According to our findings we could confirm the hypothesis that extracting upper first premolars results in a more pronounced retroinclination and retroposition of the incisors. Furthermore, our results verify that second molar extraction increases orthodontic treatment time, but not statistically significant.
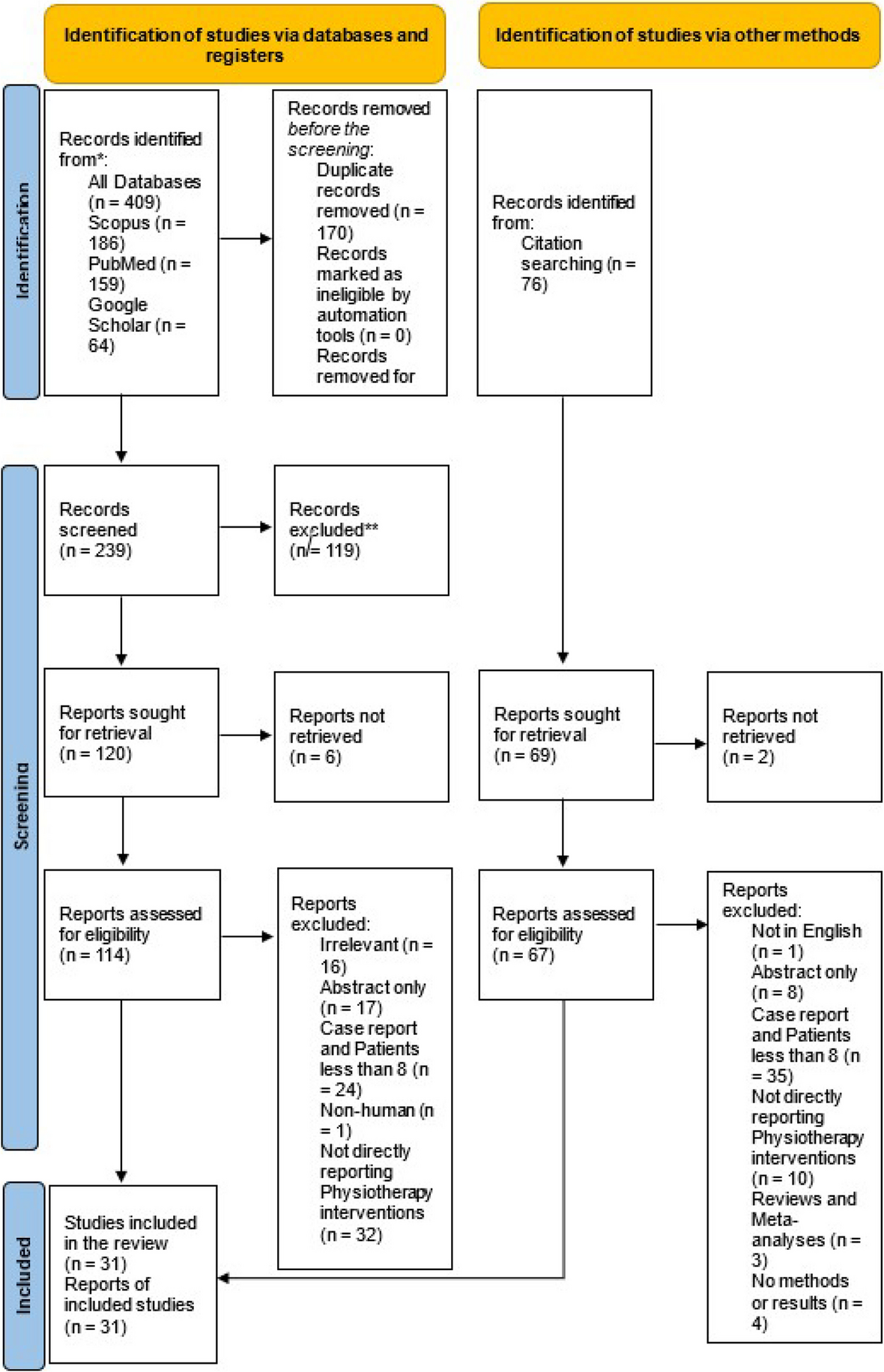
The study collective was not homogeneously distributed into the two groups concerning the number of participants and gender. This can be explained by the retrospective study design and the fact that the intervention was chosen by the patients independently of the study. Compared to previous publications about bilateral maxillary second molar extraction, our population was the biggest (N = 31) [17, 23].
Our results indicate no difference in orthodontic treatment duration (24.0 months group I, 21.9 months group II) between the two methods. A similar duration after second molar extraction is reported by Stellzig et al. (2.1 years) [5]. However, in the first months of treatment after second molar extraction only a headgear was used, and hence treatment time with fixed appliances was reduced. Furthermore, treatment devices using skeletal anchorage may present a shorter treatment time in both interventions without anchorage loss [24,25,26]. Especially in group I orthodontic treatment duration was influenced by patient compliance, which is required for successful distalisation of the first molars by headgear. However, patients with bad compliance were excluded.
Our findings revealed no statistically significant difference in pre-treatment chronological age between the groups (13.0 years group I, 12.6 years group II). Still, dental age is very important during timing of extractions, because it affects the surgical procedure and eruption of neighbouring teeth [8]. It is recommended that teeth are extracted after they have fully erupted to reduce invasiveness of the surgical procedure. Furthermore, in case of second molar extraction third molars should have their crowns calcified and their position assessable to allow successful placement into the arch. Additionally, some authors suggest that their vertical development should have reached the cemento-enamel-junction of the second molars [5]. In theory, extraction and orthodontic treatment could be started earlier in group II, because first premolars complete development and eruption earlier than second molars [27, 28]. However, this was not justified by our results and seems meaningful, since canines, which were the next teeth to be moved, usually develop later than first premolars, and because inclusion criteria required visibility of the upper third molars in orthopantomograms with good prognosis.
This study found relapse only after first premolar extraction, which is supported by the findings of Stellzig et al., who described space opening in 41% after first premolar extractions [17]. A possible explanation may be that dental crowding was smaller than the amount of space generated by sacrificing two first bicuspids. In contrast, after second molar extraction, the remaining space was used by the third molars. Another explanation for that difference may be that there was bias resulting from the exclusion criterion “bad compliance:” since headgear wear requires more compliance than fixed appliances, group I patients may have been more compliant in general. Hence, during the retention group I patients may have shown better compliance than group II participants, resulting in less relapse.
According to our results, third molars were not successfully aligned into the upper arch in some cases, especially after extraction of first bicuspids. In contrast, following maxillary second molar extraction third molars are often successfully aligned into the upper arch [8, 15, 17, 29]. This could be explained by the location of the extraction sites, as second molar extraction generates more space in the region of the maxillary tubera, because of the bigger tooth size and their adjacent location. Nevertheless, since the third molars were not controlled orthodontically, angulation and torque may be improper and the shape could be abnormal [30], requiring further orthodontic correction.
Concerning the cephalometric changes, in the sagittal direction (individualised) Wits-appraisal was significantly higher after first premolar extractions showing an increased distobasal jaw-relation. However, since the ANB angle was not significantly different, this observation was negligible. Compared to an untreated control group, Stellzig et al. found a significant reduction of SNA and ANB after extraction of four first premolars, but no significant differences after maxillary second molar extractions [17]. This can be explained by the patient collective, presenting a class II division 2 with no need for significant incisor retraction, and the results would have been different, if the entire dentition was moved a lot. Basdra et al., however, did report significant sagittal changes after upper second molar extraction: whereas SNA and ANB decreased, SNB increased [15]. In the vertical direction, we found a significant difference only for the index and facial axis, both indicating a more horizontal pattern in group I. Since the other vertical variables were comparable, this difference is of minor clinical relevance. Stellzig et al. reported a significantly smaller overbite after both interventions [17]. In another study Stellzig et al. found a reduction of overbite after second molar extraction in horizontally growing patients, who were expected to show further deepening without the intervention [5]. Dental parameters indicated more retroinclined incisors after first premolar extraction. This was also reflected in the increased concavity of the soft tissue profile in group II and is supported by other investigations [17]. However, thickness of the soft tissue and the anchorage applied must be considered. Due to the maximum anchorage in both groups, the effect of extracting premolars on front teeth and soft tissue can be explained by the incisors’ retrusion. Overall, the type of tooth extracted seems to affect mainly dental and soft tissue parameters, whereas skeletal variables are comparable.
An advantage of first premolar extraction is their location in the centre of the sagittal arch and thus the close position to the location of crowding and the possibility to solve anterior as well as posterior crowding [6]. Thus, in case of severe anterior crowding or pronounced proclined incisors, extraction of the first premolars may be more efficient. Concerning the vertical direction, second molar extraction followed by distalisation of the first molar decreases overbite, whereas first premolar extraction and consecutive mesialisation deepens the bite [31]. However, in this study maximum anchorage of the first molars was required, and hence no deepening occurred. To ensure controlled and bodily tooth movements fixed appliances were inserted directly after extraction of first premolars. Therefore, apart from oral hygiene, first premolar extractions may need less compliance than second molar extractions, which require patient compliance in headgear use. Extraction of maxillary second molars presents the following advantages: class-I-occlusion at first molars, reduced risk of relapse, improved inclination of dental axes, increased overbite reduction, less incisors’ retrusion with a better aesthetic profile, shorter orthodontic treatment time with fixed appliances and prevention of third molar tooth impaction [5, 6, 17, 32]. However, possible disadvantages of second molar extraction are their location in cases of anterior crowding because of the long distance to the crowding to be resolved, and the biomechanics required, which may be more challenging.
In this study cephalometric analysis included individualised norms for the ANB angle [19] and Wits appraisal [22], increasing diagnostic precision. However, only post-treatment situations were evaluated without considering pre-treatment patterns and changes during treatment, which reduces the expressiveness of our findings. Another limitation of this study is that growth was not considered, because it may have affected skeletal and dental parameters. Hence, the differences found cannot solely be attributed to the intervention and future investigations should evaluate pre-treatment cephalometry as well.
Our results can be generalised for skeletal class I or borderline class II/III cases, showing brachyfacial growth pattern, dental class II malocclusion and maxillary third molars calcified with good prognosis. In case of agenesis of the upper third molars, however, the extraction of second molars is not indicated. The findings only address compliant patients and treatment of non-compliant patients may result in different treatment outcomes, being better in the treatment with first premolar extraction, which requires less compliance.





留言 (0)