Restoring the depleted soft tissue volume using injectable fillers has become increasingly popular nowadays. Polylactic acid (PLA) is an aliphatic polyester. It is widely used for biomedical applications because its degradation products H2O and CO2 are neither toxic nor carcinogenic to the human body [2]. Owing to its safe application and long-lasting effect, PLA substances including poly-L-lactic acid (PLLA) and PDLLA have been rising stars in the cosmetic filler market [3, 4].
Animal studies of PDLLA application were conducted between September 2009 and May 2011. PDLLA microspheres were injected into the subcutaneous space of rats. PDLLA-induced cell inflammation was observed from the 2nd week and subsided in the 4th week. Cells, actin, and type-1 collagen were increasing near and inside the PDLLA microspheres from the 2nd to 20thweek post-injection. No abnormal finding was found at the injection site. Animal studies proved the efficacy and safety of PDLLA microspheres as subdermal fillers [5]. More studies of PDLLA as a filler were done and showed comparable efficacy and safety with hyaluronic acid for the correction of nasolabial folds [6,7,8].
Research performed by the manufacturer reported approximately 16,000 patients receiving facial injection of PDLLA filler from April 2014 to July 2018 with no serious adverse effects (i.e., death, blindness, and skin necrosis). Adverse side effects observed included mild swelling (50% of all patients), bruising (30%), and pain (20%) which were resolved or relieved with ice packing and medication [1]. Although previous studies showed safety of PDLLA as a subdermal filler, the present case had a major side effect of the multiple branch arterial occlusion after injection of PDLLA above the eyebrow.
Emergency treatment was administered to the case patient according to suggestions made by the management of a committee convened by the Society of Aesthetic Medicine (Singapore) [9]. They included the immediate lowering of intraocular pressure and dislodging the embolus to a more peripheral downstream location. We laid the patient down and administered one drop of topical Brimonidine tartrate 0.2%/Timolol maleate 0.5%. Followingocular massage that could also lower intraocular pressure, blood flow increased in the arterioles, potentially dislodging the embolus. Loh et al. also recommended supportive treatments including steroid pulse therapy and heparin infusion and HBOTafter immediate treatment [9]. Alprostadil as a vessel dilator had previously been used [10, 11], which helps move the emboli to a more distal part of the retinal artery.
With the outbreak of the coronavirus disease-2019 (COVID-19) pandemic, our HBOT building had been changed into a COVID-19 ward. HBOT was arranged immediately after reopening of the HBOT unit. The meta-analysis study conducted by Wu et al. in 2018 reported beneficial effect of oxygen therapy in improving visual acuity in retinal artery occlusion (RAO) patients, especially those treated with 100% HBOT and for over 9 h [12].
The present case had immediate vision loss after injection at the glabella area. A review study of 98 patients showed glabella (38.8%) as the most common injection site of iatrogenic RAO, followed by nasal region (25.5%), nasolabial fold (13.3%), and forehead (12.2%) [13]. The ophthalmic artery system branches into vessels including the supraorbital, supratrochlear, and dorsal nasal arteries. It has been suggested that injection at the glabella or inferior to the forehead should be superficial while injection on the forehead should be deep because supratrochlear artery and supraorbital artery become more superficial when they travel superiorly above the supraorbital rim [14].
Other prevention tips include aspiration before injection, avoiding overcorrection by using low volumes in two or more treatment sessions, and using botulinum toxin in the glabella first to reduce the severity of wrinkles before injecting soft tissue filler [15, 16].
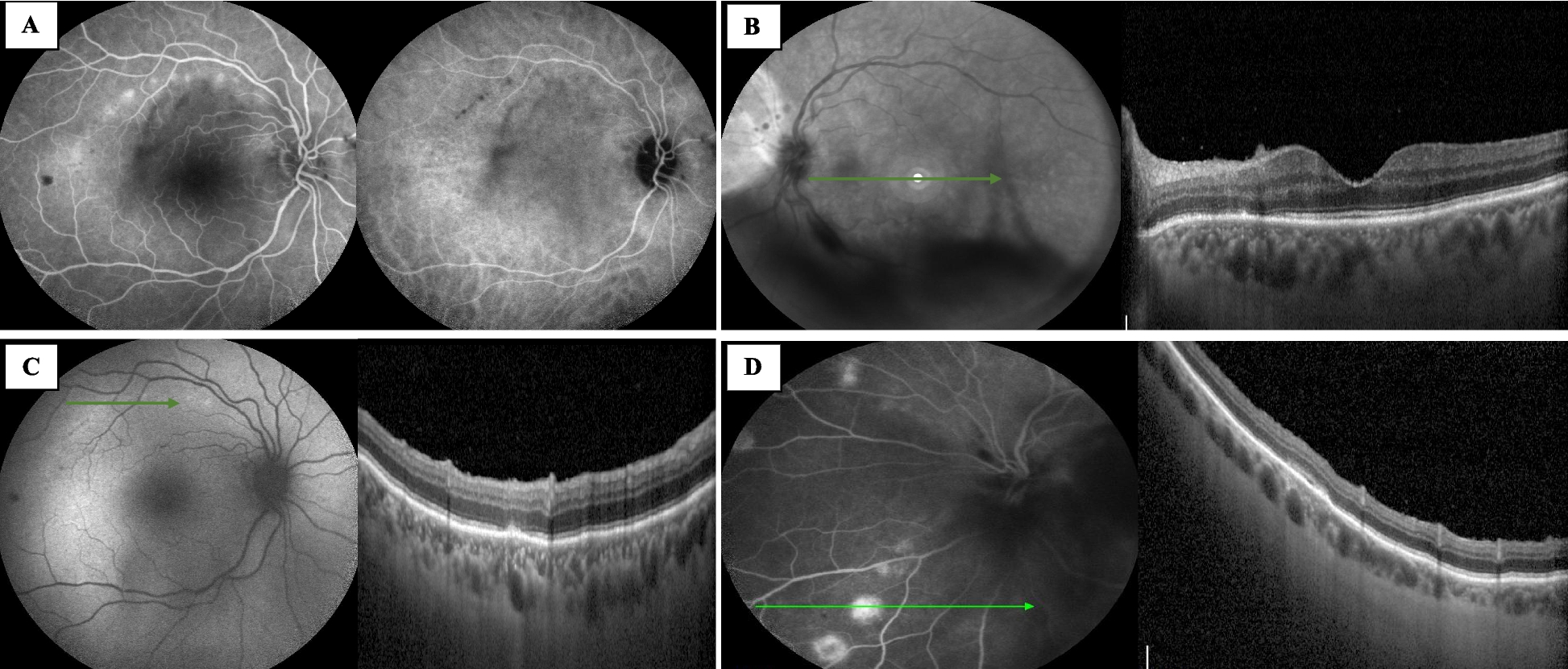
The pathogenesis of filler-caused RAO can be attributed to intravascular injection or penetrating the proximal branches of the artery or anastomoses vessels. The high pressure of injection can make the filler retrograde to the larger vessel. In our case, the filler retrograded from the supratrochlear artery to the ophthalmic artery then propelled forward to central retina artery and then occluded multiple branch retina arteries [13].
Treatment of RAO within a limited time from onset, known as the golden period, may achieve better VA. In CRAO, experimental monkey model showed the retina can only tolerate up to 97 min of CRA clamping without causing detectable injury [17]. Four hours of arterial occlusion results in massive irreversible retinal injury, therefore, the recanalization therapies were generally suggested within four hours [18]. However, in human, the time window was found to be 15 h in patients with central retinal artery occlusion (CRAO) caused by fibrinoplatelet embolization [15]. Early treatment appears to be as important in BRAO cases as it is in CRAO cases to avoid retinal damage after artery obstruction and ischemia. One study suggests 24 h threshold time for the conventional treatment for BRAO [19]. The present case came to our ED after 5 h of symptom onset and initial visit to another hospital. The ophthalmologist there informed the patient of poor prognosis but performed no treatment. This article aims to bring attention to possible improvement of visual acuity within the human time window.
In conclusion, retinal artery occlusion can be a devastating side effect after cosmetic facial filler injection. Physicians who provide the filler service should pay attention to the location and level of injection, signs and proper referral of iatrogenic RAO. Although safety of PDLLA was confirmed in animal studies and prior application on 16,000 human cases without serious adverse effects, it could still cause the rare but devastating complication of RAO. This is the first reported case of PDLLA-related RAO worldwide. Proper and immediate therapies could still improve patient’s vision and scotoma. Ophthalmologists should keep in mind the possibility of iatrogenic filler-related RAO. Further treatment guidelines and investigations are needed.





留言 (0)