
記住我










Endometrial cancer is the most common gynecologic cancer. In the US, approximately 66 570 new cases of uterine cancer and 12 940 uterine cancer related deaths will be reported for 2021.1 Even though the majority of these patients are diagnosed with an early stage localized disease and tend to have excellent survival (5 year survival 95%), those with metastatic or recurrent disease tend to have a lower response to therapy and a poor prognosis. Patients diagnosed with metastatic disease have a lower survival (5 year survival 16%), higher risk of recurrence, and tend to have recurrence at extra-pelvic sites. The 5 year survival for patients with pelvic recurrent disease is 55% but decreases to 17% in those with extra-pelvic recurrent disease.2 The outcome of those with extra-pelvic recurrent disease is dependent on disease distribution, molecular subtype, age, performance status, previous therapy, and time since previous therapy.
The current standard of care for systemic therapy in recurrent and metastatic settings includes chemotherapy with carboplatin/paclitaxel in the first line setting and pembrolizumab with or without lenvatinib or hormonal therapy in the second line setting. The role of immunotherapy with immune checkpoint inhibition has evolved in endometrial cancer based on the status of the mismatch repair system (Figure 1).
 Figure 1
Figure 1 Treatment landscape in endometrial cancer. *Advanced stage/metastatic endometrial cancer or serous histology. #Pembrolizumab+lenvatinib. §Ongoing research. Anti-PD1, anti-programmed cell death protein 1; EC, endometrial cancer; FDA, Food and Drug Administration; IHC, immunohistochemistry; MSI-H, microsatellite instability-high; MSS, microsatellite stable; PCR, polymerase chain reaction; RT, radiation.
Recently, the molecular classification of endometrial cancer based on data from The Cancer Genome Atlas (TCGA) has played a significant role in identifying prognostic and predictive factors which is currently shaping the selection of appropriate therapy as well as the design of future therapeutic agents. Endometrial cancer is divided into four molecular subtypes: (1) POLE mutated (5–7%), (2) microsatellite unstable (microsatellite instability-high)/deficient mismatch repair endometrial cancer (25–30%), (3) high copy number endometrial cancer (20–25%), and (4) low copy number endometrial cancer (~40%).3 High copy number endometrial cancer is usually an aggressive subtype (serous and 25% of grade 3 endometrioid endometrial cancer), and is driven by P53 mutations and a high frequency of amplification of oncogenes, such as ERBB2, CCNE1, and MYC. Low copy number endometrial cancer is usually an endometrioid subtype, hormonally driven, and characterized by a high rate of PTEN loss, phosphatidylinositol-3 kinase (PI3K) alteration, and positive estrogen receptor expression.3 Immunotherapy with immune checkpoint inhibitors demonstrated distinct antitumor activities as monotherapy or in combination for the different subgroups of endometrial cancer.
Immunotherapy in Endometrial Cancer with Microsatellite High/Deficient Mismatch Repair SystemApproximately 17–36% of patients with endometrial cancer are characterized by a defect in the mismatch repair system (deficient mismatch repair).4–6 In the NRG Oncology/Gynecologic Oncology Group (GOG) study and among 1024 patients with endometrial cancer, 26% were classified as epigenetic mismatch repair defective (microsatellite instability-positive with MLH1 methylation) and 10% as probable genetic mismatch repair mutation (microsatellite instability-positive and/or immunohistochemistry defect with absence of MLH1 methylation).4 In this study, microsatellite instability testing was done using the five-plex assay and was confirmed with polymerase chain reaction if microsatellite instability was tested with a single marker. Tumors were considered microsatellite instability-high if microsatellite instability was found at two or more markers. MLH1 methylation testing was done using pyrosequencing or combined bisulfite restriction analysis, or both. Using data from the GOG 86P study, immunohistochemical analysis of MSH6 and PMS2 on representative sections of the tumor of patients was used for microsatellite instability testing and a diagnosis of mismatch repair deficiency was inferred from loss of either MSH6 or PMS2. Among the entire cohort, 24% of patients were reported as having a deficient mismatch repair system.5 Similarly, in another study of 466 patients with endometrial cancer, 20% were classified as epigenetic mismatch repair defective and 5% as probably mismatch repair mutation.6 Overall survival outcome was similar to those with proficient mismatch repair.4 5
In contrast, patients with an epigenetic mismatch repair defect are more likely to have advanced stage, high grade disease and positive lymphovascular space invasion compared with those with a proficient mismatch repair system.6 These patients with an epigenetic mismatch repair defect tend to have lower progression free survival and a higher recurrence rate in advanced stage disease settings despite receiving similar adjuvant therapy.6 Among stage III/IV disease, the rate of recurrence was higher in patients with an epigenetic mismatch repair defect compared with those with stage III/IV disease with a proficient mismatch repair system (48% vs 3.4%).6 Adjuvant therapy was not different between the two groups. On the other hand, no difference was found in the rate of recurrence in early stage settings.
These patients are particularly sensitive to immunotherapy due to the increased rate of somatic mutation leading to high neo-antigenic load.7 8 Recently pembrolizumab was approved by the Food and Drug Administration (FDA) to treat patients with recurrent cancer with deficient mismatch repair status who progressed on standard therapy (Figure 2). In the phase II trial, the response rate among the non-colorectal patients with deficient mismatch repair was about 40%.6 Median progression free survival was not reached in the study. In the subset of patients with microsatellite instability-high endometrial cancer, the objective response rate was 57%, median progression free survival was 27 months, and overall survival was not reached.7 Similarly, another anti-programmed cell death protein 1 (anti-PD1) monoclonal antibody, dostarlimab, was studied in patients with microsatellite instability-high endometrial cancer. The objective response rate was 42%.9 Responses were durable and median duration of response was not reached. These data led to approval of dostarlimab in patients with recurrent endometrial cancer with deficient mismatch repair status (Figure 2).
Similarly, anti-PDL1 (programed death ligand 1) therapy with avelumab or durvalumab showed higher efficacy in endometrial cancer patients with deficient mismatch repair status (Table 1). In the meta-analysis by Yarchoan et al, the response rate to immunotherapy with PD1/L1 inhibitors was highest in patients with deficient mismatch repair tumors compared with the other approved indications, including melanoma and lung cancer.10 These promising results were noted in patients in recurrent settings after previous lines of therapy. This approach can be durable with limited toxicities.
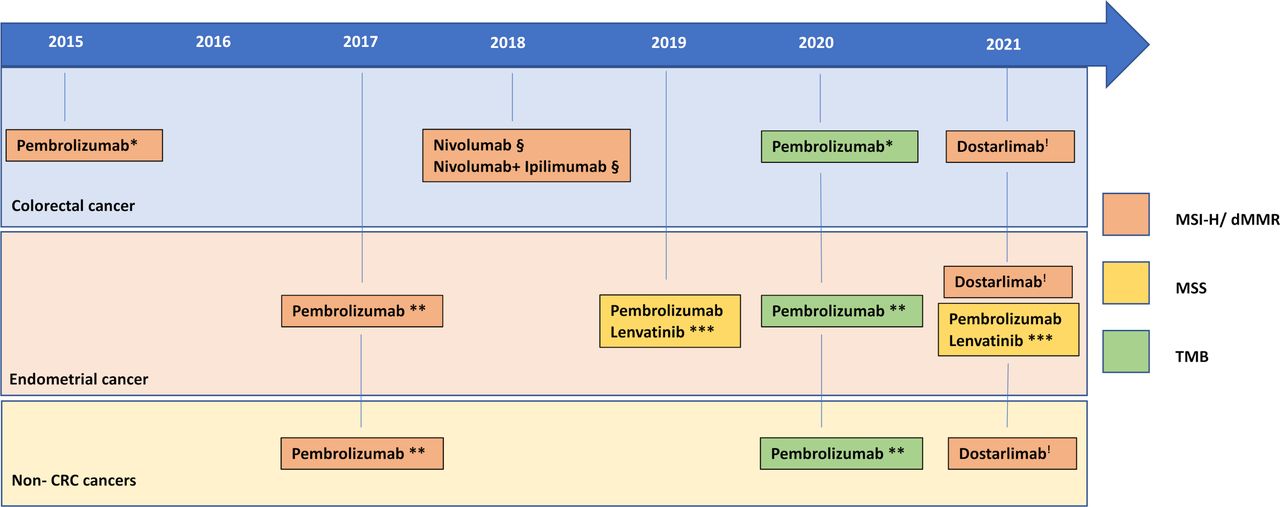 Figure 2
Figure 2 Food and Drug Administration approvals summary for immune checkpoint inhibitors based on microsatellite instability and tumor mutational burden status in solid tumors. *KEYNOTE-16; **KEYNOTE-158; ***KEYNOTE-146 and KEYNOTE-775; §CheckMate142; !Garnet. CRC, colorectal cancer; dMMR, deficient mismatch repair; MSI-H, microsatellite instability-high; MSS, microsatellite stable; TMB, tumor mutational burden.
Table 1Immunotherapy trials. Phase I/II in recurrent endometrial cancer by microsatellite instability/mismatch repair status
Future Strategies for Immunotherapy in Endometrial Cancer with Microsatellite High or Deficient Mismatch Repair SystemThese data support the promising role of immunotherapy in microsatellite instability-high/deficient mismatch repair endometrial cancer. Given that these are highly immunogenic tumors, we need to identify strategies to move immunotherapy to the first line setting and to reverse resistance among those who progress on anti-PD1 immunotherapy.
First Line Anti-PD1/PDL1 ImmunotherapyGiven the promising efficacy of anti-PD1 immunotherapy in recurrent settings, it would be ideal for immunotherapy with anti-PD1/PDL1 to be used in the first line setting. The most pressing question is whether immunotherapy is adequate as monotherapy, or do we still need to combine it with chemotherapy? Data from microsatellite instability-high colorectal cancer are encouraging and support the potential role of immunotherapy as monotherapy in the first line setting. In the KEYNOTE-177 trial, the efficacy of first line anti-PD1 therapy with pembrolizumab was compared with chemotherapy in advanced or metastatic microsatellite instability-high colorectal cancer. The results showed that pembrolizumab outperformed chemotherapy with significant improvement in progression free survival (16.5 vs 8.2 months, hazard ratio (HR) 0.6, p=0.0002) and a trend toward improved overall survival (not reached vs 37 months, HR 0.77, p=0.069) despite 59% crossover. Currently there is an ongoing phase III trial comparing the efficacy of pembrolizumab versus standard of care combination chemotherapy (carboplatin and paclitaxel) in the first line setting in patients with advanced or metastatic microsatellite instability-high endometrial cancer (KEYNOTE-C93/GOG-3064/ENGOT-en15; NCT05173987).
Other phase III trials have either completed or are ongoing and looking at incorporation of anti-PD1 or anti-PDL1 immunotherapy compared with chemotherapy in the first line setting in advanced stage or metastatic microsatellite instability-high endometrial cancer (Table 2). The main issue and remaining question that will not be answered by these trials is whether immunotherapy alone or combined with chemotherapy is better.
Table 2Immunotherapy trials in first line metastatic or recurrent endometrial cancer
The role of immunotherapy in early stage microsatellite instability-high colorectal cancer was studied in the neoadjuvant setting with promising results, with a high rate of complete pathologic response reaching 60–100%.11 12 Therefore, it will be important to assess the efficacy of anti-PD1 immunotherapy in the early stage setting as primary therapy (in young patients who are interested in fertility preservation or those who are poor candidate for surgery) or in the adjuvant setting. Currently, there is a large ongoing trial assessing the efficacy of adjuvant pembrolizumab in combination with chemotherapy with or without radiation compared with chemotherapy with or without radiation alone in patients with high risk endometrial cancer (NCT04634877). Further, there is an ongoing phase III trial assessing the efficacy of adding pembrolizumab and radiation compared with adjuvant radiation alone as adjuvant therapy in early stage microsatellite instability-high endometrial cancer meeting high–intermediate risk criteria (NCT04214067) (Table 2).
Combination ImmunotherapyIt is critically important to identify future immunotherapy options post progression on anti-PD1/PDL1 therapy. One approach is to co-target other immune checkpoints to synergize with anti-PD1/PDL1 therapy. Previous studies have shown that other T cell immune checkpoints tend to be upregulated in these patients, such as CTLA4 (cytotoxic T lymphocyte associated protein 4), LAG3 (lymphocyte activation gene 3), and TIGIT (T cell immunoreceptor with Ig and ITIM domains), and these represent an attractive approach. Further targeting tumor associated immunosuppressive myeloid cells and/or angiogenesis are other potential strategies.
Targeting Tumor Associated Myeloid Cells and Antiangiogenesis TherapyData suggest that microsatellite instability-high and POLE mutated endometrial cancers are characterized by high infiltration of CD3+ and CD8+ tumor infiltrating lymphocytes with increased PD1 expression (81% vs 28%) compared with microsatellite stable endometrial cancer. On the other hand, PDL1 expression was infrequent in tumor cells but was more frequent in intraepithelial immune cells (39% vs 13%). PD-L1 expression (presence vs total absence) in intraepithelial immune cells was significantly more frequent in POLE and microsatellite instability compared with microsatellite stable tumors (p=0.02). PD-L1 expression in at least 10% of peritumoral immune cells was also more frequent in POLE and microsatellite instability endometrial cancers than microsatellite stable endometrial cancers (p=0.03). PD-L1 expression in tumor cells was not different between POLE and microsatellite instability and microsatellite stable tumors.13 In another study, microsatellite instability-high endometrial cancers were noted to have increased immune cells in stroma, including granzyme B+ cells, activated cytotoxic T lymphocytes (CD8+ granzyme B+), and PD-L1+ cells. Granzyme B+ cells and activated cytotoxic T lymphocytes were also increased in the tumor compartment of microsatellite instability-high endometrial cancers. However, sporadic microsatellite instability-high endometrial cancers were characterized by increased PDL1+ macrophages in stroma and tumors compared with Lynch syndrome microsatellite instability-high endometrial cancer.14
Further, previous data have shown that antiangiogenic therapy leads to decreased immune inhibitory cells, such as T regulatory cells (also upregulated in microsatellite instability-high endometrial cancers) and myeloid derived myeloid suppressive cells, increased CD4+ and CD8+ cells, and decreased PD-1 expression.15–17 Therefore, it would be interesting to assess the combination of immunotherapy with antiangiogenic therapy or therapy targeting immunosuppressive myeloid cells in this patient population, especially post progression on anti-PD1/PDL1 therapy.
Co-targeting Dual Immune Checkpoints: PD1 with Other Immune Checkpoints, such as CTLA4 and LAG3CTLA4 targeted therapy is relevant in microsatellite instability-high endometrial cancer not only because its function as an immune checkpoint but also because it targets T regulatory cells which are immunosuppressive cells. High CTLA4 expression in T cells is found in microsatellite instability-high endometrial cancer and is significantly higher than in microsatellite stable endometrial cancer. Further, T regulatory cells have been shown to be more prominent in tumor immune microenvironments of microsatellite instability-high endometrial cancer compared with microsatellite stable endometrial cancer.18 19 These data support the role of anti-CTLA4 therapy in combination with anti-PD1 therapy.
Combined immunotherapy with PD1 and CTLA4 inhibitors act synergistically to promote T cell antitumor action through complimentary mechanisms of action and modulate other immunosuppressive immune cells.20 This in turn shifts the tumor microenvironment from a suppressive to an inflammatory environment. In metastatic colon cancer with a deficient mismatch repair system (CheckMate-142), the response rate to nivolumab was 31% and the median duration of response was not reached.21 However, in another study, the efficacy of combined therapy with nivolumab and ipilimumab in patients with metastatic colorectal cancer with deficient mismatch repair had a response rate of 55% and disease control of 80%. Median duration of response was not reached.22 These data support synergistic activity between PD1/PDL1 and CTLA4 inhibitors with promising durable results. This regimen was safe with rate of adverse events comparable with nivolumab monotherapy. The rate of grade 3 or 4 adverse events was 32%. The most common grade 3 and 4 adverse events were increased ALT/AST (15%), diarrhea (2%), fatigue (2%), pruritus (2%) and rash (2%), nausea (1%), and hypothyroidism (1%). Diarrhea was mostly grade 1–2 (20%) and so was hypothyroidism (13%). The rate of discontinuation due to adverse events related to the treatment was comparable between monotherapy and combination therapy (13 vs 7%).21 22 This has led to FDA approval of combined nivolumab and ipilimumab in patients with metastatic colorectal cancer with deficient mismatch repair (Figure 2). In another study, the efficacy of nivolumab 3 mg/kg every 2 weeks combined with lose dose ipilimumab 1 mg/kg every 6 weeks as first line therapy was investigated in metastatic microsatellite instability-high colorectal cancer. The authors reported an objective response rate of 69% and clinical benefit rate of 84%. The median duration of response and progression free or overall survival were not reached.23 Currently, a randomized phase II trial (NRG-GY-025) is ongoing comparing nivolumab with low dose ipilimumab versus nivolumab alone in recurrent microsatellite instability-high endometrial cancer (NCT05112601) (Table 2).
LAG3 is another immune checkpoint located on the surface of tumor infiltrating lymphocytes, including activated CD4, CD8, and T regulatory cells. It is also expressed on natural killer cells, B cells, and dendritic cells.24 LAG3 belongs to the immunoglobulin superfamily and associates with the CD3 (cluster of differentiation 3)/T cell receptor complex. LAG3 and PD1 are co-expressed both spatially and temporally in activated T cells and share partially overlapping cell surfaces and intracellular locations and trafficking pathways.25–27 LAG3 interacts with PD1 during CD8 cell signaling and recruits SHIP 1 and 2 to attenuate CD8 cell signaling and exert their negative regulatory role. LAG-3 interacts with major histocompatibility complex II to prohibit the binding of the same major histocompatibility complex molecule to T cell receptor and CD4, thus directly hindering T cell receptor signaling in the immune response.25–27 Crosslinking of LAG-3 and CD3 can impair T cell proliferation and cytokine secretion by inhibiting calcium ion fluxes. Co-localization of LAG3 and PD1 at antigen presenting cells and T cells support interaction between LAG3/major histocompatibility complex II and PD1/PDL1 to exert their effect on the T cell receptor/CD3 complex with independent negative signaling.25–27 Therefore, simultaneous blockade of LAG-3 and PD-1 may synergistically restore T cell activation and enhance antitumor immunity.
LAG3 has been reported to be upregulated in microsatellite instability-high cancers, including microsatellite instability-high endometrial cancers. In one study, LAG3 and TIGIT immune checkpoints were significantly elevated and highly expressed in POLE and microsatellite instability-high endometrial cancers compared with microsatellite stable endometrial cancers.18 Similarly, LAG3 has been reported to be upregulated in microsatellite instability-high colorectal cancer.19 28 In one study,19 PDL1 and LAG3 expression within tumor infiltrating immune cells was reported in 69% and 13%, respectively, while PDL1 and LAG3 expression within tumor cells were reported in only 25% and 5%, respectively.28 LAG3 immune checkpoint inhibitor (relatlimab) was investigated in combination with nivolumab in patients with advanced untreated melanoma in the first line setting. Combined nivolumab and relatlimab provided superior outcome compared with nivolumab alone with a well tolerated safety profile.29 Therefore, it will be interesting to assess the efficacy of combined dual PD1 and LAG3 blockade in microsatellite instability-high endometrial cancer both in PD1 naïve and PD1 treated settings.
Immunotherapy in Endometrial Cancer with Microsatellite Stable or Proficient Mismatch Repair SystemDespite 30% of endometrial cancer cases presenting with the microsatellite instability-high phenotype, which represents the highest frequency among all cancer subtypes, the other 70% of endometrial cancers are microsatellite stable and have limited treatment options in the recurrent setting.30 In those with a proficient mismatch repair system, the response rate to immune checkpoint inhibitors is low. In the KEYNOTE-028 trial, 24 patients with recurrent endometrial cancer who received at least two previous lines of chemotherapy with PDL1+ expression were treated with pembrolizumab. Most of these patients were mismatch repair protein proficient. The response rate was 13% and stable disease was seen in 13%.31
Given the potential role of antiangiogenesis therapy in modulating the tumor immune microenvironment and synergizing with anti-PD1 immunotherapy, as described earlier, the combination of anti-PD1 immunotherapy with antiangiogenesis is an attractive approach in microsatellite stable endometrial cancer.
Taken together, this led to the initiation of a phase 2 KEYNOTE-146 multicenter, open label, single arm study that investigated the combination of pembrolizumab with lenvatinib, a multikinase inhibitor against vascular endothelial growth factor receptors 1, 2, and 3 in patients with advanced endometrial cancer, irrespective of microsatellite instability status.32 Preliminary overall response rate (ORR) analysis of 54 patients after a median follow-up of 13.3 months demonstrated a HR of 39.6% (95% confidence interval 26.5 to 54.0). These findings supported an accelerated FDA approval of immunotherapy (IO) in combination with lenvatinib in patients with mismatch repair non-deficient endometrial cancer (Table 1). Recently, a confirmatory phase III of the KEYNOTE-775 trial was reported. The study included 827 patients with advanced metastatic or recurrent endometrial cancer after progression on one previous platinum based regimen. The study showed that pembrolizumab/lenvatinib significantly improved overall survival, progression free survival, and objective response compared with single agent chemotherapy (physician choice of doxorubicin or weekly paclitaxel). Median progression free survival was 7.2 months versus 3.8 months (HR 0.56, p<0.0001) and median overall survival was 18.3 versus 11.4 months (HR 0.63, p<0.0001). The objective response rate was 31.9% with pembrolizumab/lenvatinib compared with 14.7% with physician choice chemotherapy33 (Table 1). Adverse events of >grade 3 were reported in 88.9% of patients who received lenvatinib plus pembrolizumab and in 72.7% of those who received chemotherapy. Based on these data, the FDA granted regular approval for pembrolizumab with lenvatinib for patients with advanced endometrial carcinoma that is not microsatellite instability-high or mismatch repair deficient who have disease progression following previous systemic therapy in any setting and are not candidates for curative surgery or radiation (Figure 2). Other studies investigated the role of immunotherapy with anti-PD1/PDL1 therapy in microsatellite stable endometrial cancer with low efficacy (Table 1).
Given the significant toxicities and high discontinuation rate of lenvatinib when combined with pembrolizumab, it will be interesting to see if a combination of anti-PD1/PDL1 therapy with the anti-vascular endothelial growth factor monoclonal antibody, bevacizumab, will provide comparable efficacy but with a better safety and toxicity profile. Recently, Fuh et al presented the results of their phase II trial investigating the efficacy of the anti-PDL1, atezolizumab, combined with bevacizumab in 57 patients with recurrent endometrial cancer at the International Gynecologic Cancer Society Meeting, 2022. The author reported an objective response rate of 33%, median duration of response of 15 months, and median progression free survival of 7.8 months in patients with mismatch repair proficient recurrent endometrial cancer.34 These data are attractive and need to be validated in a larger phase III trial.
Future strategies for Immunotherapy in Endometrial Cancer with Microsatellite Stable or Proficient Mismatch Repair SystemFirst line Anti-PD1/PDL1 Therapy in Combination With Chemotherapy Followed by Anti-PD1/PDL1 Maintenance With or Without Poly ADP Ribose Polymerase InhibitionSimilar to microsatellite instability-high endometrial cancer, phase III trials are being conducted to assess the efficacy of anti-PD1/PDL1 in combination with chemotherapy followed by maintenance anti-PD1/PDL1 therapy. Interestingly, in two trials (GOG-3031/RUBY, NCT03981796 and GOG3041/DUO-E, NCT04269200), patients were randomized to receive either maintenance therapy with anti-PD1/PDL1 alone or in combination with poly ADP ribose polymerase inhibition. These trials will provide important information on the role of immunotherapy in the first line setting and whether adding maintenance poly ADP ribose polymerase inhibition (niraparib or olaparib) will provide an additional benefit. A press release about the RUBY trial announced that it achieved its primary endpoint, but further details are yet to be disclosed.
Recently, a single arm phase II trial investigating the efficacy of rucaparib with atezolizumab and bevacizumab in 30 patients with recurrent endometrial cancer was presented at ASCO 2022. The authors reported an objective response rate of 43% and median even free survival of 5.3 months and overall survival of 13.3 months35
Combination of Anti-PD1/L1 With Other Agents in Molecularly Driven Approach (EndoMAP)Another interesting study that is currently ongoing is the EndoMAP trial. This trial is investigating the efficacy of the anti-PDL1, atezolizumab, in combination with another targeted therapy based on the molecular profile of endometrial cancer, such as a combination with the poly ADP ribose polymerase inhibitor, talazoparib, in those with a homologous recombination deficient tumor, or a combination with ipatasertib or T-DM1 (ado-trastuzumab emtansine) in those with alteration in the PI3K pathway or HER2 amplification, respectively (NCT04486352). This trial raises the question of the potential role of molecularly targeted therapy as a strategy to enhance the response to anti-PD1/PDL1 immunotherapy in recurrent endometrial cancer.
ConclusionImmunotherapy in endometrial cancer is evolving and different novel combination approaches are being investigated. It is important to categorize endometrial cancer into two immunologically different subtypes: microsatellite instability-high and microsatellite stable endometrial cancer. Future design and therapeutic approaches should take the immunologically different subtypes into account.
Ethics statementsPatient consent for publicationEthics approvalNot applicable.
留言 (0)