The frequency of IgG4-ROD ranges from 4 to 34% in IgG4-RD patients according to the largest case series published to date [10]. According to recent reports, IgG4-ROD is an emerging cause of uveitis, uveal masses, and scleritis with or without conjunctival infiltration and should be considered in any patient with multisystem inflammatory disease [3]. IgG4-ROD can mimic several infectious, inflammatory, and malignant disorders. More common causes of lacrimal gland masses, other orbital space-occupying lesions, scleritis, and uveitis should be ruled out before suspecting a diagnosis of IgG4-ROD [3].
In cases of orbital or intraocular masses, it is important to differentiate IgG4-ROD from malignant tumors (e.g. melanoma, lymphoma) and similar diseases [3, 5]. In our case, the MRI of the patient was quite similar to that of melanoma. Choroidal melanoma typically displays a high-intensity signal on T1-weighted images and a low signal intensity on T2-weighted images. Nevertheless, imaging findings may vary based on the degree of pigmentation and the presence of areas of necrosis or cavitation [11]. After gadolinium administration, the images showed intermediate-to-hyperintensity enhancement on T1WI [12]. At present, there is no established uniform description of the imaging findings for IGg4-ROD. IGg4-ROD has various imaging manifestations, including lacrimal gland type, ocular muscle type, mass type and diffuse type. In a study of Xiaoyan Wang, all types of IGg4-ROD were isointense or slightly hypointense on T1WI and slightly hyperintense on T2WI. The lacrimal gland type showed an obviously high signal on T2WI with fat suppression (fs). Moreover, if lymphoplasma cells and lymphoid follicles were predominant in the lesion, it appeared isointense or slightly hyperintense on T2WI. When fibrotic components were predominant, the lesion exhibited slight hypo-intensity on T2WI [13]. However, in another study of Lin Fu, the lacrimal gland type was found to be slightly hypointense on T1WI and isointense or slightly hypointense on T2WI. Contrast-enhanced imaging demonstrated a lesion with heterogeneous enhancement. The ocular muscle type, which is characterized by diffuse thickening of ocular muscles, presents blurred edges, slightly hyperintense T1WI, and marked reinforcement after enhancement [14]. In our case, we found that the lesion, which was located in the ciliary body area, appeared isointense or slightly hyperintense on T1WI, and hypointense on T2WI. Contrast-enhanced scanning showed progressive enhancement of the lesion. Therefore, we could not rule out the diagnosis of a malignant tumor by MRI before histopathological examination.
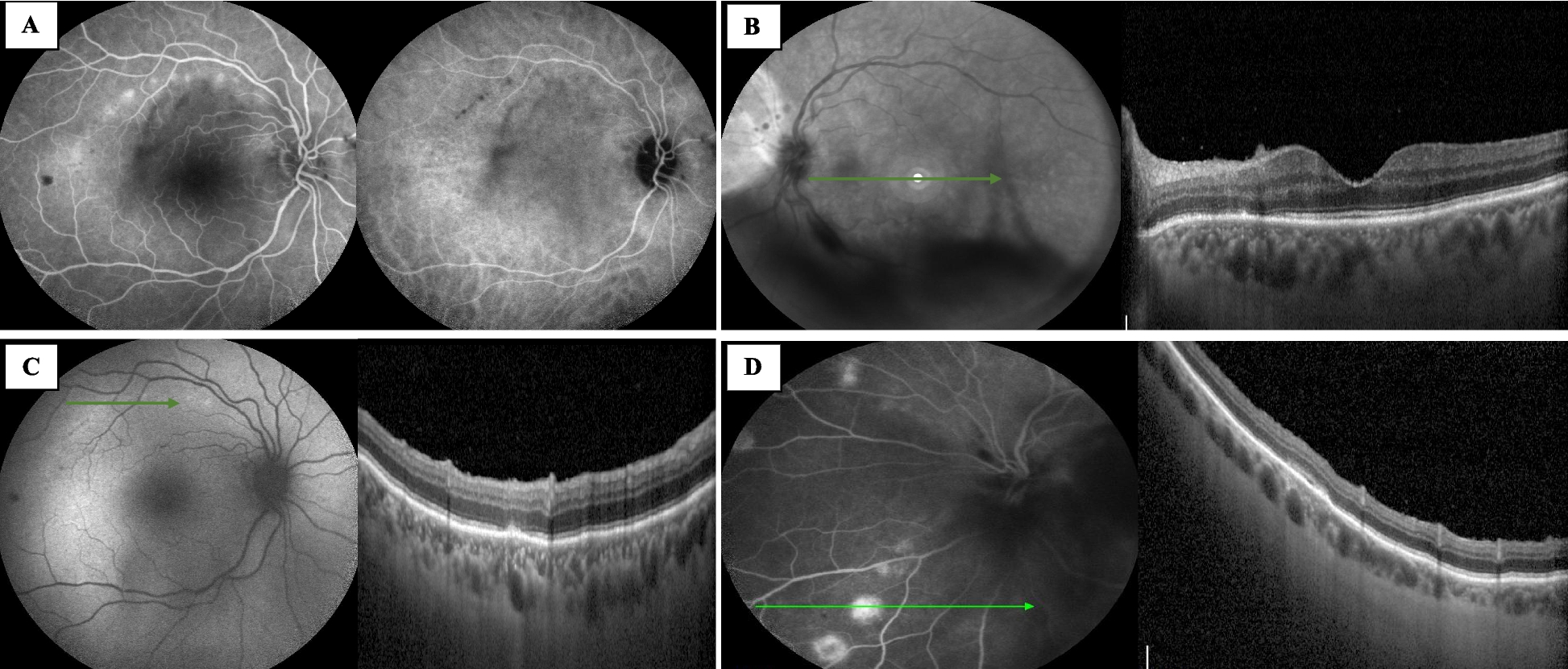
A long delay in the diagnosis of IgG4-RD remains common and may be responsible for irreversible sequelae due to extensive fibrosis [15]. Most reported cases of intraocular involvement have been unilateral. However, in the present case, both eyes were involved sequentially. The left eye was first involved and presented as a large intraocular mass and severe ocular inflammation, together with ERD, which displayed well on ophthalmic imaging including MRI, slit lamp photography, UBM, B-ultrasonography, and wide-angle fundus photography. Cytokine profile analysis showed a severe intraocular “inflammatory storm” characterized by an explosive rise of proinflammatory IL-6 together with increases in other tested inflammatory cytokines including IL-4, IL-10, TNF-α, and IL-17A. Immunohistochemistry (IHC) staining of the enucleated eyeball showed that the ratio of lgG4+/IgG+ cells was approximately 40%. The lymphoma and other ocular tumors were negative. Based on the diagnostic criteria for IgG4-ROD, the patient was diagnosed with probable IgG4-ROD. Lesions with similar features to the left eye (a ciliary body mass with ocular inflammation showed by ophthalmic imaging and cytokine analysis) were detected later in the right eye in the same patient, and systematic and local corticosteroids yielded satisfactory results, which further supported the diagnosis.
With advances in technology, several novel imaging modalities are available. Each modality has its pros and cons as well as its limitations. A combination of multiple imaging techniques can overcome these individual weaknesses and provide a comprehensive picture. Multimodal imaging is the concept of “bundling” images obtained from various imaging modalities that enable accurate localization and in vivo near-histologic assessment of ocular tissue, greatly aiding the clinician in establishing a diagnosis and monitoring the therapeutic response of ocular lesions. In the present case, we combined techniques including MRI, slit lamp photography, UBM, B-ultrasonography, and wide-angle fundus photography to evaluate ocular lesions. Notably, the bulbar conjunctival swelling observed by slip lamp in the lesion location 40 days after treatment might be easily considered as a sign of aggravation. However, as a powerful ophthalmic imaging tool for detecting anterior segment lesions of the eye [16], UBM clearly depicts the location and dynamic accumulation of the subconjunctival fluid and the gradual shrinking of the mass, helping ophthalmologists to develop a proper therapeutic strategy.
Cytokines play essential roles in inflamed eyes. Elevated aqueous humor concentrations of cytokines have been reported for different types of uveitis, and diverse cytokine profiles have been shown to be characteristic of specific diseases [17]. Consequently, cytokine patterns may serve as diagnostic and prognostic monitoring tools for clinicians, but are also useful for understanding the underlying immunopathogenic mechanisms. The expression patterns of these cytokines in IgG4-RD involving ocular tissues have not been investigated. We analyzed Th1/Th 2/Th17 cytokine (IL-2, IL-4, IL-6, IL-10, TNF-α, IFN-γ and IL-17A) profile in the aqueous humor of both eyes and found significant increase of IL-6, a major proinflammatory cytokine, companied by slight to moderate increases of IL-4, IL-10, TNF-α and IL-17A, which indicated severe intraocular “inflammatory storm” in this IgG4-ROD case.
During treatment, ocular inflammation was effectively suppressed, and the levels of these cytokines were gradually restored. During the dynamic accumulation of the subconjunctival fluid after treatment with UBM, IL-6 showed a simultaneous gradual increase, indicating fluctuation of the intraocular inflammatory state. With resolution of the subconjunctival fluid and disappearance of the ciliary mass, the IL-6 level was readjusted to nearly normal according to the aqueous humor cytokine analysis. Our observations suggested that cytokine level detection is another effective tool for estimating intraocular inflammatory activity, monitoring disease progression, and evaluating therapeutic effect in IgG4-ROD.
A high rate of systemic IgG4-RD involvement exists in patients with IgG4-ROD, particularly in bilateral cases. In a retrospective observational case series study, 14% of patients with unilateral IgG4-ROD and 79% of patients with bilateral IgG4-ROD had extra-ophthalmic involvement [18]. The most common sites of extraocular involvement in IgG4-ROD are the salivary glands and lymph nodes [19, 20]. Given the high rate of extra-ophthalmic involvement, systemic examination and imaging (head, neck, chest, abdomen, and pelvis) of new cases of IgG4-ROD are recommended to identify other sites of involvement.
Systemic prednisone is recommended as first-line therapy because a high rate of response to prednisone is a common feature of IgG4-ROD. Immunosuppressive therapy may be required in steroid-sparing or steroid-resistant cases [1]. Ophthalmic diseases also respond well to glucocorticoids in many patients. However, relapses are frequent after tapering or discontinuing therapy and can progress to a chronic state [10]. Additional immunotherapy is necessary in some cases, including the use of cyclophosphamide, rituximab (the most specific biological treatment with high rates of remission), mycophenolate, methotrexate, cyclosporine, or azathioprine [1, 10]. A possible relationship between IgG4-ROD and lymphoma has been reported. Thus, prolonged surveillance of IgG4-ROD patients is advisable [21, 22].
IgG4-ROD can be challenging to diagnose as a new and rare entity, especially in cases of atypical features, such as ocular mass, conjunctival infiltration, uveitis, or scleritis. It should be suspected in any chronic inflammatory ophthalmological manifestation after excluding the more frequent alternative diagnoses. Combined with ocular cytokinome profiles, multimodal imaging can help detect lesions, monitor disease progression, and guide therapeutic strategy.





留言 (0)