
記住我









Transcatheter aortic valve implantation (TAVI) has emerged as a valuable alternative to surgical aortic valve replacement (SAVR) in the treatment of severe aortic stenosis (AS) across different surgical risk groups.1–7
TAVI has grown in numbers and are catching up with SAVR or even exceeds the number of SAVRs in various European countries,8–10 UK11 and in the USA.12 However, considerable variation in the adaptation of TAVI exists in Europe.13 The 2021 European guidelines on the management of valvular heart disease14 favour TAVI over SAVR in older patients (≥75) or patients with a high surgical risk (STS/EuroSCORE II>8%), whereas SAVR is favoured in younger patients (<75) with low surgical risk (STS/EuroSCORE II <4%). The 2020 American Heart Association guidelines15 favour TAVI in patients ≥80 years or in younger patients with life expectancy <10 years and patients with high surgical risk (STS>8%) and SAVR in younger patients (<65) or patients with life expectancy longer than 20 years.
Contemporary nationwide data assessing changes in aortic valve replacements (AVR) over time are needed to evaluate how clinical practice patterns have changed in the era of TAVI compared with the recommendations in the current guidelines. Thus, the objectives of this study were to compare the rates of AVRs in Denmark in the era of TAVI and to assess the proportion of AVRs stratified by age in accordance with the age recommendations presented in the current guidelines.
MethodsData sourcesDanish citizens are provided with a unique personal identifier making it possible to link multiple nationwide administrative registries.16 We used the following registries: The Danish National Patient Registry; the Danish Prescription Registry and the Danish Civil Registration System. The Danish National Patient Registry contains information on every hospital admission since 1977 including diagnosis codes reported by physicians at discharge. The registry also holds information on primary and secondary diagnoses, date of hospital admission and discharge. From 1994, primary and secondary diagnoses are coded using the International Statistical Classification of Disease 8th and 10th edition (ICD-8 and ICD-10). From 1996, surgical procedures were added to the registry.
The Danish Prescription Registry contains information on dates of prescription redemption and type of drug according to the Anatomical Therapeutic Chemical classification system.
The Danish registries are validated and of high quality and have been described previously.16–18
Study populationAll patients in Denmark with AS (ICD-8 codes, 39500, 39502, 39590, 39592; ICD-10 codes, I.350, I.352, I.060, I.062) undergoing AVR (NOMESCO Classification of Surgical Procedure Codes, KFMD00, KFMD10, KFMD11, KFMD12, KFMD14) in the period from 1 January 2008 until end of December 2020 were identified.19 20 All patients had a diagnosis of AS; however, a small proportion of the patients included had a concomitant diagnosis of aortic regurgitation prior to AVR.
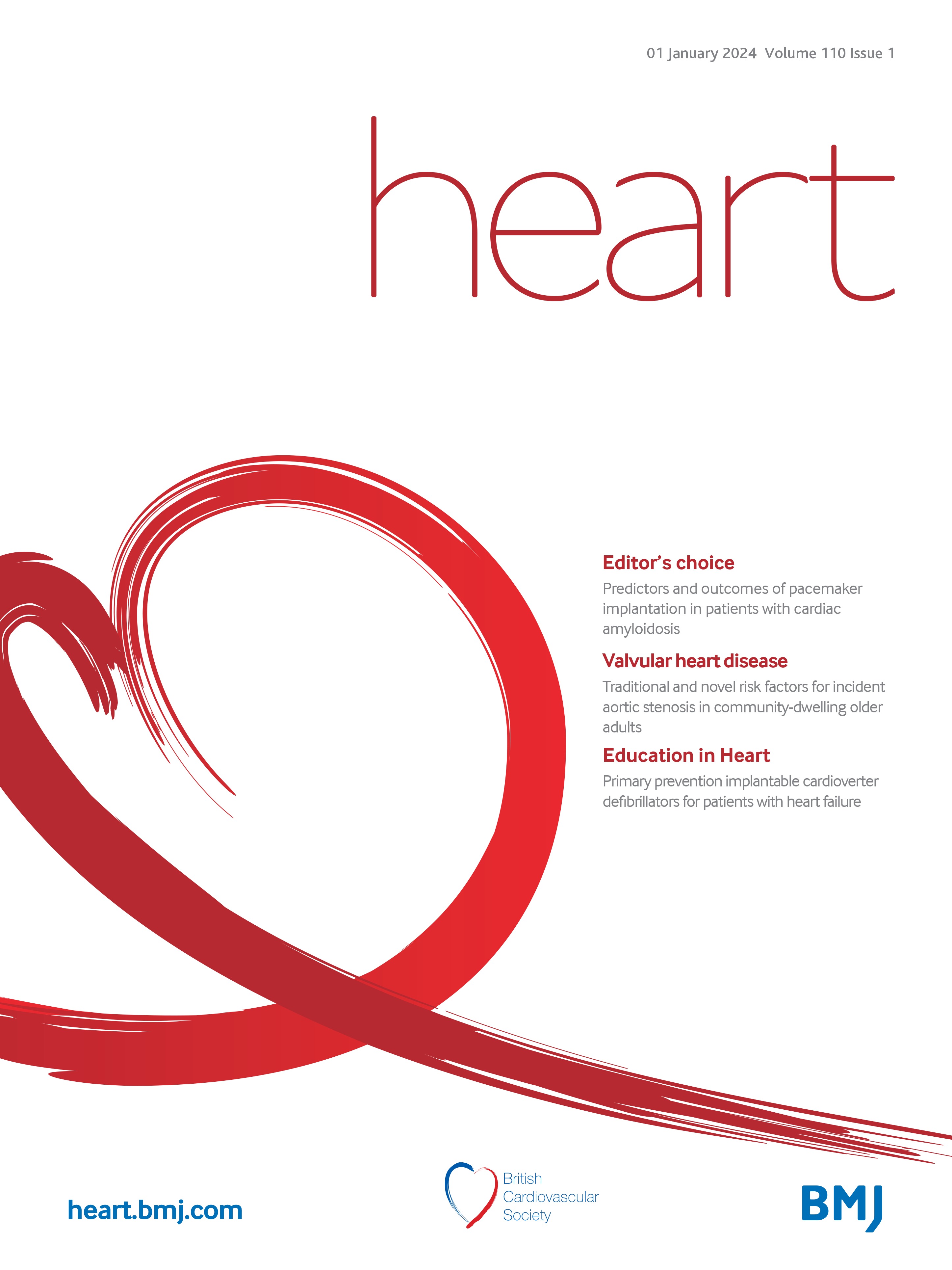
Patients with prior AVRs or aortic valve repair were excluded as were those who were discharged after end of the study (31 December 2020) or were hospitalised with a diagnosis of infective endocarditis close to time of AVR (discharge date of IE within 30 days of AVR). Patients receiving either a bioprostheses or mechanical prostheses with an additional procedure code of coronary artery bypass graft (CABG) (KFNA, KFNB, KFNC, KFND, KFNE) the same day as the AVR procedure were classified as combined SAVR (SAVR+CABG). Patients with concomitant other valve surgery or surgery on aorta were excluded. Patients who underwent percutaneous catheter intervention within 90 days prior to the TAVI procedure were categorised as undergoing prior revascularisation (TAVI+percutaneous coronary intervention (PCI))(figure 1).
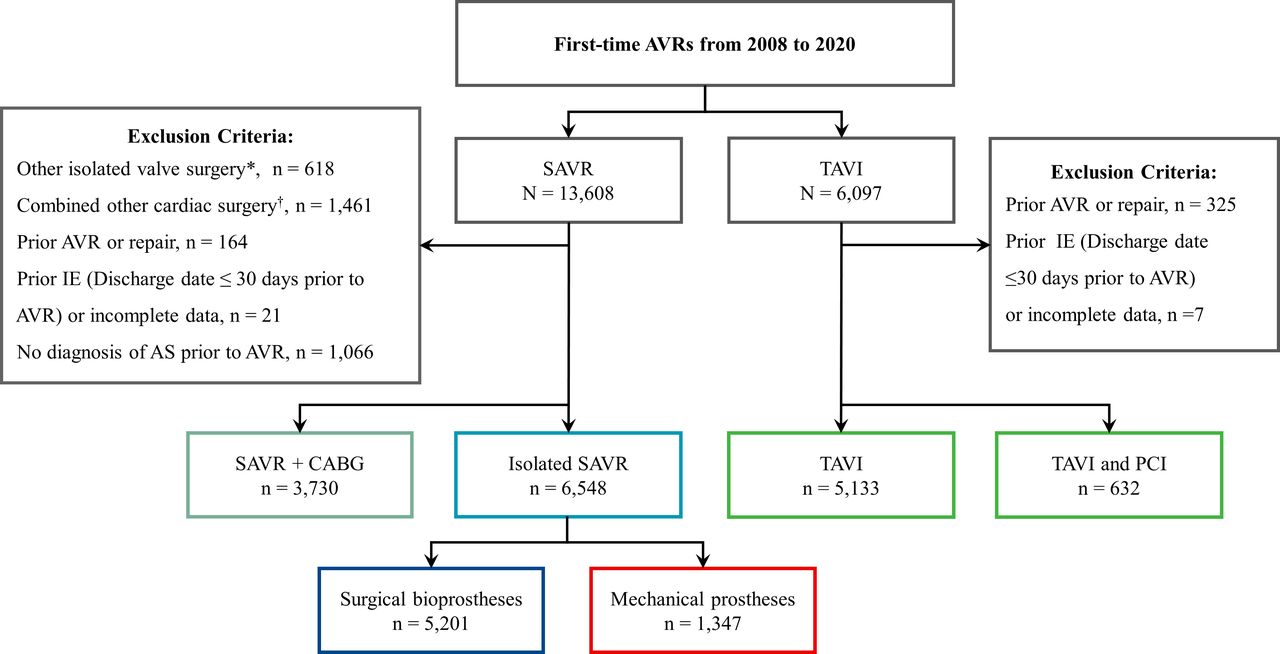 Figure 1
Figure 1 Flowchart of study population.Total population treated with AVRs between 2008 and 2020 and the numbers and type of AVR procedures performed. *Other isolated valve surgery was defined as other valve surgery combined with AVR without any other cardiac surgery. †Combined other cardiac surgery was defined as surgery on aorta or surgical ablation combined with AVR. AVR, aortic valve replacement; AS, aortic stenosis; CABG, coronary artery bypass grafting; IE, infectious endocarditis; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation.
The study cohort consisted of patients undergoing (1) isolated SAVR, (2) combined SAVR and CABG and (3) TAVI. In a sensitivity analysis, we divided TAVI into two groups TAVI+PCI as described above and isolated TAVI (no PCI 90 days before TAVI). Patients who underwent isolated SAVR were further grouped into two groups (surgical bioprostheses and mechanical prostheses) and compared with patients undergoing first-time TAVI. Further, the study cohort was grouped by calendar periods (2008–2011, 2012–2015 and 2016–2020) and age (two main age categorisations were defined (1) <75 and ≥75 years, (2) <70, 70–74, 75–79 and ≥80 years) to determine temporal trends across different calendar periods and age groups.
Characteristics, comorbidities and comedicationInformation on medical history prior to date of admission was obtained from the Danish National Patient Registry using ICD-8 and ICD-10 codes (online supplemental table 1). Comorbidities were defined as primary or secondary diagnosis codes given during hospitalisation or in an outpatient clinic. Further, we calculated the original Charlson Comorbidity Index (CCI)21 to estimate the cumulative comorbidity burden (online supplemental table 2).
Comedication prior to baseline was defined as a filled prescription for a specific drug-group within the last 6 months prior to the date of AVR. Hypertension was defined as having at least two antihypertensive drugs collected at a Danish pharmacy within 6 months prior to baseline, as described previously.22 Diabetes was defined from a prescription of any glucose lowering medication 6 months prior to baseline or an ICD-8/10 code of diabetes. Length of hospital stay was defined as time in days from AVR surgery until hospital discharge in same admission.
Statistical analysisBaseline characteristics of the study population were presented as median and 25th–75th percentiles for continues variables and in counts and percentages for categorical variables. CCI was categorised into three groups according to the total CCI score (CCI: 0, CCI: 1–2 and CCI ≥3). The annual rate of AVRs was calculated as the total number of AVR procedures performed in the investigated year divided by the population size determined on 1 January the following year. Trends in patient characteristics over time were estimated by the Cochran-Armitage test (two levels) and Cochran-Mantel-Haenszel test (>2 levels) for binary and categorical variables. For continuous variables, time trends in patient characteristics were evaluated with the Mantel-Kendall trend test and quantile regression for non-normally distributed variables and linear regression for normally distributed variables. All trend tests were calculated over each calendar year from 2008 to 2020. All tests were two-sided, and the level of statistical significance was defined as p<0.05. Data management and statistical analysis were performed in SAS Enterprise 7.1 (SAS Institute, Cary, North Carolina, USA) and R software V.3 (R Foundation for Statistical Computing, Vienna, Austria).
Patient and public involvementPatients or public were not involved in the design, or conduct, or reporting, or dissemination plans of this research study.
ResultsPopulation and baseline characteristics during study periodWe identified 16 043 first-time AVRs between 2008 and 2020 with a diagnosis of AS prior to AVR in Denmark. Isolated AVRs were performed in 12 313 patients of which 53.2% were SAVR (n=6548) and 46.8% were TAVI (n=5765). AVR combined with revascularisation accounted for 27.2% of all first-time AVRs (n=4362); of these, 85.5% were SAVR and CABG (n=3730) and 14.5% were TAVI and PCI (n=632). In the isolated AVRs, the median age was 76.2 years (25–75th percentile, 67.7–82.2) and 7290 were males (59,2%).
Median age decreased significantly over time for both surgical bioprostheses and mechanical prostheses. In patients undergoing TAVI, median age remained stable during study period. The proportion of males increased significantly in patients receiving TAVI or surgical bioprostheses and remained stable in the mechanical prostheses group (ptrend=0.131). Burden of ischaemic heart disease and heart failure decreased over time in all types of AVR. Diabetes remained stable all groups. Malignancy significantly increased in both SAVR and TAVI. CCI decreased over time in both TAVI and surgical bioprostheses (ptrend<0.001) and remained stable in mechanical prostheses (table 1). Comparable trends were observed for patients undergoing SAVR+CABG (online supplemental table 3).
Table 1Baseline Characteristics of isolated AVR
AVR practice patterns over timeThe total number of AVR procedures including concomitant revascularisation increased with 39% from 174.7 per 1 million inhabitants in 2008 to 242.5 per 1 million inhabitants in 2020 (ptrend<0.001)(figure 2). The increase in total AVR procedures was driven by an increase in TAVI (10.0 per 1 million in habitants in 2008 to 155.8 per 1 million inhabitants, ptrend<0.001). TAVI exceeded the total number of SAVRs in 2017 and accounted for 64.2% of all AVRs in 2020.
 Figure 2
Figure 2 Annual rate of AVRs over time.The number of AVRs performed between 2008 and 2020 per million inhabitants grouped by type of AVR, total AVR in purple, total SAVR in orange, surgical bioprostheses in blue, mechanical prostheses in red, SAVR+CABG in dim green and TAVI in green. AVR, aortic valve replacement; CABG, coronary artery bypass grafting; SAVR, surgical aortic valve replacement; TAVI, transcatheter aortic valve implantation.
In isolated AVR, a similar trend was observed for TAVI, which accounted for more than 70% of all isolated AVRs in 2020 (online supplemental figure 1). Analysing isolated AVR’s further, use of surgical bioprostheses increased from 2008 to 2012 followed by a stable period from 2012 to 2014, subsequently a stepwise decline was observed. Mechanical prostheses declined throughout the study period (ptrend<0.001). Assessing AVR in combination with revascularisation, TAVI+PCI increased from 3.1% in 2008 to 37.3% in 2020 with a proportional decline in SAVR+CABG (ptrend<0.001)(online supplemental figure 2). TAVI access approach changed during study period. Use of transfemoral approach increased over time and constituted 96% in 2020 (online supplemental figure 3). In table 1, numbers and percentages of TAVI access approach are shown for the three calendar periods.
Length of hospital stay according to type of isolated AVRThe length of hospital stay declined over time for all types of isolated AVRs (figure 3). The most pronounced decline in length of hospital stay was observed in the TAVI group, with a decline from a median of 9 days in 2008 to 2 days in 2020 (ptrend<0.001). In surgical bioprostheses, length of hospital stay declined from a median of 9 days to 6 days (ptrend<0.001). In patients who received mechanical prostheses, the length of hospital stay was stable over time. In table 1, the median length of hospital stay is shown for three calendar periods for each type of AVR.
 Figure 3
Figure 3 Length of hospital stay according to type of isolated AVR.Median length of hospital stay in days (values in bolt), error bars represent 25th–75th percentile. Median length of stay defined as date of AVR until date of discharge. Surgical bioprostheses in blue, mechanical prostheses in red and TAVI in green. AVR, aortic valve replacement; TAVI, transcatheter aortic valve implantation.
Utilisation of isolated AVRs according to ageIn patients aged <75 years, 5565 isolated AVRs (81% isolated SAVR and 19% TAVI) were performed compared with 6748 isolated AVRs (30% isolated SAVR and 70% TAVI) performed in patients ≥75 years. In patients aged <70 years, the proportion of surgical bioprostheses showed a minor annual increase until 2013 and subsequently declined during the rest of the study period. The use of surgical bioprostheses in patients aged ≥75 years declined during the study period (ptrend=0.001). The proportion of TAVI increased in both age groups most pronounced in patients aged ≥75 years (ptrend<0.001 in both age categories). In 2020, TAVI accounted for 91.5% of all isolated AVRs in elderly patients aged ≥75 years (figure 4). Same patterns were observed in the analysis with four age groups. TAVI increased in all age groups and was the predominant use of isolated AVR in patients aged >70 years in 2020 (ptrend<0.001). Use of mechanical prostheses declined during study period in patients aged <70 years and surgical bioprostheses was the most predominant choice of AVR after 2010 in this age group (online supplemental figure 4).
 Figure 4
Figure 4 Annual proportion of isolated AVRs according to age.The proportion of isolated AVRs performed between 2008 and 2020 according to the type of AVR in two age categories (<75 and ≥75 years). Surgical bioprostheses in blue, mechanical prostheses in red and TAVI in green AVR, aortic valve replacement, TAVI, transcatheter aortic valve implantation.
DiscussionWe present nationwide, complete and contemporary data on clinical practice patterns of first-time AVRs for AS in Denmark between 2008 and 2020. Our main findings can be summarised as follows: first, the rate of AVRs per million inhabitants increased with 39% and even higher when looking at isolated AVRs from 2008 to 2020, driven by an increased use of TAVI (figure 2). Annual proportion of TAVI increased and accounted for 64% of all AVRs and 72% of all isolated AVRs in 2020. Second, among elderly (≥75 years), TAVI increased and accounted for >90% of all isolated AVRs in 2020. Third, the use of TAVI increased in younger patients and since 2014, the absolute number of performed SAVRs (both isolated and combined with CABG) declined in Denmark.
The number of AVRs has increased over the last decade in Denmark and TAVI has become the dominant form of isolated AVRs for treatment of severe AS, in agreement with prior study results.23 Similar trends have been reported in other European countries.8–10 The overall increase in AVR procedures may be ascribed to several factors, an increased awareness of TAVI as a treatment option for a wide range of patients, including patients in extremely high or high surgical risk1 and patients >85 years regardless of their calculated surgical risk. These groups were more often treated conservatively in the past. Second, better diagnostics and more attention to AS will likely also influence our results and we expect an increased prevalence of AS with increasing age in the population. Last, two recent randomized controlled trials (RCT) concluded that asymptomatic patients with severe AS had lower mortality rates for SAVR compared with patients who received conservative care.24 25 This could partly explain the increase in numbers of AVR because of an increased referral of patients with asymptomatic AS.
Regarding, the choice of prosthesis type, surgical bioprostheses became the dominant prostheses type in patients aged <70 years in 2010 (online supplemental figure 4). This may reflect a transition to the use of surgical bioprostheses in younger patients, because valve-in-valve TAVI can be used in cases of surgical bioprosthesis valve deterioration in the lifetime management of severe AS in young patients.26 As a result, the choice of surgical bioprosthesis type and size is also becoming increasingly important. Similar trends were observed in a study from Germany10 and from the eastern part of Denmark.23 In the USA, the number of performed isolated SAVR began to decline in 2015 and onwards.12 In other European countries, isolated SAVR remained stable.8 9 The reason for this is likely differences in adaptation of TAVI across European countries.13
In patients aged ≥75 years, TAVI markedly increased >90% of all isolated AVR procedures in 2020 (figure 4). Thus, in Denmark the treatment strategy of patients with severe AS is in accordance with the age recommendations in the current European Guidelines favouring TAVI in elderly patients ≥75 years.14 An important observation in our data was that use of TAVI also increased in the younger patients (<75 years) during study period. In fact, TAVI exceeded the use of isolated SAVR in patients with aged between 70 and 74 years in 2020 (online supplemental figure 4). Thus, in Denmark, TAVI is used in younger patients beyond the favoured age cut-off according to the European guidelines.14
The risk profile of SAVR and TAVI patients improved over time with a decreasing burden of comorbidity, in line with previous studies.8 9 12 23 27 In the case of TAVI, this may be explained by an increased use of TAVI in younger and lower-risk patients and treatment of older patients with fewer comorbidities. In the case of SAVR, only younger patients and patients with low surgical risk are still treated with SAVR.
The length of hospital stay was significantly reduced over time for both isolated SAVRs and TAVI, most pronounced in TAVI (figure 3), in line with previous study from the USA.12 The decline in length of hospital stay may be explained by improved procedural techniques, including vascular access sites. Further, an overall decrease in comorbidity burden could explain the decrease in length of hospital stay especially in patients receiving surgical bioprostheses.
The increase in use of TAVI in younger patients appears to reduce use of surgical bioprostheses. However, SAVR is still favoured in younger patients (<75 years) with a longer life expectancy mainly because data on the long-term valve durability of TAVI are sparse. Results from the Nordic Aortic Valve Intervention trial (NOTION) showed that the 8-year durability of TAVI was comparable to that of SAVR in an older (mean age 79.4 in TAVI group) low-risk population.28 Few studies have reported the performance of TAVI in low-risk younger patients, with a mean age of 73–74 years.5 6 29 Although the follow-up time is limited, TAVI has shown acceptable clinical outcomes compared with SAVR in short-term follow-up.26 Further studies are warranted to investigate long-term durability of TAVI in younger patients. The NOTION-2 trial comparing TAVI to SAVR in patients aged 75 years or younger, should provide important answers (NCT02825134). Current practice in Denmark shows that most elderly patients (>90%) are treated with TAVI. This is in accordance with the age recommendations from the European14 and American guidelines.15 One might speculate that TAVI completely overtakes isolated SAVR in uncomplicated cases of AS. However, most patients with concomitant coronary artery disease are still treated with SAVR combined with CABG, although we observed an increase in the use of TAVI combined with PCI (online supplemental figure 2). This tendency could be expected to increase continuously due to increasing experience with complex percutaneous coronary interventions and chronic total occlusions. One may expect that SAVR will be used more predominately in complicated cases or where concomitant surgery is needed (ie, ascending aortic surgery, infective endocarditis, or bicuspid valve) in the future.
Strengths and limitationsThis study has some limitations. First, we used administrative registry data with limitations inherent to this type of data. Second, all analyses rely on correct diagnosis coding; however, the procedure and ICD-10 codes in the Danish registry have been validated with high performance corresponding to positive predictive values (PPV) of 99% (95% CI 95 to 100) in aortic valve surgery20 and PPV of 98% (95% CI 90 to 100) in the diagnosis of AS.19 Third, some important clinical data, such as echocardiography measures, are missing in our registries which could have provided useful information about the severity of the AS and data regarding patient-prosthesis mismatches. Although all patients had a prior diagnosis of AS, some cases of SAVR might have more aortic regurgitation than AS. We did not have access to referral time in the registries and could not assess how waiting time for AVR has changed in relation to the increased rate of AVRs over the last decade, or how mortality has changed while on the waiting list. We could not distinguish between patients admitted with IE and developing IE during admission for AVR. IE during initial AVR admission (early IE) is extremely rare. Thus, we excluded patients with IE discharge date near the date of AVR. Last, we were not able to reliably calculate surgical risk because of missing information on one or more of the risk factors contained in the validated risk scores used in clinical practice (EuroSCORE II or STS).
留言 (0)