
記住我

There is growing recognition of ineffective practices and systemic waste in healthcare services, with evidence that up to 30% of healthcare provision is unnecessary.1 In the United Kingdom and Australia, this waste occurs in healthcare systems facing acute shortages of time and resources.2,3 Recent research has increasingly focused on the identification and cessation of medical tests, treatments, and procedures that deliver minimal or no benefit, be it through overuse, misuse, or waste.4–8 This has driven the “Choosing Wisely” campaign, which encourages patients and healthcare professionals to choose care that is evidence based, free from harm, and truly necessary.9 This, now a global initiative, involves 20 countries in which medical societies regularly identify and review common practices, of questionable necessity. For example, in Australia, the NPS MedicineWise partnered with the South Australian Clinical Senate to identify the top 5 practices for removal, congruent with the Choosing Wisely campaign objectives.10 Similarly, in the United Kingdom, the National Institute for Health and Clinical Excellence provides online recommendations and “do not do” reminders to enable clinicians to conduct evidence-based best practice.11
The publication of “To Err Is Human: Building a Safer Health System” prompted a global surge in research and investment in improving patient safety, leading to the introduction of patient safety practices (PSPs) designed to reduce the likelihood of adverse events.12 Despite progress in patient safety since this publication, the value of certain PSPs has been questioned. For example, previous research reported that some innovative PSPs have been implemented despite insufficient evidence in an attempt to address urgent quality and safety problems, e.g., mandates to reduce staff working hours.13 Although well meaning, the implementation of PSPs based on anecdotal evidence may lead to unintended consequences and wasted resources. The introduction of PSPs may also contribute to the problem of “safety clutter,” which is the accumulation of safety procedures, checklists, and activities performed in the name of safety that do not actually contribute to safety.14
To improve the quality of care and create more sustainable health services, it is necessary to consider the deimplementation of low-value PSPs. While there has been research to identify those PSPs ready for adoption and so by default those that are not,15 evidence exploring removal of ineffective PSPs is lacking. Previous research has highlighted the need to scrutinize the value of PSPs to prevent unintended patient outcomes. However, there has been minimal focus on identifying low-value PSPs specifically.16 Progressing this issue could increase capacity for staff to deliver more effective, patient-centered care.
A first step toward deimplementation is to identify low-value PSPs. Previous attempts to identify potential practices for deimplementation have involved using top-down strategies to decide which clinical practices are not cost effective and then developing guidelines to discourage their use.17 This approach has proved difficult to implement.18 Consulting staff about potential opportunities for disinvestment may be more effective in supporting the deimplementation of low-value care. This study aimed to address this gap by identifying PSPs that healthcare staff perceived to be low value because they do not contribute to safer care.
Research Questions:
1) What PSPs are most commonly perceived to be low value by healthcare staff in the United Kingdom and Australia? 2) Why are the identified PSPs perceived to be low value? METHODS Sampling and RecruitmentSnowball sampling was used to recruit healthcare staff using Facebook and Twitter.19 Purposive sampling was also used to recruit participants from wards in a medium-sized teaching hospital in the North of England and a medium-sized tertiary referral hospital in Sydney to promote inclusion of staff who did not use social media.
ProcedureThe online survey was circulated via social media between April 2018 and November 2019 (United Kingdom) and May 2020 to November 2020 (Australia). Paper versions were distributed in person on 10 wards (September 2019–November 2019) in the United Kingdom and 9 wards in Australia (May 2020–November 2020). Completed paper surveys were collected from sealed collection points on wards.
Survey DesignThe UK questionnaire was developed over 4 piloting phases involving 59 healthcare staff and patients. It was designed for quick and simple completion. As the phrase “low value” was not widely understood, researchers tested different options for example, “I would like to stop doing the following safety practice even though I am supposed to because I don’t think it benefits safety” until one was identified that was commonly understood by most participants. The final UK questionnaire (Supplementary File 1, https://links.lww.com/JPS/A519) included demographic questions and one main question: “It is a waste of time doing ‘X’ because it doesn’t make care safer. Please tell us what ‘X’ is below. You can list more than one answer.” The Australian survey (Supplementary File 2, https://links.lww.com/JPS/A520), used the same demographic questions with context-related modifications and included the additional question: “Please write any further comments in the box below, in particular, why you think ‘X’ is a waste of time.”
EthicsEthical approval was granted from the University of Leeds (No: PSC-730, 26/07/2019), the Health Research Authority (19/HRA/4755, 19/08/19), and St Vincent’s Hospital Sydney Human Research Ethics Committee (HREC) (2020/ETH00072, 05/02/2020) and was ratified by University of Technology Sydney HREC (ETH20-4808, 02/03/2020).
Data Analysis Qualitative Content AnalysisD.H. read all UK responses repeatedly before grouping similar practices together into categories using open coding (where codes are developed and modified during the coding process rather than using predefined codes).20 Uncertainty about the meaning of responses was clarified with a research nurse. Initial categorization of practices was reviewed by G.J. (50%) and R.L. (50%) who agreed with 75% of the initial coding, with discrepancies resolved by discussion. Responses categorized as “can’t think of anything,” ‘misunderstood,” “disagree,” or “N/A” were removed upon consensus between reviewers because they did not address the research questions. Additional responses considered too vague, for example, “emails,” or not a behavior, for example, “slow processing laptops” were also removed. All remaining practices were then reviewed again by D.H. who removed practices, which did not meet the following definition of a PSP, “a type of process, structure [or behaviour] whose [purpose] is to reduce [directly or indirectly] the probability of adverse events resulting from exposure to the health care system.” Adaptations [in brackets] were made to the original definition by Shekelle et al16 (2013) to aid its application in this context. For practices D.H. was uncertain about (7% of remaining practices), R.L. and G.J. jointly made a decision on whether they met the definition. Where R.L. and G.J. disagreed or were uncertain, advice was sought from relevant clinicians (e.g., nurse, doctor, or pharmacist) and a final consensus decision was reached through discussion. The frequency of the remaining practices was then calculated (Fig. 1).
 FIGURE 1:
FIGURE 1: United Kingdom responses flowchart.
This process was repeated for the Australian survey responses (Fig. 2). D.D., J.C., and S.S.L. acted as independent second reviewers and agreed with 77% of the initial codes. D.D., J.C., and S.S.L. together also reviewed the practices where D.H. was uncertain if they met the definition of a PSP (3%).
 FIGURE 2:
FIGURE 2: Australian responses flowchart.
Thematic AnalysisThe UK data were subject to thematic analysis after the first round of elimination.21 D.H., G.J., and R.L. reviewed responses independently and identified higher-order, cross-cutting themes based on those responses that provided insight into why staff perceived the practices identified to be of low value. After discussion, similar themes were merged and adjusted to reach consensus on the final, cross-cutting themes. D.H. then coded all responses into these themes. Free-text coding of the Australian data was conducted using the framework developed to analyze UK responses. D.H. also reviewed the responses to identify any additional cross-cutting themes, which may not have been identified in the UK data. D.D. and J.C. reviewed D.H.’s categorization of responses to the cross-cutting themes.
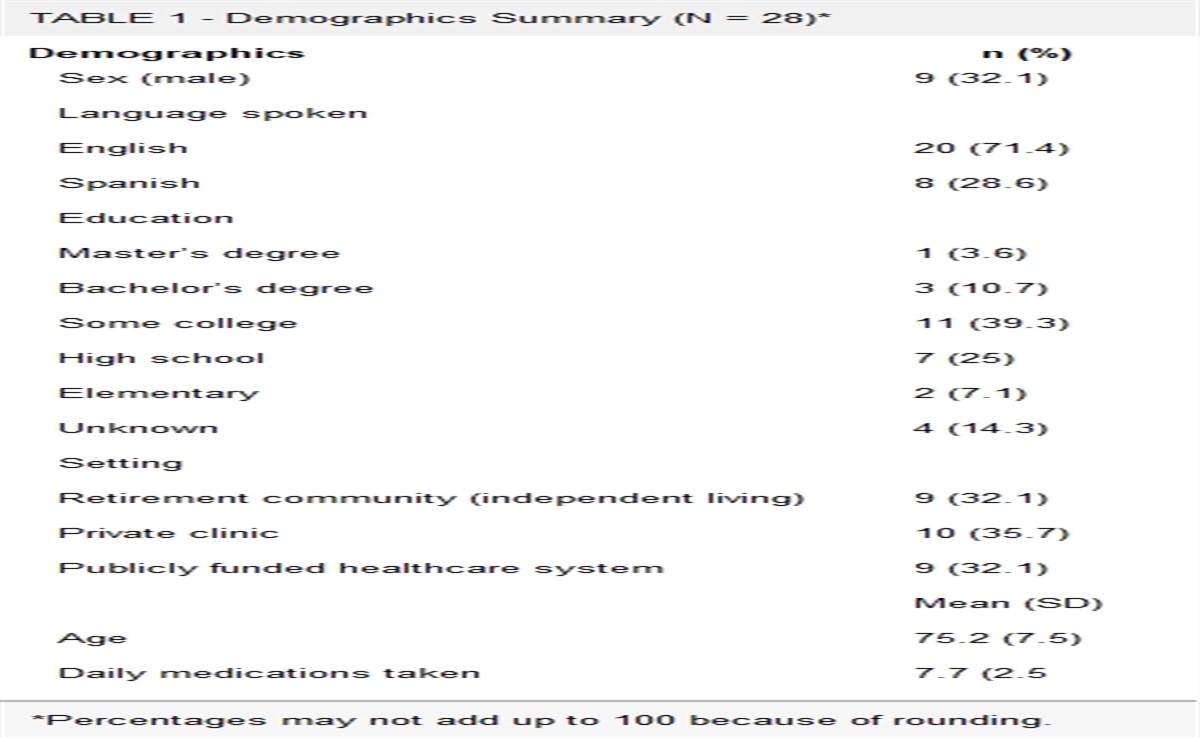
RESULTSParticipants in both samples were mostly clinical staff, although nonclinical staff were also represented (Table 1).
TABLE 1 - Number of Participants by Occupation (Including Proportion Online and Proportion of Occupation by Total Sample per Country) Occupation Online: United Kingdom Total: United Kingdom (Online and Paper) Online: Australia Total: Australia (Online and Paper) Nurse 99 (70%) 142 (27%) 196 (85%) 213 (44%) Pharmacist 84 (98%) 86 (16%) 3 (50%) 6 (1%) Doctor 71 (93%) 76 (14%) 73 (100%) 73 (14%) Manager 19 (86%) 22 (4%) 39 (98%) 40 (8%) Healthcare assistant 17 (52%) 33 (6%) 2 (100%) 2 (<1%) Midwife 14 (93%) 15 (3%) 10 (100%) 10 (2%) Student 11 (92%) 12 (2%) 4 (100%) 4 (1%) N/A 10 (77%) 13 (3%) 13 (100%) 13 (3%) Paramedic 10 (100%) 10 (2%) 8 (89%) 9 (2%) Clinical researcher 9 (69%) 13 (3%) 18 (78%) 23 (4%) Occupational Therapist 5 (100%) 5 (1%) 3 (100%) 3 (<1%) Physiotherapist 5 (83%) 6 (1%) 6 (86%) 7 (1%) Head of department 4 (100%) 4 (1%) 7 (100%) 7 (1%) Administrator 1 (33%) 3 (1%) 10 (44%) 23 (4%) Director 3 (100%) 14 (100%) 14 (3%) Social worker 0 (0%) 0 22 (96%) 23 (4%) Other 65 (75%) 86 (16%) 35 (78%) 45 (9%) Total 427 526 463 515Five hundred twenty-six healthcare staff completed the survey, contributing a total of 663 suggestions for low-value PSPs. Most participants worked in secondary (acute) care (n = 366, 70%) and were based in the Yorkshire and Humber NHS region (n = 227, 43%). Of the 663 responses, 82 were removed because they were: (1) “unable to think of an answer” (n = 2), (2) “misunderstood” (n = 9), for example, “it is not a waste of time striving to better patient care,” (3) “disagree” (n = 6) where the participant disagreed with the question, for example, “I believe nothing is a waste of time,” and (4) “N/A” (n = 65), for example, “no comment” (Fig. 1).
When finalizing the short list of the most frequently reported safety practices, a further 216 responses were removed because they (a) were not practices, but rather organizational policies (n = 110), for example, “some quality payment targets” or (b) lacked sufficient information to know what was being referred to (n = 106), for example, “ticking boxes.” Then, all responses that did not meet the abovementioned PSP definition were also removed (n = 26), for example, “cost saving prescribing switches.”
Table 2 displays the four most frequently mentioned categories of safety practices perceived to be low value. Supplementary File 3, https://links.lww.com/JPS/A521, contains the final list of included practices.
TABLE 2 - Frequency of Perceived Low-Value Safety Practices (United Kingdom) by Category and Highest Scoring Example Practices Category Frequency Example Practice 1. Paperwork 73 (Assessments) 23 Falls risk assessment (Duplication) 16 Writing the same information in different documents (Audits) 12 Completing hand hygiene audits 2. Duplication 43 Double-checking medication 3. Intentional rounding 27 Intentional rounding* 4. Incident reporting 25 Completing incident reports * Intentional rounding is a structured process whereby nurses or healthcare assistants check on patients in hospitals, usually hourly, to assess their positioning, pain, personal needs, and placement of items.22Five hundred fifteen healthcare staff completed the survey, producing 731 suggestions of low-value PSPs. Most participants worked in hospital settings (n = 384, 74%) and were based in New South Wales (n = 352, 68%). The flowchart in Figure 2 displays the process for screening responses and arriving at the final shortlist of 460 practices. Table 3 displays the 4 most frequently mentioned categories. Supplementary File 4, https://links.lww.com/JPS/A522, contains the final list of included practices.
TABLE 3 - Frequency of Low-Value Safety Practices (Australia) by Category and Highest Scoring Example Practices Category Frequency Example 1. Paperwork 196 (Assessments) 82 Waterlow assessment* (Evidencing care) 32 Completing the intentional rounding (Checklists) 20 document Safety checklists 2. Mandatory training 40 Hand hygiene training 3. Duplication 34 Duplicating information on paper and electronic systems 4. Task allocation 25 Administrative tasks carried out by clinicians *A Waterlow score is a routinely used practice that assesses the risk of pressure sore development in patients.23Five cross-cutting themes were identified in both data sets to explain participants’ perceptions of why these practices were low value. Themes are presented in order of dominance with the most dominant discussed first.
A blanket policy is a healthcare procedure that is applied across patient groups and not adapted to suit individual patient need. Although blanket safety policies are implemented to mitigate preventable adverse events, for example, thromboembolism in certain patient groups, some respondents perceived mandatory completion of such checks on patients at very low risk to be a waste of time: for example:
“Doing falls risk assessment for obviously very low-risk patients” (Australia).
Similarly, participants suggested that some blanket policies, not only wasted staff time but also had potential to cause harm when carried out on patients who are unlikely to benefit. For example:
“Routinely checking hourly on sleeping patients when there is no reason to think they will harm themselves during the night and shining a light on them just wakes them up (United Kingdom).”
Some healthcare staff considered a task to be unnecessary because it did not have a visible effect on patient safety but policy required it, for example:
“Doing tasks because the standards say so, rather than it’s of benefit to care” (Australia).
These responses suggest that either healthcare staff believe they carry out certain practices for no safety benefit, perhaps not being informed of, or not fully understanding their benefits.
Participants reported some administrative tasks they are required to complete are a “waste of time” because they take staff away from providing direct care to produce evidence of completed safety-related tasks (e.g., safety checklists). While participants understood that many administrative tasks were introduced to reduce the risk of adverse events, they also conveyed beliefs that the volume of administrative tasks meant that this strategy had become counterproductive, potentially detracting from rather than enhancing patient safety, for example, “Filling in multiple forms to indicate care done… forms become more important than doing the care” (United Kingdom).
This theme encompassed all responses mentioning administrative burden of recording completed care tasks at the expense of quality of that care. Some participants perceived the focus to be more on reducing legal risk should an adverse event occur than increasing patient safety:
“Obsessive admin[istration] doesn’t change patient care but does cover our backs—at the cost of time” (United Kingdom).
“It is aimed at protecting the employer rather than the patient” (Australia).
In addition, some responses in this theme described some healthcare tasks as “tick box exercises” that do not enhance patient safety but rather are mandated to demonstrate that the healthcare professional practiced appropriately. For example:
“Doesn’t make patients safer, just shows that nurses have read the form and ticked the box so they score 100% on the audits” (Australia).
Staff highlighted that performing tasks outside of their scope of practice takes them away from their core caring responsibilities. Many responses identified specific tasks often carried out by healthcare staff that are not their responsibility:
“Sorting out IT issues are an inefficient use of my time which should be spent on clinical rather than administration tasks” (Australia).
In addition, some participants reported that certain tasks, which are part of their job description, should be allocated to other staff with a more appropriate skill set, to ensure more specialized healthcare professionals have time to complete tasks that require specific expertise:
For example, “…having to do regular CD (controlled drugs) checks as pharmacists… this task could be done by pharmacy technicians and would save time for the pharmacists to focus on seeing patients” (United Kingdom).
In this way, some participants felt that doing a task that could be completed by someone with more basic skills training was a waste of time. Therefore, whether a task is perceived as a “waste of time” can depend on who is performing it rather than the task itself.
4. Approaches to Implementation of Safety PracticesSome participants felt the way certain practices are implemented can detract from patient safety. A policy might be instigated, which, if carried out according to the guidelines, enhances patient safety. However, if that policy is disseminated without the appropriate guidance or implementation strategy, healthcare staff may carry out the practice in a way that was not originally intended or not at all, potentially causing more harm than good.24 Participants identified that certain policies that are difficult to adopt can be low value, for example, “Policies and protocols at high-level without a real focus on implementation” (United Kingdom).
Therefore, participant responses indicated that the way a policy is implemented in practice can determine its perceived usefulness in enhancing patient safety.
The theme “lack of impact” was identified when analyzing the Australian data. After its identification, the research team rereviewed the UK data and found that although less prominent, several UK responses were congruent with this theme.
Some staff noted that healthcare practices can be a waste of time if they do not lead to discernible action or change, for example, “…writing these (local operating procedures)… makes no difference it’s just another thing to read” (United Kingdom).
These examples highlight the lack of motivation experienced when completing tasks for seemingly no benefit, for example, completing audits without implementing a plan for positive change. In addition, some participants noted that certain practices can have a negative impact on staff: for example, “it just tells staff that we are doing poorly at things and rarely has positive benefits or enforcement of better behaviors” (Australia). Therefore, some practices can be perceived as low value because they induce negative feelings among staff that are not conducive to facilitating improvements in care.
DISCUSSIONThe aim of this study was to identify PSPs that healthcare staff perceived to be low value. Previous research focuses on identifying clinical areas of low value in health care.5,8,25 This study is unique because it concentrates on identifying potential low-value PSPs based on healthcare staff perception and provides an alternative method for identifying candidate practices for deimplementation that directly involves staff. Healthcare staff groups across the United Kingdom and Australia were willing to identify practices they believed were of little value for patient safety. Certain factors were identified as important to consider when determining the value of PSPs, for example, the context in which a practice is carried out and who is performing it.
In the United Kingdom, “paperwork” was perceived by staff to represent the greatest “waste of time” with the subcategory “paperwork (assessments)” containing most responses, including practices such as falls risk assessments or pressure injury risk assessments. “Duplication” was also perceived by healthcare staff to waste time, with “double-checking medication” being the most identified behavior within this category. “Intentional rounding” and “incident reporting” were also frequently mentioned in survey responses. In the Australian data, the category “paperwork (assessments)” also contained the greatest number of responses, with “Waterlow assessment” the most frequently mentioned practice within this category. The present study detected 5 cross-cutting themes across both data sets that provide some explanation of why staff perceived the practices to be “a waste of time.” These themes highlighted issues relating to the removal of professional autonomy and reducing direct patient care time. In addition, themes highlighted that some practices were only deemed “a waste of time” when applied universally to all patients or when performed by certain staff groups.
Existing evidence supports the dubious value of many of the practices staff identified, at least in the way they are currently implemented. For example, the value of “incident reporting” for improving patient safety has been questioned repeatedly.26–28 This practice, although well intended, and central to many efforts to improve healthcare safety, suffers from a variety of limitations, including physician underreporting and, when incidents are reported, visible action in response to these is rare.29 There is limited research demonstrating the benefits of “intentional rounding,” another practice highlighted by UK staff in our study. The evidence that does exist has been questioned because of concerns regarding: selection bias, study design, and data analysis.22,30,31
One of the most frequently mentioned practices UK staff perceived to be low value was double-checking medication. This widely adopted procedure is used when administering specifically classified drugs to ensure the correct dose and drug are given to the correct patient at the right time. Despite evidence that double checking makes healthcare professionals feel safer when administering drugs in high-risk situations,32 it requires additional nursing resource and causes workflow interruptions that may introduce other risks.33 Evidence demonstrating that double-checking medication is associated with reduced harm compared with single checking is inconclusive.34 Therefore, the perceptions of healthcare staff regarding double-checking medication reported in this study are congruent with evidence suggesting potential low value for patient safety, particularly when applied routinely to low-risk medicines, or not executed as intended.35
Similar questions have been raised in the literature about those practices most frequently identified in the Australian data. For example, a systematic review explored whether using pressure injury risk assessment tools, including Waterlow assessments, reduces the incidence of pressure injuries.23 It identified just 2 eligible studies, both of which found no significant difference in pressure ulcer incidence when participants were assessed using a structured assessment compared with unaided clinical judgment.
Mandatory training was also commonly identified as a low-value safety practice across both data sets. Mandatory training for healthcare professionals is required by commissioning bodies and nonadherence can negatively impact care quality ratings.36 Hand hygiene training was the most frequently identified practice within this category in the Australian data. It is well established that effective training can improve hand hygiene practices among healthcare professionals, thus reducing risk of infection.37 However, there is considerable variation in adherence to best hand hygiene practice among healthcare professionals globally, indicating that improvement is required to prevent patient harm.38–40 Rather than investigating whether this practice is appropriate for deimplementation, it would be more useful to explore why healthcare staff perceived hand hygiene training to be low value and how it can be modified to become less onerous. Previous evidence suggests that mandatory training takes too much time to complete and is required unnecessarily frequently, suggesting the way a practice is implemented can detract from its perceived value.41 This finding highlights that some practices identified in the present study as low-value PSPs will not be appropriate for deimplementation but should prompt investigation into how they can be implemented more effectively to streamline staff workload and thereby improve patient safety.
The cross-cutting themes identified also align with previous literature exploring healthcare professional perspectives on low-value health care. For example, “fear of litigation,” previously identified to be an underlying reason for the overuse of low-value practices, relates to the present theme of “covering ourselves.”42–44 Implementation problems45 and professional autonomy46 are known to influence staff perception of the value of tasks and were also referred to herein “approaches to implementation” and “not my job.”
Understanding why healthcare staff perceive a PSP to be low value is crucial for deimplementation, as merely making healthcare professionals aware that they should stop a practice does not translate to behavior change.47 There are no clear guidelines on how to approach deimplementation in health care.8 Deimplementation must involve healthcare providers, commissioners, and patients in the decision-making process.15 Soliciting ideas from staff about opportunities to reduce low-value PSPs is essential when creating the optimal conditions for sustainable change.48 Healthcare staff perception of the potential benefits of a practice can affect the pace and extent to which it is deimplemented.49 Staff input should be considered alongside additional factors, including strength of evidence underpinning the practice, cost-effectiveness, and magnitude of the problem when identifying an appropriate low-value safety practice for deimplementation.50 The methods used in this study provide a starting point for a joint approach to removing low-value PSPs.
A strength of this study is that survey responses were collected from a variety of staff across the United Kingdom and Australia, enhancing the representativeness of the sample. Using online and paper-based data collection enabled the team to engage healthcare staff who did not use social media. Finally, anonymity of responses is likely to have improved participation.51
The present study also has limitations. Despite iteration during multiple rounds of piloting with staff, the survey generated a substantial number of responses, which could not be analyzed because participants disagreed with the question, misunderstood, could not think of an answer or responded with “N/A” (United Kingdom: 82, 12%; Australia: 127, 17%). Although this may be attributed to healthcare workers’ unfamiliarity with discussing deimplementation or the absence of an established terminology surrounding the subject,52 it may also be due to confusion regarding the nonspecific phrase “a waste of time.” Furthermore, allowing healthcare staff to interpret the phrase “a waste of time” may have prompted identification of practices they disliked doing, rather than those they felt did not enhance patient safety.
CONCLUSIONSHealthcare staff in the United Kingdom and Australia identified practices of perceived low value for safety. The resulting short lists of practices can now be subjected to further evaluation (e.g., evidence base, cost-effectiveness, and magnitude of the problem) to determine appropriateness for deimplementation. Participants provided information about why these practices were low value for safety, often referring to their focus on risk management rather than patient outcomes or uniform and inappropriate use across all patients. Future studies are needed to explore the context and reasons why participants identify certain practices for deimplementation. However, this staff-led approach offers a novel and potentially more context-sensitive method for identifying candidate safety practices for deimplementation within healthcare.
ACKNOWLEDGMENTSThe research is supported by the NIHR Yorkshire and Humber Patient Safety Translational Research Centre (NIHR YHPSTRC). This independent research is funded by The Healthcare Improvement Studies Institute (THIS). The views expressed in this publication are those of the author(s) and not necessarily those of THIS Institute or the NIHR YHPSTRC.
REFERENCES 1. Grimshaw JM, Patey AM, Kirkham KR, et al. De-implementing wisely: developing the evidence base to reduce low-value care. BMJ Qual Saf. 2020;29:409–417. 2. Sanderson M, Allen P, Moran V, et al. Agreeing the allocation of scarce resources in the English NHS: Ostrom, common pool resources and the role of the state. Soc Sci Med. 2020;250:112888. 3. Briggs DS. Challenges for health systems: Australian perspectives. Public Policy Adm. 2017;20:6–17. 4. Elshaug AG, Hiller JE, Tunis SR, et al. Challenges in Australian policy processes for disinvestment from existing, ineffective health care practices. Aust N Z Health Policy. 2007;4:23. 5. Elshaug AG, Watt AM, Mundy L, et al. Over 150 potentially low-value health care practices: an Australian study. Med J Aust. 2012;197:556–560. 6. Garner S, Docherty M, Somner J, et al. Reducing ineffective practice: challenges in identifying low-value health care using Cochrane systematic reviews. J Health Serv Res Policy. 2013;18:6–12. 7. Pearson S, Littlejohns P. Reallocating resources: how should the National Institute for Health and Clinical Excellence guide disinvestment efforts in the National Health Service?J Health Serv Res Policy. 2007;12:160–165. 8. Niven DJ, Mrklas KJ, Holodinsky JK, et al. Towards understanding the de-adoption of low-value clinical practices: a scoping review. BMC Med. 2015;13:255. 9. Parker G, Rappon T, Berta W. Active change interventions to de-implement low-value healthcare practices: a scoping review protocol. BMJ Open. 2019;9:e027370. 10. O’Callaghan G, Meyer H, Elshaug AG. Choosing wisely: the message, messenger and method. Med J Aust. 2015;202:175–177. 11. Garner S, Littlejohns P. Disinvestment from low value clinical interventions: NICEly done?BMJ. 2011;343:d4519. 12. Donaldson MS, Corrigan JM, Kohn LT. To Err Is Human: Building a Safer Health System. Washington (DC) National Academies Press: National Academy Press. 2000. 13. Auerbach AD, Landefeld CS, Shojania KG. The tension between needing to improve care and knowing how to do it. N Engl J Med. 2007;357:608–613. 14. Rae AJ, Provan DJ, Weber DE, et al. Safety clutter: the accumulation and persistence of ‘safety’ work that does not contribute to operational safety. Policy pract Health Saf. 2018;16:194–211. 15. Shojania KG, Duncan BW, McDonald KM, et al. Making health care safer: a critical analysis of patient safety practices. Evid Rep Technol Assess (Summ). 2001;43:668. 16. Shekelle PG, Wachter RM, Pronovost PJ, et al. Making health care safer II: an updated critical analysis of the evidence for patient safety practices. Evid Rep Technol Assess (Full Rep). 2013;1–945. 17. Rooshenas L, Owen-Smith A, Hollingworth W, et al. “I won’t call it rationing...”: an ethnographic study of healthcare disinvestment in theory and practice. Soc Sci Med. 2015;128:273–281. 18. Haas M, Hall J, Viney R, et al. Breaking up is hard to do: why disinvestment in medical technology is harder than investment. Aust Health Rev. 2012;36:148–152. 19. Ghaljaie F, Naderifar M, Goli H. Snowball sampling: A purposeful method of sampling in qualitative research. Strides Dev Med Educ. 2017;14. 20. Maguire M, Delahunt B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. All Ireland J Higher Educ. 2017;9. 21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. 22. Harris R, Sims S, Levenson R, et al. What aspects of intentional rounding work in hospital wards, for whom and in what circumstances? A realist evaluation protocol. BMJ Open. 2017;7:e014776. 23. Moore ZE, Patton D. Risk assessment tools for the prevention of pressure ulcers. Cochrane Database Syst Rev. 2019;1:CD006471. 24. Soong C, Shojania KG. Education as a low-value improvement intervention: often necessary but rarely sufficient. BMJ Qual Saf. 2020;29:353–357. 25. Morgan DJ, Brownlee S, Leppin AL, et al. Setting a research agenda for medical overuse. BMJ. 2015;351:h4534. 26. Shojania KG. The frustrating case of incident-reporting systems. BMJ Qual Saf. 2008;17:400–402. 27. Thomas MJ, Schultz TJ, Hannaford N, et al. Mapping the limits of safety reporting systems in health care—what lessons can we actually learn?Med J Aust. 2011;194:635–639. 28. Brunsveld-Reinders AH, Arbous MS, De Vos R, et al. Incident and error reporting systems in intensive care: a systematic review of the literature. Int J Qual Health Care. 2016;28:2–13. 29. Mitchell I, Schuster A, Smith K, et al. Patient safety incident reporting: a qualitative study of thoughts and perceptions of experts 15 years after ‘To Err is Human’. BMJ Qual Saf. 2016;25:92–99. 30. Snelling PC. Ethical and professional concerns in research utilisation: intentional rounding in the United Kingdom. Nurs Ethics. 2013;20:784–797. 31. Halm MA. Hourly rounds: what does the evidence indicate?Am J Crit Care. 2009;18:581–584. 32. O’Connell B, Hawkins M, Ockerby C. Construct validity and reliability of the single checking administration of medications scale. Int J Nurs Pract. 2013;19:281–287. 33. Mcleod M, Barber N, Franklin BD. Facilitators and barriers to safe medication administration to hospital inpatients: a mixed methods study of nurses’ medication administration processes and systems (the MAPS study). PLoS One. 2015;10:e0128958. 34. Koyama AK, Maddox CSS, Li L, et al. Effectiveness of double-checking to reduce medication administration errors: a systematic review. BMJ Qual Saf. 2020;29:595–603. 35. Westbrook JI, Li L, Raban MZ, et al. Associations between double-checking and medication administration errors: a direct observational study of paediatric inpatients. BMJ Qual Saf. 2021;30:320–330. 36.
留言 (0)