
記住我

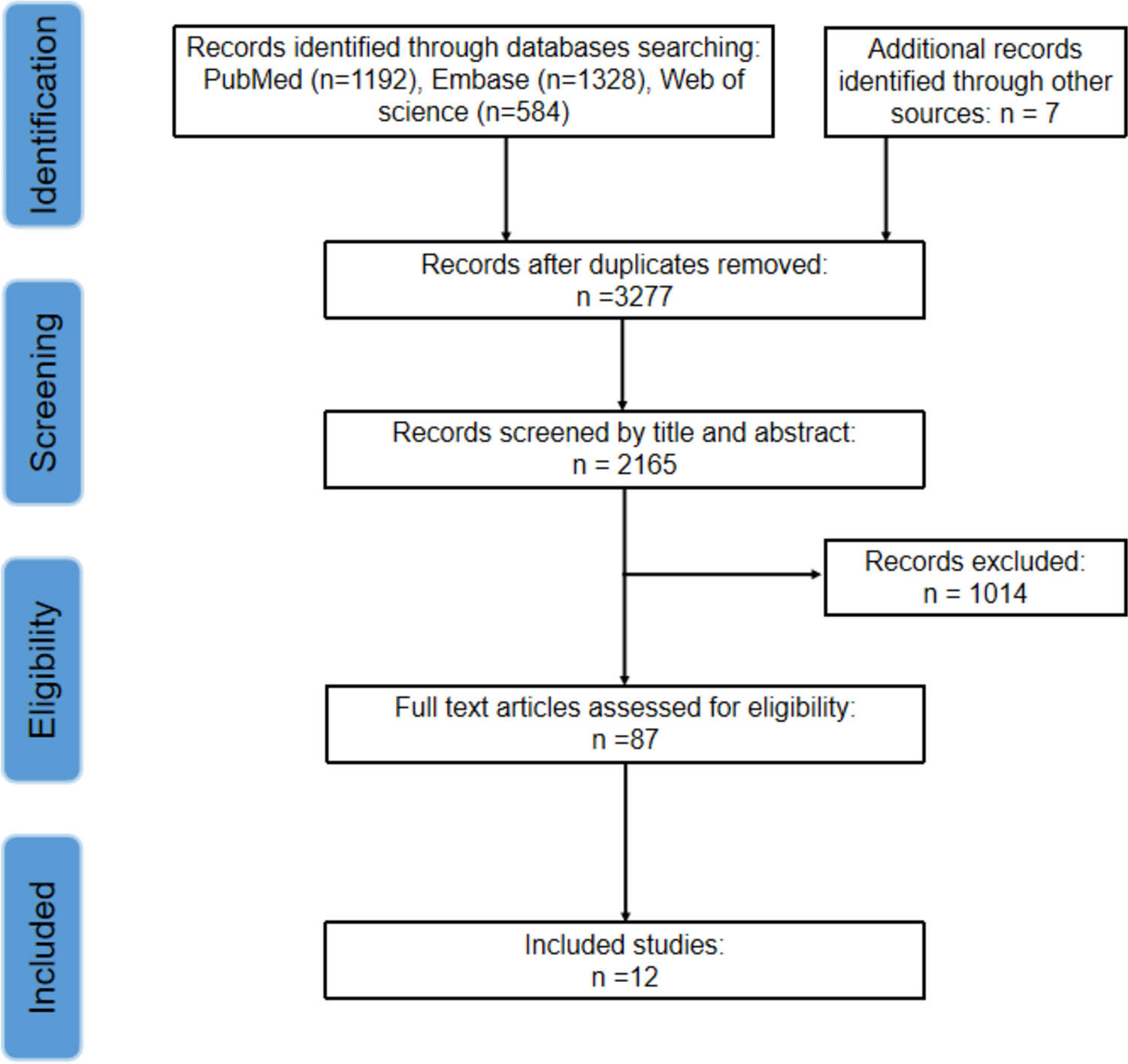


The search produced a total of 6453 results across all databases, with 13 additional records identified by authors. After deduplication 4015 possible studies remained. We excluded 3971 records based upon title and abstract, leaving 44 full text records. We excluded 28 records as they were not randomised controlled trials of IRT versus sedentary control in people with hypertension. A list of excluded studies with reasons is provided (Supplementary Table S2). We excluded 5 records, and all 13 records identified by authors as these were secondary reports. Twelve studies with a total of 415 participants (213 IRT and 202 controls) with hypertension were included in this review [14,15,16, 24,25,26,27,28,29,30,31,32] and qualitative analysis (Supplementary Fig. S1).
Characteristics of Included StudiesCharacteristics of included studies are detailed in Table 1. The studies varied in size from 11 to 79 participants. The studies by Farah et al. [26] and Gordon et al. [24] each had two intervention groups listed as Home and Supervised or Laboratory resulting in 14 comparison groups. Two studies had secondary publications of the same participants. Two studies used a randomised crossover design [15, 32], and we used data from both parts of the crossover design for Taylor et al. [32] but only the first part for Nemoto et al. [15] as it was unclear if the wash-out period was sufficient.
Table 1 Summary of included study characteristicsParticipant CharacteristicsParticipants varied between studies in terms of body mass index (BMI) classification; two studies had participants of normal BMI; one study had borderline normal/overweight participants; one study had overweight participants; three studies used borderline overweight/obese participants; two studies had obese participants; and three studies provided no BMI data. With respect to participant gender, two studies provided no information [24, 29], while the remaining studies included both males and females. Two studies were of unmedicated participants [16, 32], and the other studies had medicated participants. Smoking information was not available for four studies; the other studies were of non-smokers. Three studies confirmed participants had no co-morbid disease, while this information was unavailable for other studies.
Exercise Program CharacteristicsAll but one study used handgrip IRT at 30% of MVC [32]. This study used lower limb wall squats at a joint angle designed to elicit a specific heart rate response, but this method may not precisely reflect a specific MVC%. One study used a method to prescribe MVC that may have been imprecise as it assigned participants to one of four pre-determined workloads, rather than the common practice to periodically assess each person’s MVC and assign them to 30% of maximum load achieved [15]. Study duration varied from 4 to 12 weeks with the most common duration 8 weeks. Session frequency was most often three per week; the only exceptions was five weekly sessions and instruction to participants of ‘at least three per week’ [15].
Resting Systolic Blood PressureIn a pooled analysis of 12 studies (14 comparison groups – 415 participants), IRT significantly reduced SBP with a mean difference (MD) of − 7.47 mmHg (95%CI − 10.10, − 4.84), P ≤ 0.01, I2 = 57% (Fig. 1a).
Fig. 1
Change in systolic (A) and diastolic (B) blood pressure: IRT versus control
Systolic Blood Pressure Sub-analysesAll sub-analyses for SBP can be seen in Fig. 2.
Fig. 2
Sub-analysis of systolic blood pressure outcomes: arm vs leg, study duration, unilateral vs bilateral, unmedicated vs medicated
Arm Versus Leg IRTWhen the one study that used lower limb IRT was removed, the change in SBP for handgrip only IRT was MD − 6.45 mmHg (95%CI − 8.65, − 4.25), and the single study that used leg IRT produced a mean SBP reduction of − 12.6 mmHg (95%CI − 15.66, − 9.54), both P < 0.001.
IRT Program DurationIRT for 4, 8, 10, and 12 weeks showed significant reductions in SBP, although the one study of 6 weeks, with only 11 participants, was not significant.
Unilateral Versus Bilateral IRTBoth these sub-analyses produced significant and similar reductions in SBP with bilateral IRT participants demonstrating a MD − 7.86 mmHg (95%CI − 11.21, − 4.52), P < 0.001, and unilateral IRT participants MD − 7.11 mmHg (95%CI − 11.15, − 3.07), P = 0.001.
Medicated Versus Unmedicated ParticipantsBoth these sub-analyses produced significant, but similar, reductions in SBP with unmedicated participants showing a MD − 12.82 mmHg (95%CI − 15.74, − 9.90) and medicated participants MD − 6.1 mmHg (95%CI − 8.07, − 4.14), both P < 0.001.
24-h Mean Ambulatory Systolic Blood PressureIRT did not significantly reduce 24-h mean ambulatory SBP; MD − 4.09 mmHg (95%CI − 9.26, 1.09), P = 0.12, I2 = 92%, in a pooled analysis of 4 studies (5 comparison groups), with an aggregate of 147 participants (Supplementary Fig. S2).
Day-time ambulatory SBP was not significantly reduced MD − 3.77 mmHg (95%CI − 9.39, 1.84), P = 0.19 (Supplementary Fig. S3); however, night-time SBP was significantly reduced MD − 4.28 mmHg (95%CI − 7.88, − 0.67), P = 0.02 (Fig. 3a).
Fig. 3
Change in night-time ambulatory systolic (a) and diastolic (b) blood pressure: – IRT versus control
Resting Diastolic Blood PressureIn a pooled analysis of 12 studies (14 comparisons – 415 participants), IRT significantly reduced DBP with MD − 3.17 mmHg (95%CI − 5.29, − 1.04), P < 0.01, I2 = 64% (Fig. 1b).
Diastolic Blood Pressure Sub-analysesAll sub-analyses for DBP can be seen in Fig. 4.
Fig. 4
Sub-analysis of diastolic blood pressure outcomes: arm vs leg, study duration, unilateral vs bilateral, unmedicated vs medicated
Arm Versus leg IRTWhen the one study that used lower limb IRT was removed, the change in DBP for handgrip only IRT was significantly lower with MD − 2.80 mmHg (95%CI − 5.08 to − 0.52), P = 0.016, and the single study that used leg IRT produced a DBP reduction of MD − 6.00 mmHg (95%CI − 9.67, − 2.33), P = 0.001.
IRT Program DurationIRT for 4 weeks MD − 6.00 mmHg (95%CI − 9.67, − 2.33), P = 0.001, and 8 weeks MD − 5.21 mmHg (95%CI − 8.74, − 1.67), P = 0.004, showed significant reductions in DBP. Program durations of 6, 10, and 12 weeks were not significant.
Unilateral Versus Bilateral IRTBilateral IRT participants demonstrated a significant DBP reduction of MD − 2.99 mmHg (95%CI − 4.95, − 1.03), P = 0.003, whereas in unilateral IRT participants, the DBP reduction MD − 1.79 mmHg (95%CI − 7.98, 4.40), P = 0.57, was not significant.
Medicated Versus Unmedicated ParticipantsUnmedicated participants produced a significant reduction in DBP MD − 6.20 mmHg (95%CI − 9.48, − 2.91), P < 0.001, and medicated participants also showed a significant DBP reduction MD − 2.51 mmHg (95%CI − 4.88, − 0.14), P = 0.04.
24-h Mean Ambulatory Diastolic Blood PressureIRT did not significantly reduce 24-h mean ambulatory DBP with MD − 1.98 mmHg (95%CI − 4.53, 0.58), P = 0.13, I2 = 70%, in a pooled analysis of 4 studies (5 comparisons), with 147 participants (Supplementary Fig. S4).
Day-time ambulatory DBP was not significantly reduced MD − 1.02 mmHg (95%CI − 2.97, 0.94), P = 0.31, I2 = 48% (Supplementary Fig. S5); however, night-time DBP was significantly reduced with MD − 2.22 mmHg (95%CI − 3.55, − 0.88), P < 0.01, I2 = 1% (Fig. 3b).
Resting Mean Arterial Blood PressureIn a pooled analysis of 7 studies (8 comparisons – 184 participants), IRT significantly reduced MAP with MD − 7.19 mmHg (95%CI − 9.06, − 5.32), P < 0.0001, I2 = 0% (Fig. 5).
Fig. 5
Change in mean arterial blood pressure: IRT versus control
24-h Average Ambulatory Mean Arterial Blood PressureOnly two studies provided this data, and a pooled analysis was not possible.
Resting Brachial Pulse PressureIn a pooled analysis of 6 studies (7 comparisons – 261 participants), IRT did not significantly reduce pulse pressure; MD − 1.15 mmHg (95%CI − 2.43, 0.13), P = 0.08, I2 = 0% (Supplementary Fig. S6).
Resting Heart RateIn a pooled analysis of 8 studies with 294 participants, IRT did not significantly reduce resting heart rate; MD − 1.99 beats/min (95%CI − 4.42, 0.43), P = 0.11, I2 = 36% (Supplementary Fig. S7).
Adverse EventsThere were no major adverse events reported.
Study QualityMedian TESTEX score was 10 (range 9–13); see Table 2. Four items were done poorly in more than 50% of studies: allocation concealment (4 studies), blinding of assessors (3 studies), and activity monitoring in control groups (0 studies) and energy expenditure (0 studies).
Table 2 Summary of TESTEX assessment of study quality and reporting of included studiesRisk of Bias and HeterogeneityThe risk of bias for randomisation was considered low as most groups were matched for key participants characteristics at baseline. As blinding of participants to exercise therapy is not possible, the risk of bias on a possible placebo effect is not possible. As eight of the 12 studies failed to blind investigators to group allocations, there is a possibility of measurement bias.
Heterogeneity was moderate to high for most analyses, but no reasons were identified for this. A possible explanations are study size, manual blood pressure measurement, medication status, and IRT study duration.
GRADE Recommendations for the EvidenceThe GRADE assessment can be seen in Table 3. For two of the five outcomes selected, systolic and diastolic blood pressures, the GRADE recommendation was rated as high certainty of evidence. For MAP as well as night-time ambulatory SBP and DBP, the GRADE recommendation was rated moderate certainty of evidence as the effect size was smaller and rated less important for these outcomes.
Table 3 GRADE-pro summary table of IRT compared to control in the management of hypertension
留言 (0)