Study population and grouping
This study retrospectively enrolled 190 TAK patients admitted to the Department of Rheumatology and Immunology, Beijing Anzhen Hospital, from October 2014 to June 2021. All patients were diagnosed with TAK according to the criteria for the classification of TAK developed by the American College of Rheumatology in 1990 [14]. Patients with other autoimmune diseases, liver and kidney dysfunction, cancer, or infections were excluded from the study.
Disease activity was assessed using a modified version of Kerr’s criteria [NIH (National Institutes of Health) score]; ITAS-A (Indian Takayasu’s Arteritis Activity Score with acute-phase reactants), and ITAS2010 (Indian Takayasu’s Arteritis Activity Score) [15, 16]. One item of IgG, immunoglobulin (IgA), or immunoglobulin (IgM) is higher than the normal range [IgA (g/L): 1.0–4.2, IgG (g/L): 8.4–17.4, IgM (g/L): 0.3–2.2] which was defined as the elevated immunoglobulin group. Immunoglobulins were detected by an automatic analyzer (Hitachi 7600–120, Tokyo, Japan).
This retrospective study was conducted following the ethical principles of the Declaration of Helsinki and approved by the Ethics Committee of Beijing Anzhen Hospital, Capital Medical University (number:2022244X).
Collection of clinical data
Data regarding age, sex, body mass index (BMI), disease duration, and clinical manifestation were recorded at baseline. Lesions were classified according to the angiographic classification of the 1994 International TAK Conference in Tokyo. Laboratory data were obtained from laboratory examination reports of the participating hospital. Numano classification of 1996 was adopted for image classification, divided into six types. According to the Numano standard, the imaging types of the patients were divided into six types (I, IIa, IIb, III, IV, and V) [17].
Method of pathology
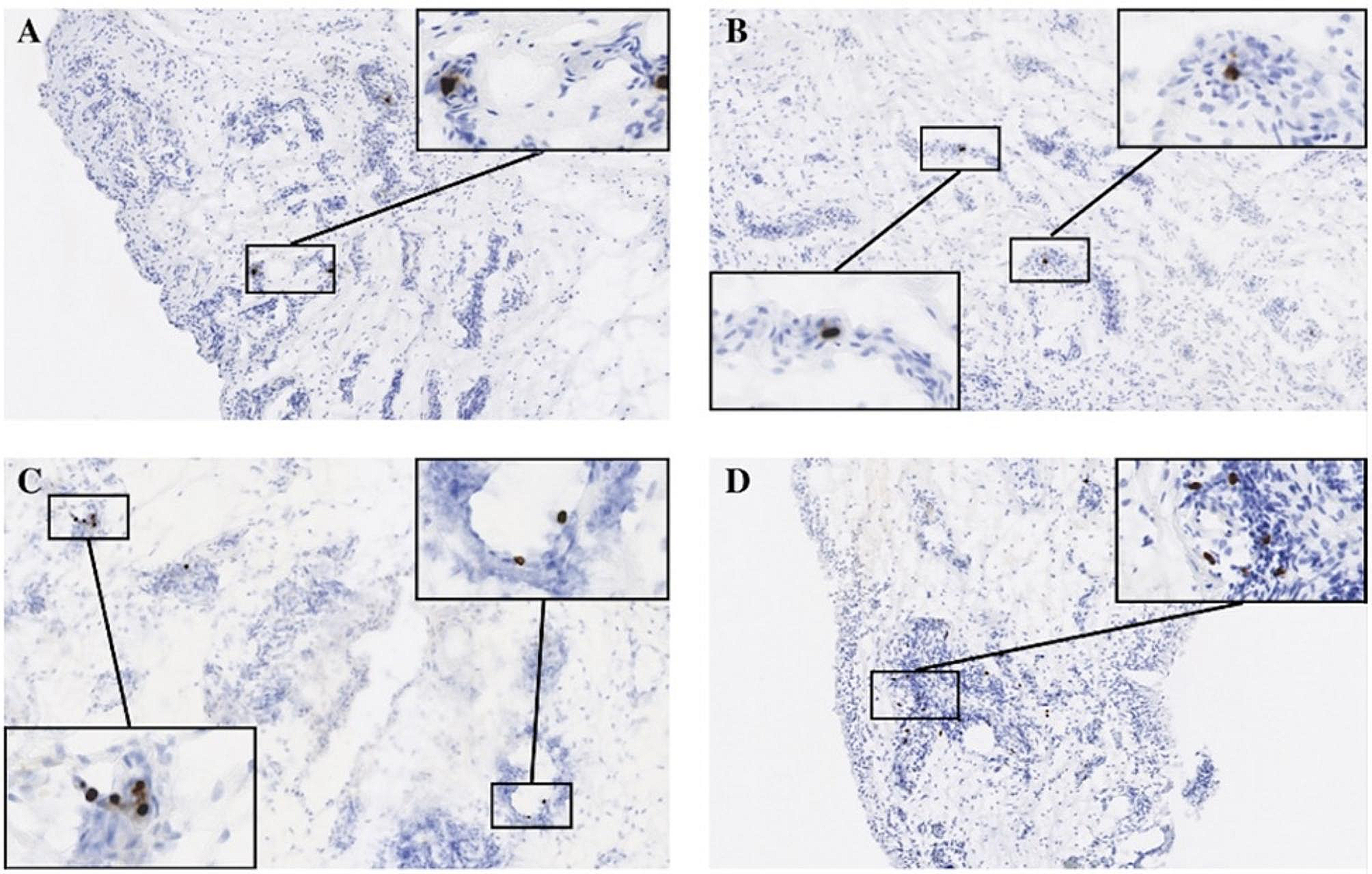
We collected surgically resected vessel specimens from four TAK and three atherosclerotic patients from the Beijing Anzhen Hospital from 2018 to 2020.
We processed the samples using immunohistochemical staining. Aortic specimens were fixed in 4% neutral formalin for 24 h, embedded in paraffin, and sectioned (4 μm). Then, they were stained with primary antibody for CD138 (Item No.ab46506, Abcam, Cambridge, CB2 0AX, UK) overnight at 4 °C and secondary antibody for 0.5–1 h at room temperature and detected with 3,3′-diaminobenzidine. Antibodies were diluted with triple-buffered saline (TBS) solution containing 1% bovine serum albumin (BSA).
A Nikon microscope eclipse 90i (Nikon, Tokyo, Japan) was used for image capture and analysis by the NIS-Elements BR 3.1 software (Nikon). Positive areas for immunohistochemical staining were measured in 8–10 areas of each section, and the mean value was expressed as a percentage of the total area.
Follow-up and outcome
Disease activity was assessed at 1, 3, and 6 months after discharge and every 6 months after that, and 130 of the 190 patients completed our follow-up. Of the 130 patients, 120 achieved remission within 3 months after discharge.
Remission was defined as the following: no clinical signs and symptoms of active TAK, normal ESR and CRP levels, and no evidence of progressive stenosis or dilatation in the involved vessels [18].
The outcome of this study was disease 1-year recurrence. Recurrence was defined as having any of the following conditions: (a) clinical features of ischemia (such as stroke and limb claudication) and (b) evidence of active aortic inflammation leading to progression of vascular involvement [18].
Statistical analysis
Normally distributed continuous variables were expressed as mean ± standard deviation (SD), and comparison between groups was analyzed by ANOVA. Skewed data were expressed as the median and interquartile range (IQR) and compared with the Kruskal–Wallis test. Categorical variables were expressed as numbers (percentage), and the chi-square test was used to compare between groups.
Correlation analysis (Pearson correlation analysis) was used to determine the relationship between increased levels of immunoglobulin and disease activity (NIH, ITAS-A, ITAS2010) and the relationship between changes in immunoglobulin and changes in disease activity and inflammatory markers. The results are expressed as correlation coefficients (r) and P value (P).
The comparison of positive areas for immunohistochemical staining in the TAK group and healthy controls was performed using the t-test.
In this study, logistic regression was used to evaluate the association between the elevated immunoglobulin and 1-year recurrence. Sex, age, duration of TAK, and BMI were adjusted as covariates.
All tests were bilateral, and P < 0.05 was considered statistically significant. All data analyses were performed by the R software (R-project ®; R Foundation for Statistical Computing, Vienna, Austria, ver. 4.2.1).

留言 (0)