
記住我


Antiretroviral therapy has played an important role in reducing mortality, morbidity, and transmission rates for HIV.1,2 However, new HIV infections continue to be prevalent, especially in specific regions of the world, with up to 1.5 million new HIV-1 infections estimated worldwide each year.2,3 Pre-exposure prophylaxis (PrEP) has proven to be effective in reducing transmission among individuals at risk of acquiring HIV.4–6 Daily oral antiretroviral drugs are currently the main method for HIV-1 PrEP, but the effectiveness of PrEP can be variable given the challenges associated with maintaining strict adherence to a daily oral dosing schedule.7–10 In people at high risk of HIV infection, PrEP delivered using a long-acting implant has been identified as a preferred potential method of treatment compared with daily oral PrEP, particularly if a long dosing interval for an implant can be achieved.11–13 Therefore, novel PrEP strategies that use a subdermal implant may improve outcomes for people at risk of acquiring HIV.
Islatravir is a deoxyadenosine analog that is converted intracellularly into its active form, islatravir triphosphate, where it suppresses HIV-1 replication through inhibition of reverse transcriptase.14,15 Islatravir demonstrated high potency in preclinical studies and in trials in adults with HIV infection.16–18 Evaluation of more recent findings suggests decreases in total lymphocyte and CD4+ T-cell counts in some participants who received islatravir in clinical studies,19 but it is not known whether this is a potential complication after implant placement. Because of its high potency, islatravir is a candidate drug for PrEP administered using a subdermal implant with a potential for long-lasting delivery.
Based on preclinical and clinical data demonstrating effective lowering of viral load, an intracellular islatravir triphosphate concentration of 0.05 pmol/106 cells, which is approximately 5 times the in vitro concentration required to inhibit 50% of the replication activity (IC50) of wild-type HIV-1, was established as a target threshold for PrEP.14 An initial placebo-controlled, double-blind, phase 1 clinical trial of islatravir delivered using a prototype polymer implant (54 mg and 62 mg) over 12 weeks in adult participants at low risk of acquiring HIV offered encouraging results.20 This prototype implant was generally well tolerated at both dose levels (n = 16; 6 active and 2 placebo per panel); no systemic events were reported and no deaths, serious adverse events (AEs), or discontinuations due to an AE occurred throughout the 12-week study.20 Through 12 weeks in both the islatravir 54 mg and the 62-mg implant cohorts, mean islatravir triphosphate concentrations were above the prespecified pharmacokinetic (PK) threshold of 0.05 pmol/106 peripheral blood mononuclear cells (PBMCs).20 These promising results led to the development of a next-generation radiopaque islatravir-eluting implant.
A study was conducted to investigate the safety, tolerability, and PK of intracellular islatravir triphosphate and plasma islatravir in next-generation radiopaque subdermal islatravir-eluting implants.
METHODSThis study was a randomized, double-blind, placebo-controlled, phase 1 trial (protocol MK-8591-008). This study was performed in accordance with the International Conference on Harmonization Good Clinical Practice guidelines and the principles of the Declaration of Helsinki. The protocol and relevant study materials were reviewed and approved by Advarra, Inc., (Columbia, MD) and the ethics review committee of Ghent University Hospital (Ghent, Belgium). All participants signed informed consent documents before enrollment. This study was registered on EudraCT (Study Identifier: 2019-002718-38). This study was conducted at 2 sites in 2 countries (Celerion, Lincoln, NE, and Drug Research Unit, Ghent, Belgium).
ParticipantsAdult healthy male and female participants at low risk of HIV-1 infection, aged 18–55 years, and with a body mass index 18–32 kg/m2 were eligible for enrollment. Participants had to be in general good health, per medical history and screening laboratory values, and were required to be HIV negative and at low risk of HIV infection based on standard criteria for PrEP. For women of childbearing potential, a negative pregnancy test was required within 24 hours before implant placement, and participants had to maintain an approved method of birth control. Participants were excluded if they had a history of a clinically significant disease or a known hypersensitivity or idiosyncratic reaction to the drugs used in this study. Participants with tattoos, scars, or other physical findings at the site of implant placement, a history of keloids, or a contraceptive subdermal implant in place also were excluded from this study.
Study DesignThis study consisted of 3 panels (A, B, and C) comprising 12 participants each; participants were randomized (2:1) within each panel to receive an islatravir-containing or placebo-containing implant according to a computer-generated allocation schedule. Participants were allocated evenly between the 2 sites so that, within each panel, exactly half of the participants on active and on placebo were at each site. Panel A participants received islatravir 48 mg or placebo implant, panel B participants received islatravir 52 mg or placebo implant, and panel C participants received islatravir 56 mg or placebo implant. All placebo participant data were pooled for analyses. The next-generation radiopaque 56-mg implant was formulated to release the drug at a rate similar to that of the 62-mg prototype implant assessed previously. Placebo implants were identical in appearance to the active implants. The implants were approximately 4 cm in length and 2 mm in diameter and were inserted subdermally on the inner aspect of the nondominant upper arm, overlying the triceps muscle approximately 8–10 cm (3–4 in) from the medial epicondyle of the humerus and 3–5 cm (1.25–2 in) posterior to the sulcus between the biceps and triceps muscles. Site personnel responsible for implant insertion and removal were experienced in implant placement and received refresher training before the study start.
Blood for PK assessment was collected, and safety was assessed throughout this study. Implants were removed 12 weeks after placement. A subset of participants had rectal or vaginal biopsies collected on day 85 or 12 weeks (after implant removal) for PK tissue assessment. Implant removal was assessed during this trial, including difficulty during removal and the presence of bent/broken implants.
Pharmacokinetics AnalysesBlood samples for plasma analyses were collected predose; at 0.5, 1, 2, 4, 8, and 12 hours after receiving the implant on day 1, on days 2, 3, 5, 8, 11, 15, 22, 29, 43, 57, 71, and 85 after implant placement, and after removal on days 92, 99, 106, and 113 (Fig. 1). Blood samples for PBMC analyses were collected at the same time points as plasma analyses except 0.5-h and 8-h samples were not collected on day 1, and blood samples were collected on day 141 (Fig. 1).
 FIGURE 1.:
FIGURE 1.: Study design. R, randomization.
PK parameters of interest included the following: intracellular concentrations of islatravir triphosphate in PBMCs and tissue on day 85 [C85d], maximum concentration (Cmax), time to maximum concentration (Tmax), and apparent terminal half-life (t½), as well as plasma islatravir Cmax, C85d, and Tmax. All parameters were calculated using noncompartmental methods using Phoenix WinNonlin, version 6.3 or higher (Certara, Princeton, NJ). Bioanalysis of islatravir in human plasma was conducted by protein precipitation followed by reversed-phase chromatographic separation coupled with tandem mass spectrometric detection. The lower limit of quantitation (LLOQ) was 0.1 ng/mL (0.000341 μM), with a linear calibration range from 0.1 ng/mL to 100 ng/mL (0.000341 μM–0.341 μM).
Islatravir triphosphate was analyzed in human PBMC lysate using protein precipitation, followed by ion exchange chromatography coupled with tandem mass spectrometry. The LLOQ was 0.1 ng/mL (0.000188 μM), with a linear calibration range from 0.1 ng/mL to 40 ng/mL (0.000188 μM–0.0752 μM). PBMC cell counts (per 106 cells) were estimated using a hemocytometer, and the conversion from μM to pmol/106 cells was made using the standard assumption that 1 PBMC has an approximate volume of 0.2 pL.20,21
Islatravir triphosphate of rectal and vaginal tissue samples was analyzed by protein precipitation of tissue homogenates, followed by ion exchange chromatography coupled with tandem mass spectrometry. Rectal and vaginal tissues were homogenized at a ratio of 1:19 (tissue: homogenization solvent). The LLOQ was 0.1 ng/mL (0.000188 μM), with a linear calibration range from 0.1 ng/mL to 40 ng/mL (0.000188 μM–0.0752 μM).
Safety AssessmentsSafety was assessed by clinical evaluation, including full physical examination, vital sign assessment, 12-lead electrocardiogram measurements, laboratory tests, and local inspection at the site of implant placement, at prespecified time points. Participants were also monitored for the emergence of AEs.
Statistical AnalysisThe primary hypothesis, that a true geometric mean (GM) intracellular islatravir triphosphate C85d >0.05 pmol/106 cells is maintained for up to 12 weeks at a dose level of an islatravir-eluting implant that is generally well tolerated, was tested using a linear fixed-effects model having dose as a fixed effect. Individual islatravir triphosphate C85d values were natural log transformed before analysis. A posterior distribution for the true GM intracellular islatravir triphosphate C85d on the log scale was generated for each dose level using flat priors. Using the posterior distributions for each dose level, the posterior probability that the true GM intracellular islatravir triphosphate C85d >0.05 pmol/106 cells was calculated for each dose. A 70% posterior probability for at least 1 dose level that is generally well tolerated for up to 12 weeks was considered to satisfy the primary PK hypothesis. Point estimates and 90% confidence intervals of islatravir triphosphate C85d GM are provided by dose. Safety data, including the incidence of AEs, are summarized descriptively. The intensity of each AE and SAE was assessed by the investigator according to the National Institutes of Health Division of AIDS criteria.22
The between-subject log-SDs for islatravir triphosphate PBMC C85d were estimated at 0.268 and 0.431 after administration of a single subdermal implant dose of 54 mg and 62 mg, respectively, based on the previous clinical trial.20 The pooled between-subject log-SD across 2 dose levels was estimated to be 0.359. Using this estimated SD and a posterior probability of 70%, at each dose level, with 8 participants in the islatravir treatment group, if the true mean islatravir triphosphate PBMC C85d is >0.06 pmol/106 cells, there would be at least an 80% probability that the hypothesis is supported that the islatravir implant exhibits a GM islatravir triphosphate PBMC C85d of >0.05 pmol/106 cells.
RESULTSIn total, 36 participants were enrolled, with a mean age of 36.0 years (range, 19–54 years). The study population was evenly balanced between male and female participants and was predominantly White (Table 1). All participants completed this study per protocol. The first participant was enrolled on July 9, 2020, and the last participant completed their last visit on December 14, 2020.
TABLE 1. - Baseline Characteristics Islatravir 48 mg Implant (n = 8) Islatravir 52 mg Implant (n = 8) Islatravir 56 mg Implant (n = 8) Total Islatravir Implant (n = 24) Placebo Implant (n = 12)* Age, mean (SD), years 37.6 (9.7) 34.9 (9.5) 35.4 (7.1) 36.0 (8.5) 36.0 (11.6) Male sex, n (%) 5 (62.5) 4 (50.0) 2 (25.0) 11 (45.8) 7 (58.3) BMI, mean (SD), kg/m2 27.4 (3.9) 25.2 (3.5) 24.8 (3.6) 25.8 (3.7) 25.1 (4.1) Race, n (%) White 8 (100) 7 (87.5) 8 (100) 23 (95.8) 11 (91.7) Black or African American 0 (0) 0 (0) 0 (0) 0 (0) 1 (8.3) American Indian or Alaska Native 0 (0) 1 (12.5) 0 (0) 1 (4.2) 0 (0)*Data pooled for 4 participants in each panel (12 participants total) who were administered the placebo implant. BMI, body mass index.
Islatravir implants were generally well tolerated. AEs were reported by 20 of 24 participants (83%) who received islatravir compared with 6 of 12 participants (50%) of who had received placebo (Table 2). The most common implant site AEs were induration, pain, pruritis, hematoma, and erythema. All implant site AEs were mild or moderate in intensity and resolved, or were resolving, by the last clinic visit. Moderate erythema was observed in 2 of 8 participants (25%) for islatravir 48 mg and 1 of 8 participants (13%) for islatravir 56 mg, and moderate pruritis was observed in 1 of 8 participants for islatravir 48 and 56 mg (13% for both). The incidence and severity of implant-related AEs were higher with the islatravir implant compared with placebo. Pain was the only implant AE that appeared to have a dose-dependent relationship (Table 2). Some AEs, particularly erythema and induration, persisted for several weeks in some participants (see Figure S1, Supplemental Digital Content, https://links.lww.com/QAI/B997). All implants were removed without complication, and all implants were removed intact.
TABLE 2. - Most Common AEs Observed in ≥2 Participants in at Least 1 Treatment Group n (%) Islatravir 48 mg Implant (n = 8) Islatravir 52 mg Implant (n = 8) Islatravir 56 mg Implant (n = 8) Total Islatravir Implant (n = 24) Placebo Implant (n = 12)* ≥1 AE 7 (87.5) 5 (62.5) 8 (100.0) 20 (83.3) 6 (50.0) General implant site AEs Erythema 4 (50.0) 2 (25.0) 4 (50.0) 10 (41.7) 3 (25.0) Hematoma 4 (50.0) 4 (50.0) 3 (37.5) 11 (45.8) 6 (50.0) Hemorrhage 1 (12.5) 0 3 (37.5) 4 (16.7) 0 Induration 4 (50.0) 4 (50.0) 4 (50.0) 12 (50.0) 2 (16.7) Pain 2 (25.0) 4 (50.0) 6 (75.0) 12 (50.0) 4 (33.3) Pruritus 5 (62.5) 2 (25.0) 5 (62.5) 12 (50.0) 3 (25.0) Swelling 2 (25.0) 0 1 (12.5) 3 (12.5) 1 (8.3) Nonimplant site AEs Headache 2 (25.0) 2 (25.0) 3 (37.5) 7 (29.2) 1 (8.3) Paresthesia 0 0 3 (37.5) 3 (12.5) 1 (8.3)*Data pooled for 4 participants in each panel (12 participants total) who were administered the placebo implant. AE, adverse event.
The most common nonimplant site AE was headache, which occurred in 8 participants (1/12 [8%] in placebo, 2/8 [25%] for islatravir 48 mg, 2/8 [25%] for islatravir 52 mg, and 3/8 [38%] for islatravir 56 mg). In addition, 4 participants (1/12 [8%] in placebo and 3/8 [38%] in islatravir 56 mg) reported paresthesia in the arm in which the implant had been placed, of short duration (up to 2 hours) or intermittently up to approximately 1 week; all resolved before implant removal. All nonimplant site AEs were mild or moderate intensity and resolved by study completion. No clinically meaningful relationships were observed for changes in clinical laboratory values, vital signs, or electrocardiogram safety parameter values as a function of treatment. No serious AEs were reported, and no participant discontinued the study because of an AE. There were no meaningful differences in total lymphocyte count between the different implant dose levels and placebo. CD4+ T cells were not collected in this study.
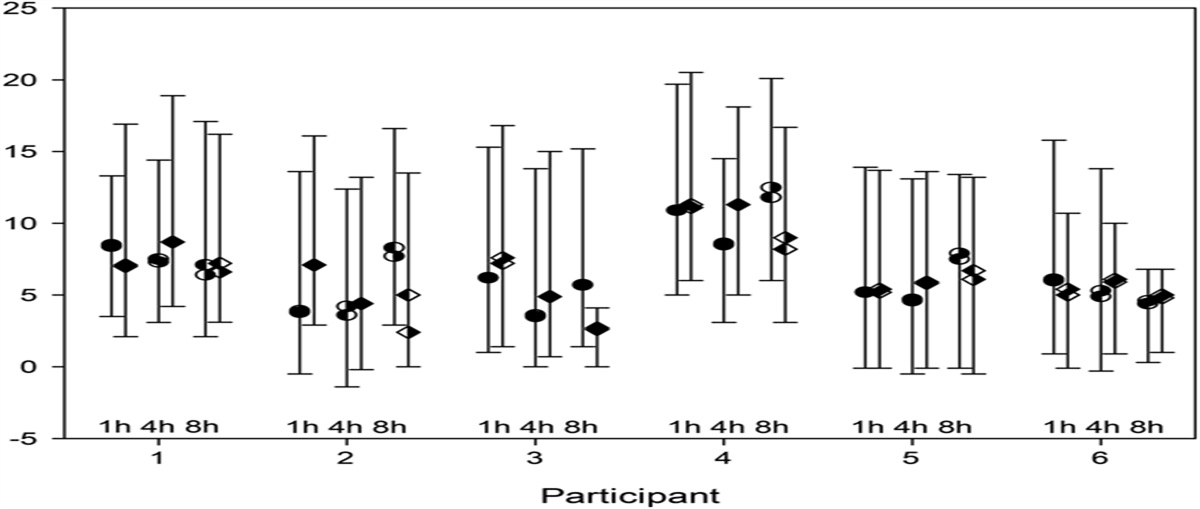
PharmacokineticsThe mean islatravir triphosphate concentrations in PBMCs remained above the prespecified PK threshold of >0.05 pmol/106 cells throughout the 12-week duration after placement of an islatravir-containing implant (48, 52, and 56 mg) (Fig. 2). Concentrations above 0.05 pmol/106 cells for all individuals were attained at 8 hours after implant placement and were maintained above this threshold at the 52-mg and 56-mg dose levels throughout the implant insertion period.
 FIGURE 2.:
FIGURE 2.: Arithmetic mean (range) concentration–time profiles for PBMC islatravir triphosphate in adult participants without HIV after placement of an islatravir-containing implant over 12 weeks and 4 weeks after implant removal. Horizontal dashed line corresponds to the threshold concentration of 0.05 pmol/106 PBMCs. Vertical dashed line corresponds to implant removal. PBMC, peripheral blood mononuclear cell.
PK results of islatravir triphosphate in PBMCs and islatravir in plasma are summarized in Table 3. Cmax in PBMCs was approximately 2.6 times higher for the islatravir 56 mg implant compared with the islatravir 48 mg implant (0.375 vs. 0.984 pmol/106 cells), and Tmax was substantially longer for the islatravir 56 mg implant (671.7 hours) relative to the islatravir 48 mg implant (95.1 hours). At day 85, GM concentrations were well above the 0.05 pmol/106 cells threshold in PBMCs (range, 0.101–0.561 pmol/106 cells) at all dose levels. The posterior probability of GM islatravir triphosphate concentrations being above the threshold of 0.05 pmol/106 cells at C85d was >0.99 for all panels. The GM apparent terminal half-life for islatravir triphosphate in PBMCs was 183–247 hours after implant removal.
TABLE 3. - PK of Islatravir Triphosphate in PBMCs and in Tissue Biopsies and PK of Islatravir in Plasma at 12 Weeks After Administration of an Islatravir Implant in Adults Without HIV GM (%GCV) Islatravir 48 mg Implant (n = 8) Islatravir 52 mg Implant (n = 8) Islatravir 56 mg Implant (n = 8) Islatravir triphosphate Cmax, pmol/106 PBMCs 0.375 (22.4) 0.519 (16.4) 0.984 (31.9) C85d, pmol/106 PBMCs 0.101 (31.9) 0.204 (54.3) 0.561 (55.7) Tmax, range, hours* 95.1 (48.0–166.9) 167.3 (48.2–670.5) 671.7 (166.9–2015.7) Apparent terminal t½, hours 183 (21.9)† 247 (19.0)‡ 190 (27.8) Vaginal biopsies, fmol/g NC§ (n = 1) NC§ (n = 2) 6220 (32.3) (n = 3) Rectal biopsies, fmol/g 1290 (173.2)|| (n = 3) 9700 (22.2) (n = 2) 12,400¶ (n = 1) Islatravir Cmax, µM 0.00447 (19.6) 0.00696 (119.9) 0.00645 (55.2) C85d, µM 0.000144 (13.4) 0.000327 (25.1) 0.000615 (11.5) Tmax, range, hours* 4.0 (4.0–8.0) 4.0 (2.0–4.1) 4.0 (2.0–4.3) C85d, µM 0.000144 (13.4) 0.000327 (25.1) 0.000615 (11.5)*Tmax is reported as median (minimum–maximum).
†n = 6; 2 participants had insufficient data at the terminal phase to estimate t½ after implant removal.
‡n = 5; 3 participants had insufficient data at the terminal phase to estimate t½ after implant removal.
§Participants had a week 12 value below the lower limit of quantitation.
||Values correspond to arithmetic mean (%CV) as few rectal biopsies had C85d values below the lower limit of quantitation. Hence, arithmetic mean (%CV) was reported because GM (%GCV) was not calculable.
¶%GCV value not reported because n < 2.
C85d, concentration at day 85; Cmax, maximum concentration; CV, coefficient of variation; GCV, geometric coefficient of variation; NC, not calculated; t½, half-life; Tmax, time to maximum concentration.
The number of participants who had rectal and vaginal biopsies performed was low. Data from the limited number of vaginal and rectal biopsies are summarized in Table 3.
DISCUSSIONPrEP has proven to be effective in reducing HIV transmission, and a long-acting PrEP option offers one method of overcoming some of the challenges associated with daily oral PrEP for people at risk of acquiring HIV-1. The long duration of activity and low maintenance characteristics of subdermal implants have been highlighted as key benefits for administering PrEP.23 Islatravir, a nucleoside reverse transcriptase translocation inhibitor, has demonstrated clinical efficacy in reducing HIV-1 viral load and is a candidate as an implant PrEP agent.18,20 A next-generation subdermal radiopaque implant containing islatravir was assessed in a safety and PK study, and PK data indicated that intracellular islatravir triphosphate concentrations in PBMCs, above a projected therapeutic threshold, were quickly reached and maintained for the entire duration of placement. The safety and tolerability profile of the islatravir implant was consistent with that expected from an implant and with the previously reported safety profile of islatravir, whether administered orally or as an implant.15,20
The outcomes observed in this study were consistent with an earlier investigation of a prototype polymer islatravir implant.20 A similar islatravir triphosphate t½ after removal was reported for the radiopaque implant versus the prototype implant, and this t½ was also similar to that after oral administration of islatravir.20,24 The delivery mechanism is not expected to affect islatravir triphosphate clearance, and there is no evidence of islatravir dose level affecting islatravir clearance.24,25 The next-generation radiopaque implant facilitates in situ localization of the implant through x-ray in addition to palpation or ultrasound, which is clearly advantageous during clinical assessment of implants that may have migrated.
The greater-than-dose-proportional changes in islatravir triphosphate Cmax, Tmax, and C85d with the implants with increasing dose are consistent with the expected properties of a subdermal implant, where changes in drug load modulate the drug-releasing properties of the implant.26 The Cmax and C85d for the 56-mg implant are approximately 2-fold to 6-fold higher than the 48-mg and 52-mg implants, likely because of the higher drug load and subsequent cumulative drug release profile. This projected increase in drug release is further reflected in the longer Tmax, with longer continuous release to reach Cmax.
The radiopaque implant seems to offer a similar safety profile as the prototype implant.20 The implant was generally well tolerated, and no serious AEs or discontinuations due to AEs were reported. Although the frequency, duration, and severity of AEs could possibly be dose-dependent, only the presence of pain and duration of some AEs seemed dose-related. Localized pain associated with implant insertion is a known and expected AE after subdermal implant insertion, and other AEs associated with implant insertion, such as moderate bruising, a small scar, and tenderness or bleeding after insertion or removal, may be considered acceptable by implant recipients.13 In addition, an implant of the size used in this study may not be considered bothersome by patients at risk of being infected with HIV-1.13 However, the small sample size in this study and the prototype implant study precludes conclusive analysis of any dose-dependent effect on AEs; additional studies in a larger population will be needed for appropriate assessment.
The key concern for individuals who use PrEP are cosmetic elements associated with an implant.11 For example, implants may be visible or readily felt under the skin.13 Conversely, these properties may offer a degree of security in confirming presence and evidence of adherence to PrEP.11,13 The ability to readily remove an implant offers an important safety advantage versus injectables in situations where drug removal is required.13
Attaining adequate tissue concentrations across plasma, PBMCs, and vaginal and rectal tissue is likely important for adequate prevention, but oral emtricitabine and tenofovir-based PrEP formulations can have inconsistent tissue concentrations yet are effective PrEP agents.27,28 The number of participants providing biopsies in this study was small, but rectal and vaginal islatravir triphosphate concentrations both were generally similar to those observed after oral dosing25; it seems likely that genital tissue distribution would be similar between oral and implant dosing. Further investigation of tissue concentrations is warranted, particularly in connection with efficacy measures.
A strength of this randomized, placebo-controlled trial is the inclusion of 3 different dosing arms with male and female participants and an increased number of participants in each panel compared with a previous islatravir implant trial. The current trial was conducted to assess implants for a 12-week interval, which provides more robust PK and safety data over a shorter duration (eg, 4-week duration). However, this study is also somewhat limited by this 12-week interval and the relatively small sample size; a larger, longer study is necessary to more fully address tolerability and safety, particularly with respect to lymphocyte count and to assess PK after longer-term implant placement. Given that adequate PK and safety have been demonstrated with the current implant, long-term studies will be necessary to demonstrate the safety and PK characteristics of this approach to offering PrEP over a full 12 months to confirm adequate drug concentrations and efficacy. Similarly, qualitative studies and investigations after repeated implantations may be required to further understand the efficacy, safety, and tolerability of PrEP administered using a subdermal implant.
CONCLUSIONSIn conclusion, islatravir administered using a subdermal implant has the potential to be an effective and well-tolerated method for administering PrEP to individuals at risk of acquiring HIV-1. Further investigation is warranted.
ACKNOWLEDGMENTSThe authors thank the participants and clinical research staff who participated in this study, Yang Liu, PhD, for excellent statistical support, and Robert Schwab, MD, for support with this manuscript. Medical writing and/or editorial assistance, under the direction of the authors, was provided by Andrea Humphries, PhD, and Jared Cochran, PhD, ApotheCom (USA), in accordance with Good Publication Practice (GPP3) guidelines. This assistance was funded by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ.
REFERENCES 1. Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. 2022. Available from: https://clinicalinfo.hiv.gov/sites/default/files/guidelines/documents/adult-adolescent-arv/guidelines-adult-adolescent-arv.pdf. Accessed September 27, 2022. 2. GBD 2017 HIV collaborators. Global, regional, and national incidence, prevalence, and mortality of HIV, 1980-2017, and forecasts to 2030, for 195 countries and territories: a systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV. 2019;6:e831-e859. 3. UNAIDS. Fact Sheet - Global HIV Statistics. 2022. Available from: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf. Accessed September 27, 2022. 4. Baeten JM, Donnell D, Ndase P, et al. Antiretroviral prophylaxis for HIV prevention in heterosexual men and women. N Engl J Med. 2012;367:399–410. 5. Grant RM, Lama JR, Anderson PL, et al. Preexposure chemoprophylaxis for HIV prevention in men who have sex with men. N Engl J Med. 2010;363:2587–2599. 6. Fonner VA, Dalglish SL, Kennedy CE, et al. Effectiveness and safety of oral HIV preexposure prophylaxis for all populations. AIDS. 2016;30:1973–1983. 7. Owens DK, Davidson KW, Krist AH, et al. Preexposure prophylaxis for the prevention of HIV infection: US Preventive Services Task Force recommendation statement. JAMA. 2019;321:2203–2213. 8. Marrazzo JM, Ramjee G, Richardson BA, et al. Tenofovir-based preexposure prophylaxis for HIV infection among African women. N Engl J Med. 2015;372:509–518. 9. Sahay S, Verma A, Shewale S, et al. Understanding issues around use of oral pre exposure prophylaxis among female sex workers in India. BMC Infect Dis. 2021;21:930. 10. Smith DK, Rawlings MK, Glick N, et al. Adherence to daily oral TDF/FTC for PrEP in community health center populations: the Sustainable Health Center Implementation PrEP Pilot (SHIPP) study. AIDS Behav. 2022;26:350–360. 11. Greene GJ, Swann G, Fought AJ, et al. Preferences for long-acting pre-exposure prophylaxis (PrEP), daily oral PrEP, or condoms for HIV prevention among U.S. men who have sex with men. AIDS Behav. 2017;21:1336–1349. 12. Minnis AM, Atujuna M, Browne EN, et al. Preferences for long-acting pre-exposure prophylaxis (PrEP) for HIV prevention among South African youth: results of a discrete choice experiment. J Int AIDS Soc. 2020;23:e25528. 13. Rael CT, Lentz C, Carballo-Diéguez A, et al. Understanding the acceptability of subdermal implants as a possible new HIV prevention method: multi-stage mixed methods study. J Med Internet Res. 2020;22:e16904. 14. Grobler JA, Fillgrove KL, Hazuda DJ, et al. MK-8591 potency and PK provide high inhibitory quotients at low doses QD and QW. Presented at: Conference on Retroviruses and Opportunistic Infections (CROI); Seattle, WA, USA; March 4–7, 2019. 15. Markowitz M, Sarafianos SG. 4'-Ethynyl-2-fluoro-2'-deoxyadenosine, MK-8591: a novel HIV-1 reverse transcriptase translocation inhibitor. Curr Opin HIV AIDS. 2018;13:294–299. 16. Stoddart CA, Galkina SA, Joshi P, et al. Oral administration of the nucleoside EFdA (4'-ethynyl-2-fluoro-2'-deoxyadenosine) provides rapid suppression of HIV viremia in humanized mice and favorable pharmacokinetic properties in mice and the rhesus macaque. Antimicrob Agents Chemother. 2015;59:4190–4198. 17. Markowitz M, Gettie A, St Bernard L, et al. Once-weekly oral dosing of MK-8591 protects male rhesus macaques from intrarectal challenge with SHIV109CP3. J Infect Dis. 2020;221:1398–1406. 18. Schurmann D, Rudd DJ, Zhang S, et al. Safety, pharmacokinetics, and antiretroviral activity of islatravir (ISL, MK-8591), a novel nucleoside reverse transcriptase translocation inhibitor, following single-dose administration to treatment-naive adults infected with HIV-1: an open-label, phase 1b, consecutive-panel trial. Lancet HIV. 2020;7:e164-e172. 19. Merck & Co., Inc. Merck Announces Clinical Holds on Studies Evaluating Islatravir for the Treatment and Prevention of HIV-1 Infection. 2021. Available from: https://www.merck.com/news/merck-announces-clinical-holds-on-studies-evaluating-islatravir-for-the-treatment-and-prevention-of-hiv-1-infection/. Accessed September 27, 2022. 20. Matthews RP, Patel M, Barrett SE, et al. Safety and pharmacokinetics of islatravir subdermal implant for HIV-1 pre-exposure prophylaxis: a randomized, placebo-controlled phase 1 trial. Nat Med. 2021;27:1712–1717. 21. Simiele M, D'Avolio A, Baietto L, et al. Evaluation of the mean corpuscular volume of peripheral blood mononuclear cells of HIV patients by a coulter counter to determine intracellular drug concentrations. Antimicrob Agents Chemother. 2011;55:2976–2978. 22. Division of AIDS. National Institute of Allergy and Infectious Diseases, National Institutes of Health, US Department of Health and Human Services. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events, Version 2.1. 2017. Available from: https://rsc.niaid.nih.gov/sites/default/files/daidsgradingcorrectedv21.pdf. Accessed September 27, 2022. 23. Cambou MC, Landovitz RJ. Challenges and opportunities for preexposure prophylaxis. Top Antivir Med. 2021;29:399–406. 24. Matthews RP, Ankrom W, Friedman E, et al. Safety, tolerability, and pharmacokinetics of single- and multiple-dose administration of islatravir (MK-8591) in adults without HIV. Clin Transl Sci. 2021;14:1935–1944. 25. Matthews RP, Jackson Rudd D, Zhang S, et al. Safety and pharmacokinetics of once-daily multiple-dose administration of islatravir in adults without HIV. J Acquir Immune Defic Syndr. 2021;88:314–321. 26. Barrett SE, Teller RS, Forster SP, et al. Extended-duration MK-8591-eluting implant as a candidate for HIV treatment and prevention. Antimicrob Agents Chemother. 2018;62:e010518. 27. Patterson KB, Prince HA, Kraft E, et al. Penetration of tenofovir and emtricitabine in mucosal tissues: implications for prevention of HIV-1 transmission. Sci Transl Med. 2011;3:112re4. 28. Cottrell ML, Yang KH, Prince HMA, et al. A translational pharmacology approach to predicting outcomes of preexposure prophylaxis against HIV in men and women using tenofovir disoproxil fumarate with or without emtricitabine. J Infect Dis. 2016;214:55–64.
留言 (0)