XLRS is a congenital retinopathy with variable natural history [5, 13]. The visual acuity of most patients remains relatively stable or gradually declines in childhood and may suffer further deterioration due to macular atrophy in adulthood [4], while others may suffer sudden severe deterioration at a younger age due to complications like RD and VH [13, 14]. Macular and peripheral retinoschisis are typical features of XLRS, with previous reports in the literature ranging from 68% to 100% and 43% ~ 60%, respectively [7, 15]. We report macular schisis in 86.5% and peripheral retinoschisis in 79.3% of the eyes in our cohort, which is relatively high, possibly due to the younger age of our patients, considering the macular and peripheral retinoschisis will collapse and change into atrophic manifestation later in life [13]. We report inner layer breaks in 55.2% and outer layer breaks in 5.3% of the eyes in our cohort, which is in accordance with the previous report of inner layer breaks in about 52% of the eyes and outer layer breaks being rare but without precise percentage [15]. We report RD in 21.6% of the eyes, compared with 5.5–16% in previous reports [9], and vitreous hemorrhage in 20.9% of the eyes, compared with 3–21% in previous reports [9].
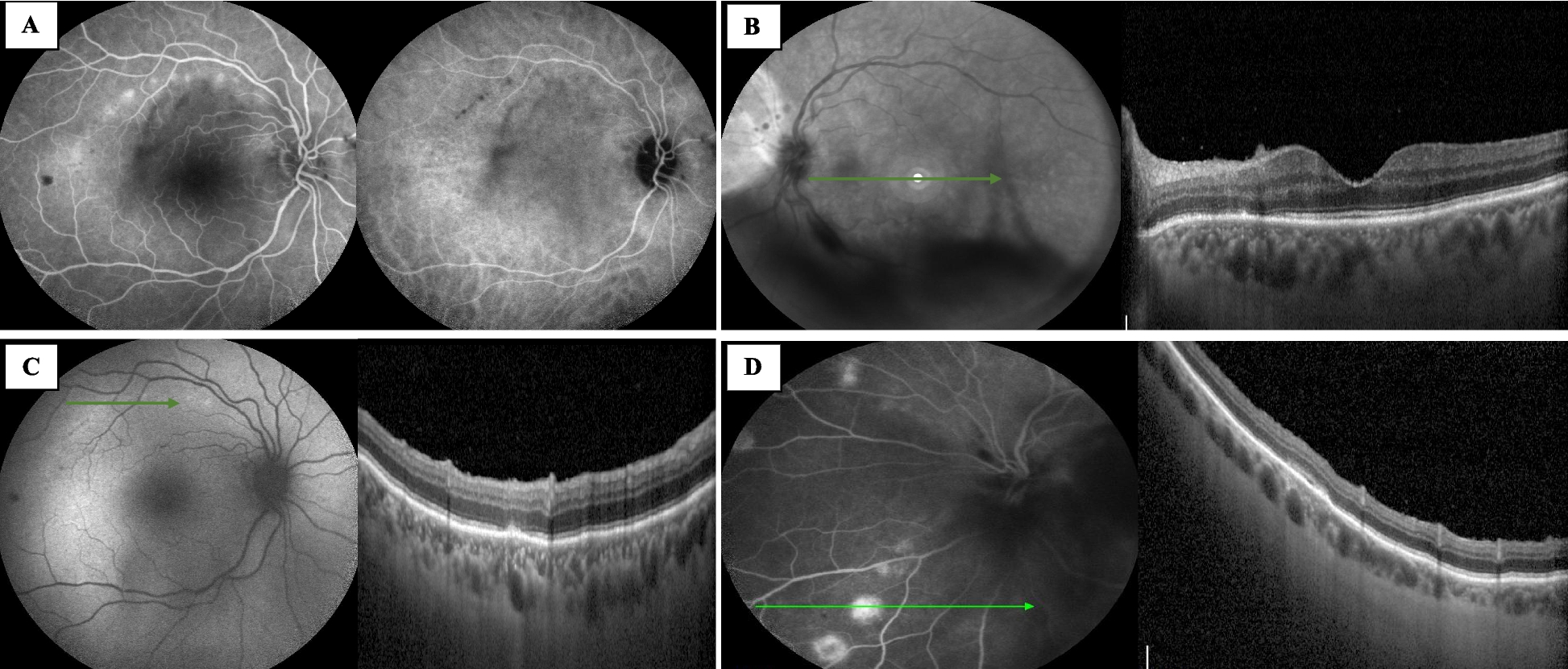
We report, for the first time, the clinical characteristics of honeycomb appearance in the fundus of patients with XLRS. Retinal honeycomb appearance is defined as an irregularly excavated pockmarked appearance on the whitish retina [11], and was found in the wide-field fundus photo of 38 patients (48.7%), and 60 eyes (39.2%). OCT showed an extremely thin inner layer and an irregulated excavated outer layer. The Optomap ultra-wide-field fundus image is captured with two laser wavelengths: red channel at 633 nm and green channel at 532 nm that scan the retina simultaneously. The red channel permits a view of deeper retinal structures [16]. In our cohort, the honeycomb appearance could be seen in both the red and green channels, indicating the excavation could be in a rather deep level of the retina. The quick acquisition and wide-field nature of the Optomap fundus imaging system make it possible to get a more comprehensive view of the peripheral fundus of younger patients, which otherwise would be impossible without proper anesthesia. The fact that, in our cohort, most of the outpatient records failed to include a description of the honeycomb appearance, even when the appearance was rather obvious on the wide-field images, may explain the reason why this appearance may be underestimated in our clinical practice. Also, a lack of recognition of this unique appearance may contribute to this discrepancy. We usually concentrated more on the severity of the retinoschisis and whether there was RD or retinal breaks in the fundus examination before. With the recognition of this unique appearance on wide-field imaging and specific attention, we could easily find this appearance in the subsequent fundus examination.
The previous report regarding the honeycomb appearance is rare. But similar appearance has been reported in studies of degenerative retinoschisis. Mohite et al. report a bullous degenerative retinoschisis with a typical honeycomb appearance [10]. In a study based on 2319 eyes obtained in autopsy and 50 eyes with degenerative peripheral retinoschisis that were clinically examined, degenerative retinoschisis can be classified as typical or reticular. Typical retinoschisis presents a deeper splitting level, usually in the outer plexiform and inner nuclear layers, and is more likely to present in the pre-equatorial retina and does not usually extend into the posterior retina. It is rarely associated with laminar retinal breaks and retinal detachment. Reticular retinoschisis, a more severe type, has a more superficial splitting level, usually between the inner limiting membrane to the inner plexiform layer. Reticular retinoschisis has a predilection for the inferior temporal quadrant and is round or ovoid with a bullous elevation of the extremely thin inner layer and an irregular excavated outer layer thus presenting a honeycomb appearance. Reticular retinoschisis often extends into the posterior retina and is frequently associated with outer layer breaks (23–25%) and is more likely to be complicated with a retinal detachment (up to 22%) [11, 12].
In our cohort, the honeycomb appearance exhibited similar clinical characteristics to the reticular retinoschisis. All the honeycomb appearances were found within the area of retinoschisis. The splitting level was also superficial and showed excavated outer layer in the OCT, in accordance with the pathological change of the reticular retinoschisis. Previous histopathological studies of XLRS show that peripheral schisis occurs mainly in the superficial layers, such as the nerve fiber layer and ganglion cell layer [17,18,19]. OCT-based studies show that schisis can present in various layers, with different regional distributions [20,21,22]. Jia Yu et al. report that schisis of the inner nuclear layer, outer nuclear layer, and outer plexiform layer almost always involves the foveal center, but the schisis of the retinal nerve fiber layer is seen only in the parafoveal area [23]. Han et al. report the schisis of the ganglion cell layer to be perifoveal and the schisis of the outer nuclear layer to be mostly extramacular [20]. However, little is known regarding the schisis distribution in the far periphery region. The difference in the regional distribution of schisis may be explained by the difference in the retina structure between the macular and the periphery. The density of nerve fibers entering the nerve fiber layer is greater in the posterior pole, thus a stronger force, or disease at a more advanced stage, may be required to separate the ganglion cell layer from the retinal nerve fiber layer in this area to create schisis [23].
Regarding complications, we report here that the honeycomb appearance was significantly associated with peripheral retinoschisis, inner and outer layer breaks, RD and RRD. The relatively thin inner layer may make itself more vulnerable and susceptible to an inner layer break. In our cohort, there was a patient who demonstrated a typical honeycomb appearance and inner retinal break at the same time. Despite a prophylactic laser photocoagulation treatment, the affected eye still suffered an RRD during follow-up. We propose that honeycomb appearance may be a precursor of an outer layer break, considering with the progression of the disease, the excavation in the outer layer may coalesce into a full-thickness break, that is, an outer layer break. Concurrent outer and inner layer breaks are risk factors for RRD. And this may explain the higher incidence of outer retinal break and RRD in eyes with a honeycomb appearance. Hence, eyes with this specific appearance warrant closer follow-up and maybe more proactive prophylactic treatment. However, more cases and longer follow-ups are needed to investigate the natural course of the eyes with a honeycomb appearance and inner retinal breaks at the same time and to evaluate the safety and effectiveness of prophylactic laser treatment or any other possible treatment.
We acknowledge several limitations to this study. The retrospective nature of the design lacks a longitudinal follow-up to further investigate the change of the honeycomb appearance. Due to the relatively young age and the subsequent lack of cooperation of this cohort, a satisfying acquisition of the peripheral fundus image and OCT scans was difficult. Most of the OCT scans were of the macular area. Further OCT-based study regarding the periphery area of XLRS, especially the area with a honeycomb appearance is warranted, to provide more insight into this appearance. Also, the number of patients with genetic data in our cohort is too small to be analyzed. A genotype-phenotype correlation study in the future would give further insights into the disease pathology and this retinal appearance.





留言 (0)