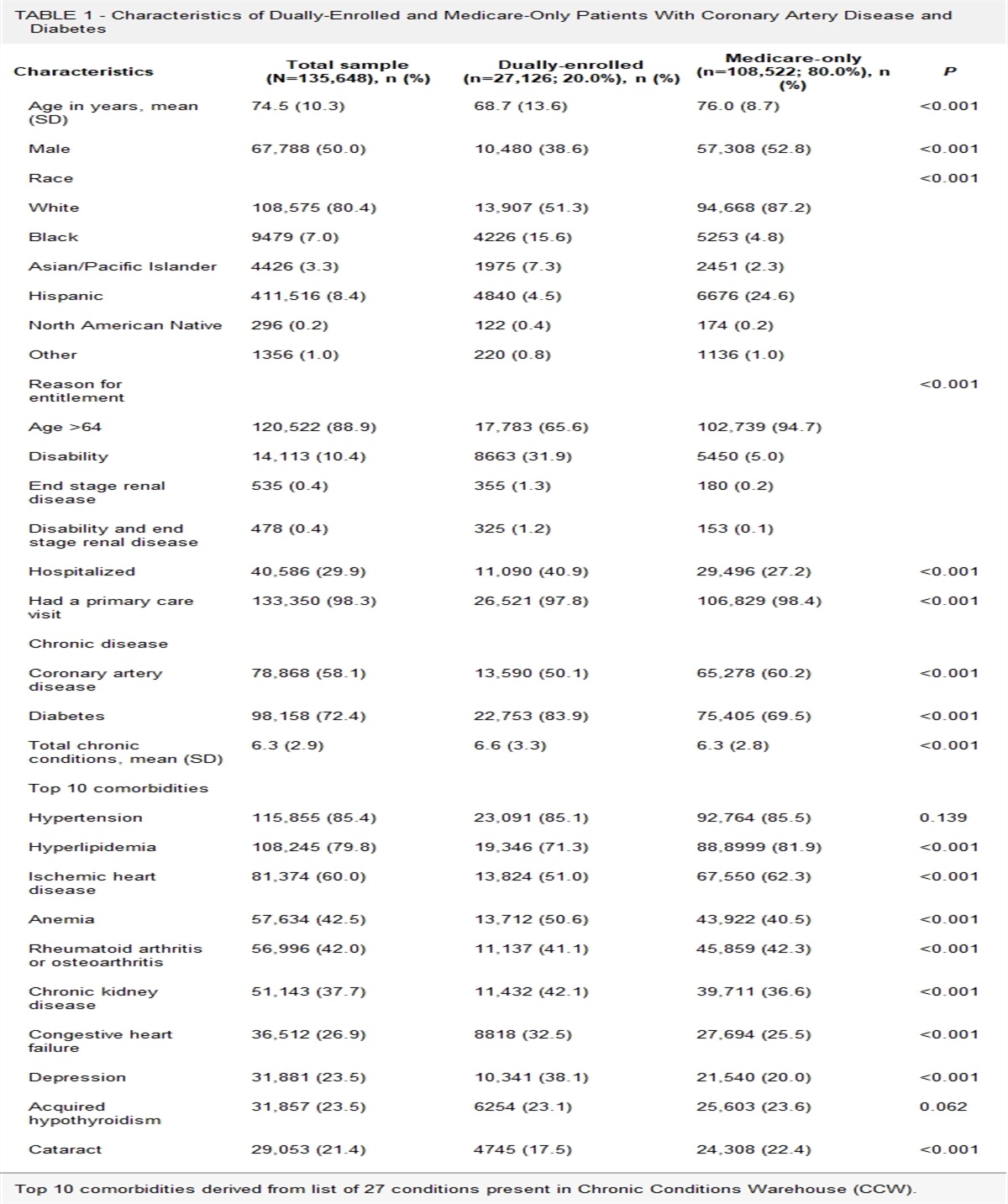
Demographic information for patients with new CHB diagnosis included sex, race, health insurance type, and ages 18 to 44 years, 45 to 64 years, and≥65 years (using the Centers for Disease Control and Prevention cancer prevention definition of midlife adults as 45 to 64 y old) (Table 1). Clinical information consisted of the presence or absence of a cirrhosis diagnosis.
TABLE 1 - Demographics and Clinical Characteristics of Patients With New CHB Diagnosis (Without HIV or HCV Co-infection or Liver Transplant or HCC) Between 1/1/2016 and 12/31/2018 in Continuous Enrollment at Least 6 Months Before and 12 Months After CHB Diagnosis (n=5,978) Categories N (%) Age group in years* (median 58, range 18–88) 18–44 1430 (23.9) 45–64 2078 (34.8) ≥65 2470 (41.3) Sex Male 2923 (48.9) Female 3054 (51.1) Unknown 1 Race Asian 2674 (44.8) White 1885 (31.5) Black 682 (11.4) Hispanic 557 (9.3) Unknown 180 (3.0) Cirrhosis No 5582 (93.4) Yes 396 (6.6) Insurance Commercial 3319 (55.5) Medicare 2433 (40.7) Both 226 (3.8)CHB indicates chronic hepatitis B; HCC, hepatocellular carcinoma.
Disease monitoring was based on unique patients with CHB and≥1 current procedural terminology code for laboratory tests (ALT and either HBV DNA or HBeAg) and imaging (liver and abdominal ultrasound, computed tomography, magnetic resonance imaging) within 12 months of CHB diagnosis (Appendix Table 2, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). Patients with CHB who received HBV antiviral therapy were defined as unique patients who had prescription claims for≥1 brand name or generic HBV antiviral medications within 12 months of CHB diagnosis (Appendix Table 3, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). Disease monitoring and treatment outcomes were also stratified by cirrhosis status. This secondary analysis of deidentified insurance claims data was approved under the Stanford University Center for Population Health Sciences umbrella IRB 40974.
Data AnalysisThe STATA 12.0 statistical software was used for data analysis. We performed descriptive statistical analysis to describe the demographic and clinical characteristics of the study population as well as to calculate the key outcome measurements (disease monitoring and treatment rates). Univariable and multivariable logistic regression models were used to evaluate the demographic and clinical characteristics (cirrhosis) of patients with CHB associated with whether the patient received≥1 claim for disease evaluation with ALT and either HBV DNA or HBeAg tests,≥1 claim for liver imaging tests, and≥1 prescription claim for HBV antiviral therapy within 12 months of the CHB diagnosis. Among patients who had prescription claims for HBV antiviral therapy within 12 months of diagnosis and in continuous enrollment≥24 months of diagnosis, we also assessed the demographic and clinical characteristics associated with the likelihood of continuing to have prescription claims at 13–24 months. Variables with P value <0.25 in univariable analysis were included in multivariable analysis. Adjusted odds ratios and their 95% confidence intervals were used to provide further insight regarding the relative importance of each independent variable on the outcome variable. Statistical significance was assessed based on a P value≤0.05.
RESULTS Demographics of Patients With New CHB DiagnosisThere were 22,250,941 adult enrollees in the Optum database between January 1, 2016 and December 31, 2018 (66.3% were White, 14.2% were Hispanic, 11.2% were Black, and 5.6% were Asian). Among the cohort of 5978 patients with new CHB diagnoses who were continuously enrolled≥6 months before and≥12 months after their initial diagnosis, 48.9% were male (Table 1). The median age was 58 years (range 18 to 88 y), and 76% were≥45 years old. Although Asian people represented only 5.6% of enrollees in the Optum database between 2016 and 2018, 44.7% of the patients with new CHB diagnoses were Asian, 31.5% were White, 11.4% were Black, and 9.3% were Hispanic. 6.6% of CHB patients had cirrhosis, 0.8% had hepatitis D, 55.5% were covered by commercial insurance, 40.7% by Medicare Advantage plans, and 3.8% by both (Table 1).
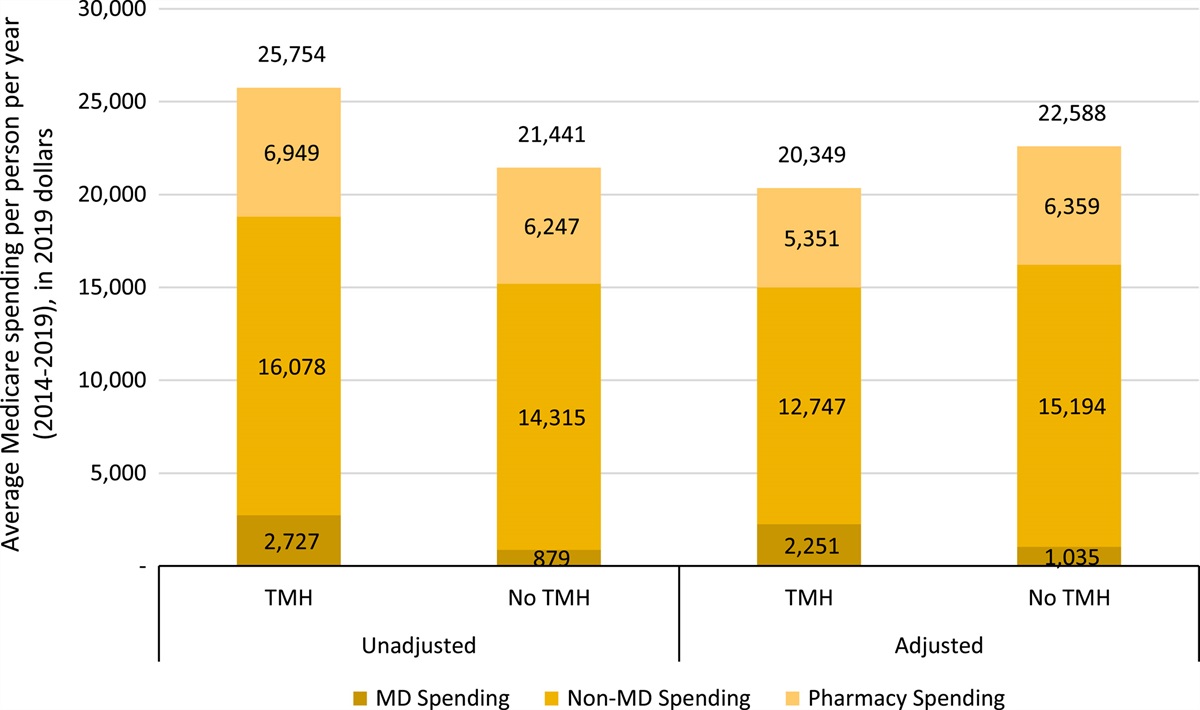
Monitoring for Liver Inflammation and Viral ActivityAmong the 5978 patients with a new CHB diagnosis, patients with cirrhosis were significantly more likely than patients without cirrhosis to receive≥one ALT and either HBV DNA or HBeAg tests within 12 months of diagnosis [CI 1.7(1.4 to 2.1), P<0.01] (Table 2). Among patients with cirrhosis, 94.4% had claims for≥1 ALT, 54%≥one HBV DNA, and 37.1%≥1 HBeAg test, but only 56.3% had≥1 ALT and either HBV DNA or HBeAg tests (Fig. 1). Among persons without cirrhosis, 83.8% had claims for≥1 ALT, 52.4%≥1 HBV DNA, and 30.1%≥1 HBeAg tests, but only 49.9% had≥1 ALT and either HBV DNA or HBeAg tests (Fig. 1). Multivariable analyses showed that patients who were significantly more likely to receive ALT and either HBV DNA or HBeAg tests within 12 months of CHB diagnosis were under 45 years old (P<0.01), male (P=0.02), Asian (P<0.01), privately insured (P<0.01), or had cirrhosis (P<0.01) (Table 2).
TABLE 2 - Univariable and Multivariable Analysis of Demographic and Clinical Factors Associated With Receiving Testing for ALT and HBV DNA or HBeAg and With Receiving HBV Antiviral Treatment Within 12 Months After Diagnosis Among Patients With New CHB Diagnosis Between January 1, 2016, and December 31, 2018 (n=5,978) ALT and HBV DNA or HBeAg testing HBV antiviral treatment N (%) Univariable analysis Multivariable analysis N (%) Univariable analysis Multivariable analysis Characteristics Categories Odds ratio, (95% CI) P Adjusted odds ratio, (95% CI) P Odds ratio, (95% CI) P Adjusted odds ratio, (95% CI) P Age 18–44 888 (62.1) (Ref) — (Ref) — 173 (12.1) (Ref) — — — 45–64 1090 (52.5) 0.67 (0.59–0.77) <0.01 0.72 (0.62–0.84) <0.01 282 (13.6) 1.14 (0.93–1.39) 0.20 — — ≥65 1028 (41.6) 0.44 (0.38–0.50) <0.01 0.64 (0.51–0.81) <0.01 254 (10.3) 0.83 (0.68–1.02) 0.08 — — Sex Male 1530 (52.3) — — (Ref) — 419 (14.3) (Ref) — (Ref) — Female 1475 (48.3) 0.85 (0.77–0.94) <0.01 0.87 (0.78–0.97) 0.02 289 (9.5) 0.62 (0.53–0.73) <0.01 0.66 (0.62–0.77) <0.01 Race Asian 1643 (61.4) (Ref) — (Ref) — 370 (13.8) (Ref) — (Ref) — White 737 (39.1) 0.40 (0.36–0.45) <0.01 0.43 (0.38–0.49) <0.01 205 (10.9) 0.76 (0.63–0.91) <0.01 0.74 (0.62–0.89) <0.01 Black 339 (49.7) 0.62 (0.52–0.73) <0.01 0.63 (0.53–0.75) <0.01 73 (10.7) 0.74 (0.57–0.97) 0.03 0.70 (0.54–0.93) 0.01 Hispanic 207 (37.2) 0.37 (0.31–0.45) <0.01 0.40 (0.33–0.49) <0.01 36 (6.5) 0.43 (0.30–0.61) <0.01 0.41 (0.28–0.58) <0.01 Insurance types Commercial 1917 (57.8) (Ref) — (Ref) — 438 (13.2) (Ref) — (Ref) — Medicare 1012 (41.6) 0.52 (0.47–0.58) <0.01 0.71 (0.58–0.87) <0.01 254 (10.4) 0.77 (0.65–0.90) <0.01 0.74 (0.62–0.89) <0.01 Both 77 (34.1) 0.38 (0.29–0.51) <0.01 0.57 (0.40–0.79) <0.01 17 (7.5) 0.53 (0.32–0.88) 0.01 0.53 (0.329–0.88) 0.02 Cirrhosis No 2783 (49.9) (Ref) — (Ref) — 595 (10.7) (Ref) — (Ref) — Yes 223 (56.3) 1.28 (1.04–1.57) 0.02 1.7 (1.4–2.1) <0.01 114 (28.8) 3.39 (2.68–4.28) <0.01 3.88 (3.03–4.97) <0.01The most common prescribed HBV antiviral therapy were:
Tenofovir: 399 (56.3%); Entecavir: 292 (41.2%); Lamivudine: 38 (5.4%); Combination tenofovir-emtricitabine medicines 26 (3.7%); Adefovir 1 (0.1%).
No patient was prescribed interferon or telbivudine.
CHB indicates chronic hepatitis B; HBeAg, hepatitis B e-antigen.
Among patients with cirrhosis, 82.1% (84.9% of men and 78.3% of women) had claims for≥1 liver imaging study with either ultrasound, computed tomography, or magnetic resonance imaging within 12 months of CHB diagnosis (Fig. 1). However, only about half of the patients without cirrhosis recommended for HCC surveillance (58% of Asian men and 51.2% of Black men age>40 years, and 58% of Asian women>50 years) had received≥1 liver imaging test within 12 months of initial diagnosis (Appendix Tables 5 and 6, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). Ultrasound accounted for 79% of the liver imaging studies performed in patients with and without cirrhosis. Among patients with cirrhosis, age, sex, race, or insurance type did not affect the likelihood of receiving liver imaging (Appendix Table 4, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). However, among men older than 50 years old without cirrhosis recommended for HCC surveillance, Asian men were more likely than Black men (P=0.05) to receive≥1 liver imaging study within 12 months of diagnosis. Insurance type did not affect the likelihood of non-cirrhotic patients receiving liver imaging tests (Appendix Tables 5 and 6, Supplemental Digital Content 1, https://links.lww.com/MLR/C600).
HBV Antiviral TherapyIn all, 28.8% of patients with cirrhosis (114 out of 396) and 10.7% of patients without cirrhosis (595 out of 5,582) had≥1 prescription claims for HBV antiviral therapy within 12 months of diagnosis (Fig. 1).
Univariable and multivariable analysis showed that patients who were male, Asian, with commercial insurance, or had cirrhosis were more likely (P<0.05) to have≥1 prescription claim for HBV antiviral treatment (Table 2). There was no significant difference in the likelihood of receiving treatment between patients ages 18 to 44 years, 45 to 64 years, and≥65 years. Among patients with cirrhosis, 37.7% of Asian patients, 27% of White patients, 33.9% of Black patients, and 11.1% of Hispanic patients received antiviral therapy within 12 months of diagnosis (Appendix Table 7, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). The HBV antiviral therapies prescribed were tenofovir (56.3%), entecavir (41.2%), lamivudine (5.4%), tenofovir-emtricitabine (3.7%), and adefovir (0.1%). No patient was prescribed interferon or telbivudine.
Among patients who received antiviral treatment within 12 monthsof diagnosis and were continuously enrolled≥24 months after initial CHB diagnosis, 79.3% of patients with cirrhosis and 76.5% of patients without cirrhosis continued to have claims for HBV antiviral therapy at 13 to 24 months (Appendix Table 8, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). Asian patients were more likely to continue to have claims for antiviral therapy at 13 to 24 months compared with White and Black patients (81.6% vs. 72.7% and 69.8%, respectively), and patients ages 45 to 65 years compared with 18 to 44 years (80.7% vs. 69.6%).
DISCUSSIONIn this study to evaluate whether patients received timely evaluation and treatment following CHB diagnosis, only about half of the patients within 12 months following the diagnosis of CHB received≥one ALT and either HBV DNA or HBeAg tests, and only half of the non-cirrhotic patients eligible for HCC surveillance received liver imaging. Among cirrhotic patients, 82.1% received liver imaging, but only 28.8% received antiviral treatment. The low treatment rates in patients with cirrhosis are consistent with prior reports by Ogawa and Harris and suggest a continued lack of awareness and compliance with the AASLD treatment guidelines.14,15
The current study found that Asian patients were more likely to receive ALT and either HBV DNA and HBeAg tests, and Asian persons without cirrhosis were more likely to receive liver imaging for HCC surveillance within 12 months of CHB diagnosis. Asian patients were also more likely to receive antiviral treatment and continue to have claims for antiviral therapy at 13–24 months compared with White and Black patients. The higher treatment rates in Asian persons are consistent with the study by Wong, who reported that Asian patients compared with all other racial/ethnic groups have higher CHB treatment rates.12
The higher rates of disease monitoring and treatment among Asian patients are likely related to increased awareness attributed to the multifaceted outreach initiatives in some Asian communities about the high CHB prevalence and risk of death from untreated disease. They include the Jade Ribbon campaign started by the Asian Liver Center at Stanford University in 2000 and San Francisco Hep B Free, founded in 2007 to increase public and primary care providers’ awareness about the importance of hepatitis B testing and vaccination among Asian adults, the importance of regular long-term monitoring including HCC surveillance and adherence to treatment, and to ensure CHB patients have treatment access.17,18 Support is needed and encouraged to expand these outreach initiatives beyond East Asian communities to inform other populations, including US-born and non–US-born Black persons and Southeast Asian ethnic groups who experience risk for CHB.
It is unclear why patients with commercial insurance were more likely to receive testing for ALT and HBV DNA or HBeAg compared with persons with Medicare Advantage plans, and yet insurance type did not affect the rates of HCC surveillance with the more costly imaging tests (Appendix 4 and 5, Supplemental Digital Content 1, https://links.lww.com/MLR/C600). Both the current study and the report by Wong12 found higher treatment rates in patients with commercial insurance compared with Medicare. The differences in treatment rates may be related to higher out-of-pocket treatment drug costs for some Medicare patients. In 2018, HBV antiviral drugs were listed as tier 5 drugs associated with high out-of-pocket costs in the Medicare Advantage formulary. Since then, costs of antiviral have dropped from thousands of dollars per year to below $500 per year for generic tenofovir and entecavir in 2022,19 but in many Medicare drug plans, generic entecavir and tenofovir are still listed as tier 4 drugs.20
Insufficient CHB disease monitoring and treatment could be the result of patient and healthcare provider-related barriers. In a systematic review of barriers to disease monitoring and HCC surveillance among patients with CHB in the United States, Ispas et al21 reported that 1 of the most common patient-related barriers is lack of patient’s knowledge about CHB, including the associated risks for liver cancer and liver cirrhosis, not knowing there are effective treatment available, and that there is currently no curative treatment. Other patient-related barriers that were identified included the patient’s beliefs, preference for complementary treatment, culture, and language, which made it difficult for the non-English–language proficient patients to understand the healthcare providers.21 To improve patients’ disease knowledge and adherence to regular monitoring tests and antiviral therapy, even if they do not experience any symptoms, providers should provide their CHB patients with language-concordant information in-person and evidence-based and culturally and linguistically appropriate pamphlets about hepatitis B facts and management that can be downloaded from various reputable websites.22,23 Wong and Khalili24 reported an in-person 20 minutes language-concordant educational session in the clinic resulted in a significant improvement in the patients’ HBV knowledge and compliance with clinic follow-up, laboratory monitoring, and treatment. Financial difficulties, including lack of insurance and out-of-pocket costs, have also been identified as a barrier to CHB monitoring and treatment.21 Out-of-pocket drug costs and not understanding the importance of long-term treatment are likely important reasons for the drop in treatment adherence of 20 % to 23.5% after the first year in the current study.
The most frequently identified healthcare provider-related barriers in a systematic review were a lack of knowledge about the disease and the benefits of antiviral treatment and HCC surveillance, as well as a lack of knowledge about or adherence to the AASLD guidelines on disease monitoring and treatment.21 In a survey of 219 physicians and residents in training, 80% of the respondents indicated that they did not feel they were well prepared by their medical training to care for patients with CHB.25 In another study of 277 primary care providers affiliated with several major health systems located in a high CHB prevalence city, authors found nearly half of the providers were unfamiliar with current AASLD guidelines for CHB management and a third of the providers were unaware that antiviral therapy would reduce the risk of liver disease progression.26 Integrating hepatitis B screening and CHB treatment in primary care is important if we are to reach the 2030 elimination targets of diagnosing 90% of people living with CHB and treating 80% of eligible patients to reduce deaths from HBV-related complications. A number of resources have been developed recently to help educate and provide primary care providers with clear and easy-to-follow guidance for CHB screening, interpretation of the test results and CHB management, including when and how to treat CHB. These include 2 free mobile and online apps (Know HBV and Hep B Consult), simplified print algorithms on CHB diagnosis and treatment, and regional ECHO programs with hepatitis B case discussions and didactic lectures.27–32
A new law in California aims to incorporate chronic hepatitis screening, monitoring, and treatment as a standard of care by primary care providers. Starting from January 1, 2022, all facilities and clinics in California that provide primary care services are required to offer their adult patients a voluntary hepatitis B and hepatitis C screening test according to the latest United States Preventive Services Task Force screening recommendations. For patients who tested positive for chronic viral hepatitis, the law requires healthcare professionals to provide care and treatment or refer them for care and treatment according to the AASLD clinical practice guidelines.33 As electronic health records (EHR) are increasingly used to improve disease screening and immunization in primary care clinics, clinical decision support tools can be built into EHRs for hepatitis screening, reflex testing for patients with CHB that includes ALT, HBV DNA, and HBeAg, and HCC surveillance to further assist and improve care and treatment of CHB by primary care providers.34,35
There are several limitations to our study. The Optum database represents a sample of the US population covered by commercial insurance and a portion of Medicare patients enrolled in Medicare Advantage programs. Optum does not have data on patients who are uninsured, incarcerated, or covered by Medicaid or Veterans Administration and may not be representative of the status of CHB monitoring and treatment across the country. Another limitation is claims data are primarily collected for billing purposes and only have encounters that occurred during the patient’s enrollment in the health plan and do not provide information about their diagnosis and services before they joined the health plans. It may be possible that some enrollees identified with new CHB diagnoses in Optum between 2016 and 2018 were diagnosed with CHB before they were entered into the Optum database, and some were disenrolled within 12 months of diagnosis and were not included in the monitoring and treatment analyses. Claims data do not provide information about how the diagnosis of cirrhosis was determined and what fraction of the patients without cirrhosis who did not have claims for HBV antiviral therapy were treatment-eligible by AASLD guidelines. We cannot determine if patients without claims for testing and treatment were the result of non-adherence or because the provider did not order the tests or prescribe the HBV antiviral medication for treatment-eligible patients. The low proportion of Black and Hispanic patients in the study may also not be representative of the status of monitoring and treatment of Black and Hispanic patients with CHB in the country.
Our findings add to the increasing body of evidence that even among patients diagnosed with CHB, many are not receiving the clinical assessments and treatment recommended. To reach the global and the US goals to eliminate hepatitis B as a public health threat by 2030, a comprehensive national HBV elimination strategy is urgently needed, including initiatives to address patient and provider-related barriers to improve CHB prevention, screening, care, and treatment. Initiatives could include adding hepatitis B screening and linkage to monitoring and treatment in EHRs; providing patients with culturally and linguistically appropriate information about CHB risks, monitoring, and treatment; and reclassifying generic entecavir and tenofovir as tier 2 rather than tier 4 drugs in the Medicare formulary to reduce the patient’s out-of-pocket costs for HBV therapy.
ACKNOWLEDGMENTSThe authors thank Laura Cooley, MD at the CDC, for her assistance in reviewing our manuscript and for her helpful comments and suggested edits that contributed to the discussion.
REFERENCES 1. Buckley GJ, Strom BL. Committee on a National Strategy for the Elimination of Hepatitis B and C; Board on Population Health and Public Health Practice; Health and Medicine Division; National Academies of Sciences, Engineering, and Medicine, eds Eliminating the Public Health Problem of Hepatitis B and C in the United States: Phase One Report. Washington (DC): National Academies Press (US); 2016. 2. Le MH, Yeo YH, Cheung R, et al. Chronic Hepatitis B prevalence among foreign-born and U.S.-Born Adults in the United States, 1999-2016. Hepatology. 2020;71:431–443. 3. Patel EU, Thio CL, Boon D, et al. Prevalence of Hepatitis B and Hepatitis D Virus infections in the United States, 2011-2016. Clin Infect Dis. 2019;69:709–712. 4. Toy M, Hutton DW, So S. Population health and economic impacts of reaching chronic Hepatitis B diagnosis and treatment targets in the US. Health Aff (Millwood). 2018;37:1033–1040. 5. Kowdley KV, Wang CC, Welch S, et al. Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology. 2012;56:422–433. 6. Wong RJ, Brosgart CL, Welch S, et al. An updated assessment of chronic Hepatitis B prevalence among foreign-born persons living in the United States. Hepatology. 2021;74:607–626. 7. Bixler D, Zhong Y, Ly KN, et al. Mortality among patients with chronic Hepatitis B infection: The Chronic Hepatitis Cohort Study (CHeCS). Clin Infect Dis. 2019;68:956–963. 8. Centers for Disease Control and Prevention. 2019 Viral Hepatitis Surveillance Report. Accessed March 05, 2022. https://www.cdc.gov/hepatitis/statistics/SurveillanceRpts.htm 9. World Health Organization. Interim guidance for country validation of viral hepatitis elimination. June 2021. Accessed March 03, 2022. https://www.who.int/publications/i/item/9789240028395 10. Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 Hepatitis B guidance. Hepatology. 2018;67:1560–1599. 11. Cohen C, Holmberg SD, McMahon BJ, et al. Is chronic Hepatitis B being undertreated in the United States? J Viral Hepat. 2011;18:377–383. 12. Wong RJ, Jain MK, Therapondos G, et al. Low rates of Hepatitis b virus treatment among treatment-eligible patients in safety-net health systems. J Clin Gastroenterol. 2022;56:360–368. 13. Spradling PR, Xing J, Rupp LB, et al. Infrequent clinical assessment of chronic Hepatitis B patients in United States general healthcare settings. Clin Infect Dis. 2016;63:1205–1208. 14. Ogawa E, Yeo YH, Dang N, et al. Diagnosis rates of chronic Hepatitis B in privately insured patients in the United States. JAMA Netw Open. 2020;3:e201844. 15. Harris AM, Osinubi A, Nelson NP, et al. The hepatitis B care cascade using administrative claims data, 2016. Am J Manag Care. 2020;26:331–338. 17. Chao SD, Chang ET, Le PV, et al. The Jade Ribbon Campaign: a model program for community outreach and education to prevent liver cancer in Asian Americans. J Immigr Minor Health. 2009;11:281–290. 18. Bailey MB, Shiau R, Zola J, et al. San Francisco hep B free: a grassroots community coalition to prevent hepatitis B and liver cancer. J Community Health. 2011;36:538–551. 19. Entecavir and Tenofovir. In: RedBook. Green Village (CO): IBM Corporation; 2022. Accessed November 16, 2022. https://www.micromedexsolutions.com Subscription required to view. 20. Blue Cross Medicare Advantage 2022 formulary (list of covered drugs). Accessed November 16, 2022. https://www.bcbsil.com/medicare/pdf/2022/mapd-formulary-ppo-flex-il-2022.pdf 21. Ispas S, So S, Toy M. Barriers to disease monitoring and liver cancer surveillance among patients with chronic Hepatitis B in the United States. J Community Health. 2019;44:610–625. 22. CDC. Hepatitis B information. Accessed November 16, 2022. https://www.cdc.gov/hepatitis/hbv/patienteduhbv 23. Asian Liver Center at Stanford University. Brochures: Know HBV. Accessed November 16,2022. https://med.stanford.edu/liver/resources 24. Wong RJ, Khalili M. A patient-centered Hepatitis B Virus (HBV) educational intervention improves HBV care among underserved safety-net populations. J Clin Gastroenterol. 2020;54:642–647. 25. Chao SD, Wang BM, Chang ET, et al. Medical training fails to prepare providers to care for patients with chronic hepatitis B infection. World J Gastroenterol. 2015;21:6914–6923. 26. Mukhtar NA, Kathpalia P, Hilton JF, et al. Provider, patient, and practice factors shape Hepatitis B prevention and management by primary care providers. J Clin Gastroenterol. 2017;51:626–631.
留言 (0)