
記住我

Four districts (equivalent to counties) were selected for the field trial. One of the districts was the no-intervention district, and the other three were intervention districts. In each selected district, four urban and four rural CHCs were selected. In each of the 32 selected CHCs, a baseline survey was conducted on 30–70-year-old residents of its catchment area to understand the existing status of NCDs risk factors. The survey was administered from June to September 2018 using a Persian translation of an adapted WHO stepwise approach to surveillance (STEPS) questionnaires [18]. Then, four different intervention packages were randomly assigned to the selected urban or rural CHCs in the intervention districts. In any intervention district, one urban and one rural CHC received intervention package A, one urban and one rural CHC received intervention package B, and so on (Fig. 1). The intervention period was 12 months, after which the second survey was conducted on the same age population in the 32 CHCs to assess the impacts of the interventions from September to November 2019.
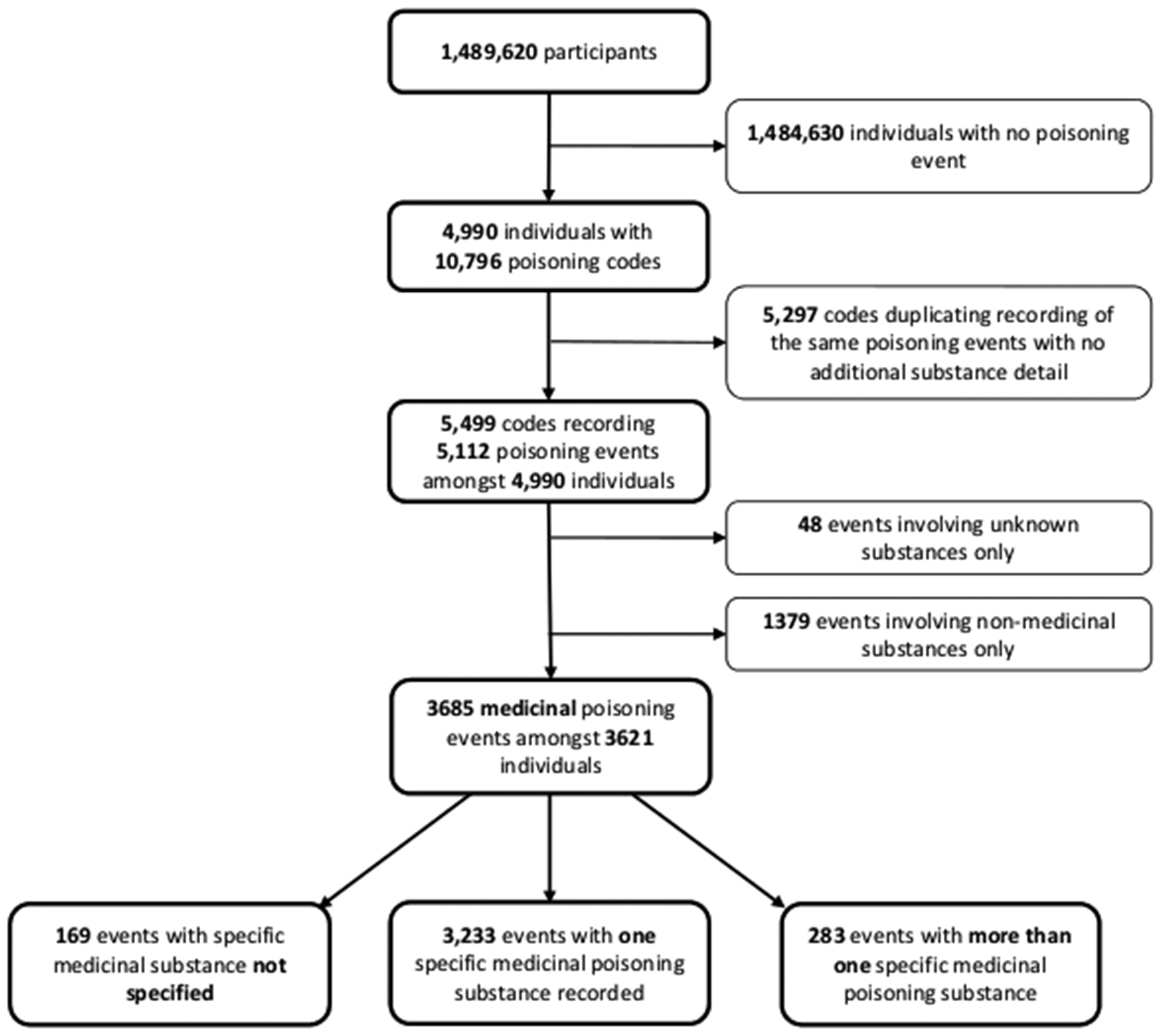
Fig. 1
CONSORT flow diagram. Note: Analysed based on population in first and second surveys. CHCs, Community Health Centers; UCHCs, Urban Community Health Centers; RCHCs, Rural Community Health Centers. a These three universities are located in three provinces of Tehran, Semnan, and Bushehr in Iran. One of the universities’ health care systems’ key tasks is providing primary health services to the covered population. b Shahriar, Dashtestan, and Damghan. c Garmsar
For each survey, a random sample of the population in the catchment area of each studied CHC was drawn. The sample size for each of the surveys was set to be 320 in each district; it was stratified by urban/rural CHCs, sex and age groups (30–39, 40–49, 50–59 and 60–69 years); 4 urban and 4 rural CHCs from each district were selected (totally, 12 urban and 12 rural in the intervention districts, in addition to the 4 urban and 4 rural in the “no intervention” district). So, the planned total sample size for each round of survey was 1280 [(12 + 12 + 4 + 4) * 40]. If we look at this number based on the intervention packages, the sample size was 240 for each of the intervention packages 1 to 4, and 320 for the no-intervention group [(4* 240) + 320 = 1280]. The sample size of 240 for each intervention group was enough to find a one-third decrease in the prevalence of 34% (based on a primary estimate for prevalence of physical inactivity) with an Alpha of 0.05 and a power of 80%. We used a higher sample size for the no-intervention group (320 versus 240) both to increase the power and to use a similar sampling protocole in all districts. As explained in the CONSORT flow diagram (Fig. 1), the final sample size in the 1st and 2nd surveys were 1226 and 1221 individuals, respectively. Since the cluster sample sizes were not proportional to the catchment areas’ population, sampling weights were used in all analyses. All interviews were in-person. If a household was not available at the first reach, it was contacted by the research team up to three times on three successive days to perform the interview. In each household, only one male and one female member from each of the following age group strata were interviewed: 30–39, 40–49, 50–59, and 60–70 years. If more than one male or female from an age group were living in a household, one of them was randomly selected and interviewed. A necessary inclusion criterion was informed consent by interviewees.
While the sampling method was similar in both surveys, the selected participants were not necessarily the same. Although the survey participants were expected to be among the target groups of the interventions, they were not necessarily the ones who received the intervention directly. According to the country’s Integrated Health Record System—called the SIB system locally [19]—on average, 20% of the catchment area population visit their local CHC in any given quarter. The country’s NPHWs’ reach, however, was expected to be much more than CHC’s direct utilization rate because, in addition to those who refer to them, they are responsible for improving the health of the entire population assigned to them. Based on how CHCs are structured and organized in the country, if individuals in a catchment area do not visit CHCs and demand health care, the NPHWs must reach out to them, encourage visits, or at least monitor their health remotely over the phone to make sure they are ceceiving health care somewhere else (such as the provate sector). This active follow-up method, especially in rural areas, has led to significant health improvements in the country, for example, remarkable decreases in maternal and childhood mortality and communicable diseases over several decades (Barzegar and Djazayeri 1981 [20], Rahbar and Ahmadi 2015 [21], and Keshvari et al. 2016 [22]). This study was built on the same infrastructures and intended to extend the NPHWs’ experiences regarding maternal and child health and communicable disease to non-communicable diseases.
Based on the approved protocol, the trial was planned to continue for 24 months, with a third survey at the end of the study. However, it was terminated prematurely after 12 months to comply with the country’s COVID-19 social distancing protocols.
The selected districts were Shahriar (population = 744,210), Dashtestan (population = 252,047), Damghan (population = 94,190), and Garmsar (population = 77,421) (Additional file 1). The districts’ populations are based on the country’s 2016 census [23]. A simple randomization method was used to select four urban and four rural CHCs in each district and to assign the intervention packages to the selected CHCs. Detailed explanations of the inclusion criteria for the districts, CHCs, and participants were explained in the protocol [24]. NPHWs implemented four intervention packages after receiving extensive training. Physicians were not the target group of this trial because they were undergoing a separate incentive payment scheme [25]. The CONSORT checklist can be found in Additional file 2 [26].
The interventions and intervention packagesAn intervention package in this study included the first, the first two, the first three, or all of the following interventions:
The first intervention (target-setting): Short-term targets (e.g., decrease in tobacco use and salt consumption) were set based on the preliminary results obtained from the baseline survey and the national goals to control NCDs behavioral risk factors. The national goals were to reduce insufficient physical activity, insufficient fruit and vegetable, salt intake, and tobacco use by 20, 30, 30, and 30%, respectively, until 2025 [27, 28]. Specific quarterly and yearly targets for NCDs risk factors are reported in Additional file 3. Meetings were held with the NPHWs of the selected CHCs, and they were informed about the status of NCDs behavioral risk factors in their catchment area population and the national goals to reduce them. Also, the proposed targets were presented to them, and they were encouraged to work through achieving them. The research team did not go beyond providing information on the status of NCDs in the catchment areas and national NDC goals, setting the goals mentioned above, and encouraging the NPHWs to achieve them. The second intervention (evidence-based education): The research team set up a 16-hour workshop for the NPHWs’ of the CHCs that received this intervention. The workshops were merely informational, during which the adverse health effects of overconsumption of salt, underconsumption of fruit and vegetable, insufficient physical activity, and tobacco use were extensively discussed. The trainees were provided with the related informational brochures as well. In addition, the team used Disease Control Priorities, 3rd edition [28, 29], and the Iranian version of the WHO package of essential NCDs (PEN) [30] to prepare a review summary of the effectiveness of the interventions aimed at decreasing the risk of NCDs in LMICs. The review also included success stories in other countries and methods of selecting, planning, and implementing cost-effective interventions. For the review.
The third intervention (operational planning): The research team coordinated with NPHWs and the local health experts to collaboratively devise operational plans for the selected CHCs in a 12-hour workshop. The major component of the NPHWs’ action plans was periodic (biweekly or monthly) educational sessions for the covered population on the causes and detrimental health effects of NDCs and practical methods to decrease the risk of NDCs (such as increasing physical activities, adjusting the diet, reading food products’ nutrition label, decreasing the consumption of salt, canned and fast food, and the use of tobacco products). Healthy lifestyle (especially in regards to movement and diet) and smoking reduction counseling was also offered to the CHC visitors. Other action plan items were organizing weekly public walking events, setting up group activities (such as painting, reading, and board games), and coordinating with government-owned sports facilities to provide free hours to the public (specifically, three two-hour sessions a week). The focus of the action plan was different from one CHC to another based on the finding of the baseline survey at the CHC’s catchment area. For example, if the body mass index was particularly high in a catchment area, more frequent educational sessions were set on the risk of obesity and the importance of physical activity, and more public walking events were organized by the NPHWs.
To support the action plans’ execution, the team allocated a supportive budget for the devised operational plans. The maximum supportive budget was 60 million Rials—equivalent to 556 United States dollars, USD, based on the exchange rate of 107,832 Rial/USD at the time of study [31]. The budget could be spent on purchasing equipment for the CHC (for example, digital blood pressure sphygmomanometers, body weight scales, and height measuring devices) and materials for educational sessions, group sports, and non-sport events.
The fourth intervention (performance-based financing or PBF): NPHWs of the selected CHCs received incentive payments. The payments were calculated at the CHC level, and paid to all NPHWs of that CHC per the pre-defined targets every 3 months. The average level of achievement of each center to its 3-month targets for eight different NCD behavioral and metabolic risk factors was quantified. The CHCs were then classified based on the percentage of their achievements into one of the following four groups: < 25, 25–49.99, 50–62.49, and 62.5% or more. These groups, respectively, received no incentive, one-third, two-thirds, and full incentive. The full monthly incentive was 10% of the average monthly salary of a typical NPHW in the studied districts, which was determined to be approximately 25 million Rial (or 232 USD). Therefore, the maximum monthly incentive payment was approximately 23 USD. No payment was delayed because they were made directly to the NPHWs’ bank account immediately after each assessment.
Intervention package A included only the first intervention, goal setting. Intervention package B included the first two interventions: goal setting and evidence-based training. Intervention package C included the first two interventions plus an action plan. In intervention package D, PBF was added to other interventions (Table 1). CHCs that received the intervention packages A, B, C, and D were also called intervention groups A, B, C, and D, respectively, in this study. The no-intervention district (Garmsar district) received neither of the interventions.
Table 1 Assignment of interventions to CHCs inside each of the three treatment districtsEvery two to four weeks, the implementation status of the interventions was reviewed and checked by the district and province supervisors selected by the research team. Also, reports on the interventions were received by the research team every quarter. The reports contained performance reviews per the set goals. Moreover, they included detailed accounts of the activities conducted at the CHCs that received an action plan. The key components of the reports were activities’ dates and type of the activity and the number of participants.
Statistical analysisThis study’s objective was to compare NCDs behavioral risk factors before and after the interventions and identify effective interventions. NCDs behavioral risk factors analyzed in this study were zero-one indicators of insufficient physical activity, insufficient fruit consumption, insufficient vegetable consumption, high salt intake, and tobacco use.
Not meeting the WHO recommendations on physical activity (Metabolic Equivalent of Task, MET, less than 600 METs per week) was defined as insufficient physical activity [32]. The WHO’s recommendations were used to determine insufficient fruit (less than two medium-sized fruits, such as two medium apples or half a cup of nuts, in the last 24 hours) and vegetable consumption (less than three cups of raw leafy vegetables or one and a half cups of cooked or chopped vegetables in the last 24 hours) [33,34,35]. A person was identified as a high salt consumer if the person always or often added salt or salt additives to the food [36]. Current tobacco smoking was defined as the use of any tobacco products, including cigarettes, cigars, or pipes, on a daily or non-daily basis in the last 30 days [37].
The prevalence of each NCDs risk factor in the baseline and second surveys was calculated in populations assigned with each intervention package. Then, the difference in the prevalence rates between the two surveys was calculated. For the more formal analysis of the effect of the designed intervention packages, the difference-in-difference (DID) design was employed. The following equation shows the linear specification of the DID design:
$$_=\alpha +\beta _+\gamma _+\rho \left(_\times _\right)+\theta _+\delta _+_$$
(1)
where i indicates a surveyed individual, c indicates the community health center to which the individual is affiliated, and t indicates the survey year. The dependent variable, Y, is a binary variable that indicates one of the NCDs behavioral risk factors for the individual. The variable IntPackage is a categorical variable with five values (0, 1, 2, 3, and 4), indicating the intervention package assigned to the CHC where the individual receives health services (Table 1). The value 0 was assigned to individuals surveyed in the no-intervention district. Therefore, four β s were estimated. Estimations of βA, βB, βC, and βD provide an adjusted comparison of the average level of dependent variable at the catchment areas that received intervention packages A, B, C, and D, respectively, to that in the non-intervention district. The variable Post indicates the survey year. It takes the value 0 if the individual was surveyed before the implementation of the interventions (2018) and 1 if surveyed after the trial (2019). The variable CHC is a community health center indicator (1, 2, …, 32), as any surveyed individual is affiliated with a specific CHC. This variable accounts for the influence of all unobservable/unmeasurable CHC-specific confounders that might not change over the study period (e.g., health care resources in the community, attitudes towards using modern medicine versus traditional practices, average distance from the CHCs, and overall weather patterns). The variable X is a vector of socioeconomic factors including age, sex, marital status (in three categories: never married, married, divorced or widowed), the level of education (in four categories: illiterate or primary, secondary, high school, and some college), labor market status (in six categories: public wage and salary job, private wage and salary job, self-employed, homemaker, retired, and unemployed), health insurance status, and homeownership status. The coefficients of interest in this specification are ρs (i.e., ρA, ρB, ρC, and ρD) which show the effect of the intervention packages versus no intervention among those surveyed after the intervention.
Given the binary nature of the outcome variables in this study, logistic models were used in fitting Eq. 1. Odds ratios were calculated, representing the change in the odds of the dependent variable being equal to 1 due to one unit change in either of the terms on the right-hand side of Eq. 1. Equation 2 is the logistic transformation of Eq. 1.
$$\mathit\left(\frac}}_}}\right)=\alpha +\beta _+\gamma _+\rho \left(_\times _\right)+\theta _+\delta _+_$$
(2)
where \(_}\) is the probability of the dependent variable Yict being reported as 1.
To account for the possibility that the NCDs behavioral risk factors (the Ys) may not be independently distributed within the population covered by each community health center, hence the estimated standard error be artificially low, standard errors were clustered at the CHC level [38]. Also, a sampling weight was assigned to the surveyed individuals. Sampling weights were calculated as the inverse of the ratio of sampled individuals characterized by sex and age group relative to the number of individuals in the respective sex and age group (namely, 30–39, 40–49, 50–59, and 60–70) in the population. For a specific individual, the ratio was the multiplication of two shares: (1) the share of surveyed individuals of the same sex and age group in the corresponding catchment area’s population, and (2) the share of individuals of the same sex and age group in the corresponding district in the country’s population. The shares were separately calculated for urban and rural areas.
The estimations were done with and without adjusting for the socioeconomic factors (X) to assess the extent of any potential observable bias in the selection of CHCs and the assignment of intervention packages. The statistical package used for analyses was STATA 14.0 (Stata, Inc., College Station, Texas).
Ethical issues/statementThis study has been approved by the national committee on ethics in medical research (code: IR.NIMAD.REC.1396.084) as well as our institutional review board (code: IR.IUMS.REC.1395.1057613). Written informed consent has been obtained from study participants.
留言 (0)