The present study examined prevalence rates of substances use disorders in a large representative sample of German adolescents and associations with mindfulness and related constructs such as impulsivity and sensation seeking. The results add to an empirical base for estimation of treatment needs in the youth population and fill an important gap in the epidemiology of SUDs in Germany. Furthermore, the study contributes to the growing literature on mindfulness as a relevant psychological target for treatment and prevention of substance-related problems.
Prevalence rates of substance use disorders
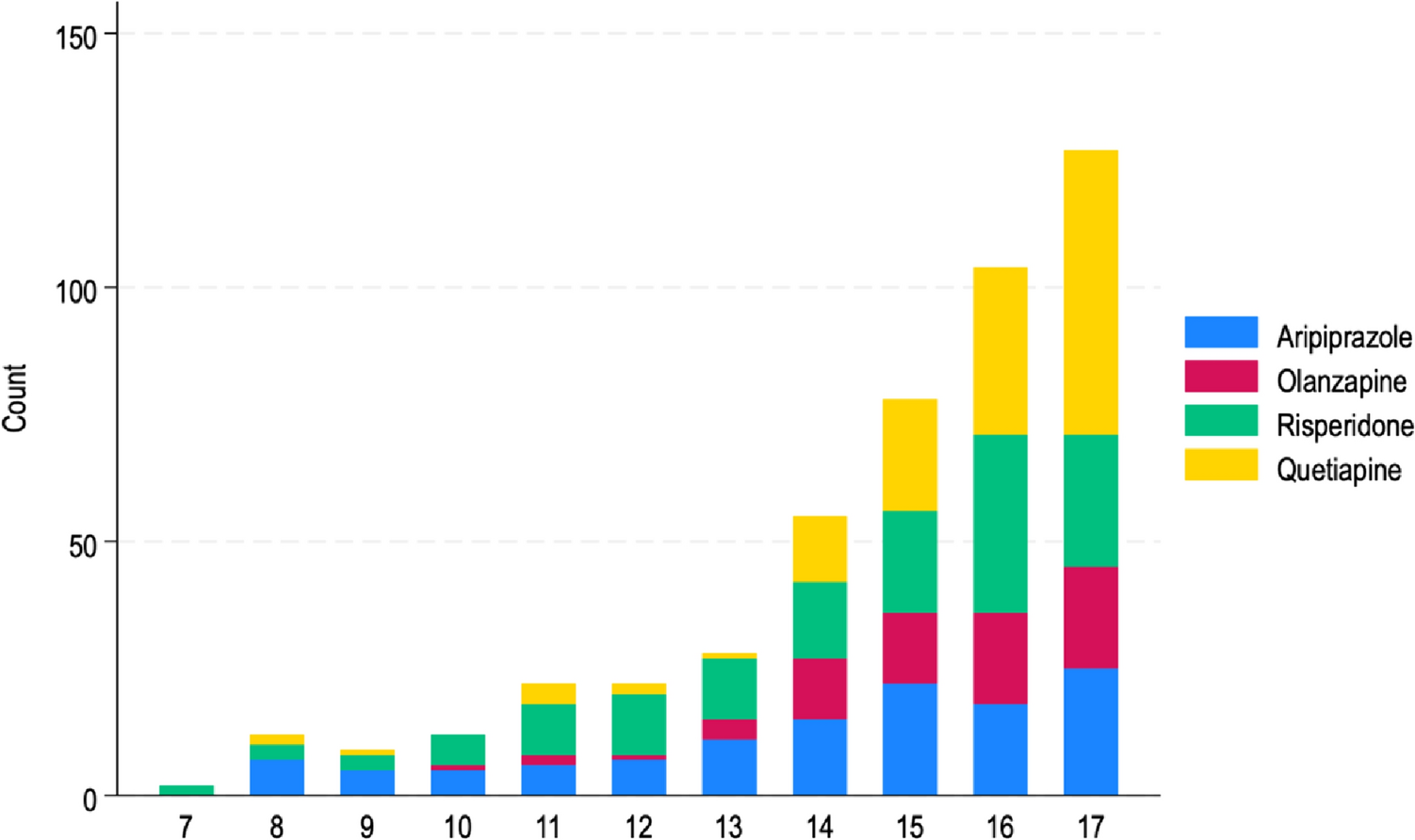
The central study results on SUD prevalences indicate that these disorders are relevant in the youth population and treatment needs for this age group may be similar to those in the adult population in Germany [8]. With the exception of alcohol dependence, all SUD subtypes were more prevalent for male compared to female youth and there was consistent increase with age (except for e-cigarettes dependence). The increases in prevalence rates from early to late adolescence are consistent with previous findings [43, 44] and largely match a “natural” life-course pattern of substance use behavior [45, 46].
Alcohol use disorders
In our adolescent sample, the highest prevalence rate was found for alcohol abuse. Compared to existing recent data from the adult population in Germany, this value is high and even exceeds the prevalence rate of the adult subsample with the highest prevalence rate (age group of 18 to 20 years: 6.7%) [8]. It also clearly exceeds youth prevalence rates for alcohol-related disorders from US-based studies with a range of 1.7% [32] to 4.7% [14]. In turn, the value from our study comes close to the prevalence rate for alcohol abuse from the previous ESDP-study (9.7% [11]). This comparison indicates that although youth drinking in Germany and Europe have been decreasing [47], a substantial proportion of school-aged youths continuous to drink alcohol at levels associated with serious risk of harm. For example, adolescents aged 15 to under 20 are the largest group for emergency care due to acute alcohol intoxication in German hospitals [48].
The diagnostic criteria for alcohol abuse were met more often than those for alcohol dependence (3.1%) and this value is also lower compared to the prevalence reported for the adult population in Germany (4.8%) [8]. This is not surprising given that youth drinking is typically characterized by episodic excessive use (“binge drinking”) [2, 49] and dependence symptoms such as tolerance and withdrawal are less pronounced in adolescence. Given that the neurobiological and pharmacological adaptation processes required for the formation of these physical symptoms usually only occur after prolonged heavy use, their appropriateness as diagnostic criteria for SUDs have been repeatedly criticized from a child and adolescent psychiatric perspective [44, 50, 51].
Cannabis use disorders
With regard to cannabis use disorders the prevalence rates were much lower than the prevalence rates for alcohol. However, this is not surprising. Cannabis is an illegal substance and less available than alcohol in Germany, which is among the countries with the highest per capita consumption of alcohol in the world [52]. Moreover, this finding matches previous results showing that cannabis use disorders are about a factor of 3–5 times less prevalent than alcohol use disorders in Germany [8, 31]. The distribution also reflects non-clinical patterns of use found in this study and as well as in the general population: while 43.6% of adolescents in this sample have used alcohol at least once in their lives, this proportion was only 8.9% for cannabis (these values are largely similar to those reported in federal statistics [53].
However, the picture is different when the prevalence rates are considered only for those adolescents who have actually used the substance within the past 12 months. For this subsample, prevalence rates were much higher for cannabis compared to alcohol use disorders. This suggests that cannabis users are more likely to meet diagnostic criteria for a SUD than alcohol users. This notion corresponds to previous findings indicating that progression from first use towards problematic use is usually faster for cannabis compared to alcohol use [54].
Tobacco and e-cigarette dependence
The prevalence for tobacco cigarette dependence outweighed the prevalence of e-cigarette dependence by far. Moreover, while a comparatively small proportion of past-year e-cigarette users met the diagnostic criteria for dependence, this proportion was about 8 times as large for tobacco cigarettes.
In Germany the spreading of e-cigarettes and associated health risks for children and young people have been of recent concern [55]. Internationally, there has been an increase in e-cigarette use during the past years with evidence indicating that the use of e-cigarettes is associated with increased risks for subsequent initiation of tobacco cigarette use [56, 57]. However, studies comparing the amount dependent users of e-cigarettes vs. cigarettes are missing. Part of the problem in comparing the addictive potentials is that e-cigarettes are not a uniform product and different products with varying doses of nicotine are available (see [58] for an overview).
In our survey, the assessment referred to the use of any form of electronic cigarettes; consumption of different products such as tobacco heaters, e-pipes or “e-hookahs” were not examined. Although this assessment appears rather broad, the present findings nevertheless confirm recent results from France [59] indicating that tobacco use continues to be more problematic than e-cigarette use among adolescents in Europe.
Associations with mindfulness and related factors
Overall, the observed associations largely match with previous findings and added to the explanation of variance in most of the assessed subtypes of SUDs; however, there were similarities and differences between these outcomes. With regard to mindfulness, our findings are comparable in direction and magnitude to meta-analytic associations with use of cigarettes, alcohol and cannabis in population-based samples of adolescents and young adults [27, 60].
Our findings also largely confirm previous studies regarding the role of impulsivity, a multifaceted and central construct in the context of addictive behavior [16]. For our survey-type study, brief assessments of impulsivity and sensation seeking were found to be independently associated with increased risk for SUD of various subtypes. These findings add to existing evidence indicating that both factors contribute independently to risks for substance misuse and can be useful as screening instruments for identifying substance-related problems among adolescents [40, 61]. It should be noted that in our multivariable analyses, mindfulness, impulsivity and sensation seeking as well as dimensions of externalizing (hyperactivity) and internalizing (emotional) problems were correlated but added unique proportions of explained variance for SUD. However, this pattern did not generalize across all different SUD subtypes.
In the additional analyses, the pattern of associations was much more consistent across SUD subtypes and the associations were also typically stronger when assessed separately. For example, stress was substantially correlated with SDQ-dimensions of psychopathology, mindfulness and impulsivity. While stress was not significant in the multivariate models for all outcomes except of cannabis abuse, it was significantly associated across all outcomes in the additional analyses. The associations between impulsivity (to a lesser degree also sensation seeking) and particularly mindfulness were much more consistent and stronger when separate variable associations were assessed.
While multicollinearity between explanatory variables can be problematic in multivariable analyses, the apparent intercorrelations in the present results appear conceptually plausible. In general, SUDs are highly comorbid with other mental problems and share a variety of risk and resilience factors in the spectrum of internalizing and externalizing problems [62, 63]. With regard to mindfulness, impulsivity and emotional and behavioral problems in particular a possible overlap is supported by previous studies [64, 65]. Single and colleagues [28], for example, found that an association between mindfulness and alcohol-related problems was explained by low levels of emotional psychopathology. Other recent research found that dimensions of impulsivity and self-regulation are associated with mindfulness [64]. While in the present study, we explored direct associations of these factors with substance use disorders, the relations between characteristics of mindfulness, impulsivity, sensation seeking, emotional and behavioral problems may include indirect chains of associations and should be examined in more detail in further analyses [65].
Implications and added value of the study
The present study provides a much needed empirical base for estimating treatment needs for the youth population in Germany [50], which have been derived rather indirectly from inadequate data bases. The methodology is largely comparable to existing survey-based research in representative samples from the general population and provides high levels of generalizability. Samples relying on adolescents in school or in treatment may underestimate substance use because they do not include adolescents who have dropped out of school or are in residential care.
The prevalence rates found in this study provide a baseline for future epidemiological studies. Given that patterns of substance use change historically, it is important to monitor trends and changes in prevalence rates to estimate public health demands.
Interestingly, while youth alcohol use in Germany has been decreasing steadily in the past two decades, the proportion of persons who consume alcohol (and other substances) problematically has been rather stable [11, 31]. This observation may inform public health initiatives towards a stronger focus on targeted intervention approaches for those who are at risk to develop substance use disorders. Currently, prevention programs in the context of substance use focus on universal and mostly school-based measures in the general population [66].
Considering the ongoing initiative to legalize recreational use of cannabis for adults in Germany [67], our data may provide a starting point from which future developments in the extent and prevalence of cannabis use disorders can be evaluated. However, it is clear that long-term longitudinal studies are needed for identifying the developmental conditions that play a role for stability and change of substance (ab) use and dependence. Without longitudinal data, we cannot determine the reliability and validity of the questionnaire-based operationalization of substance abuse and dependence criteria. Likewise, it may be possible that social desirability can influence response behavior for cannabis use, since this substance is illegal in Germany.
Moreover, while our DSM-IV-based prevalence rates allow for a high comparability with previous studies [8, 11, 14, 31], they may underestimate the prevalence in comparison with prospective DSM-5-based studies, which apply a lower diagnostic threshold (for a mild disorder). At least this is suggested by recent survey data from the United States that allows for a direct comparison: the prevalence rates for alcohol and cannabis use disorder (aggregated DSM-IV abuse and/or dependence) in the 12–17 age group were 1.7 and 1.8% in the 2019 survey [32] but 2.8 and 4.1% for at least a mild alcohol and cannabis use disorder based on DSM-5 in the 2020 survey [13].
The distinction of two well-defined categorical clinical entities is similar to the ICD-10 and ICD-11 [3] which is applied in the care systems of most European countries, including Germany. However, statements about the diagnostic compatibility with the classification standards of the ICD (ICD-10 and ICD-11) can only be made with caution because of limited availability of data from youth populations and results from adult populations are mixed. Several studies using adult samples suggest a relatively high level of concordance between ICD-10- and DSM-IV-based prevalence rates. In an Australian study [68], there was a high concordance between both classification systems for alcohol and cannabis dependence which was also higher than the compatibility between both DSM versions. Likewise, a large-scale study of over 12,000 adults from general populations in several countries showed very high overlap between ICD-11 dependence diagnoses for alcohol and cannabis with both ICD-10, as well as DSM-IV and (albeit with cutbacks) DSM-5 [69].
Our results show that higher levels of trait mindfulness are associated with a lower likelihood to meet DSM-IV criteria for SUDs. Likewise, we found an inverse relationship of trait mindfulness with other related risk factors for substance use (disorders), such as impulsivity, stress, and symptoms of psychopathology. Given the high comorbidity with emotional and behavioral problems that is frequently associated with adolescent substance use and the transdiagnostic qualities of mindfulness-based interventions [25, 70], such interventions may be promising for youth populations.
Limitations
The generalizability of the study results may be limited because of two issues. First, we lack information about those adolescents who did not participate in the survey. We can, therefore, not rule out a possible selection bias and limitations to sample representativeness. Second, the survey was conducted during the Corona pandemic. At the time of data collection, German school-aged children and adolescents were clearly affected by the restrictions to their usual lives although the estimated turning point in the pandemic and related problems across the federal states in Germany was already passed for about six months [71]. Research on the implications of the COVID-19 pandemic related conditions such as the implementation of social distancing measures on adolescent substance use are mixed: a study from Canada shows that the percentage of young alcohol and cannabis users decreased but the frequency of use of both substances increased. In a cohort-study among ninth- and tenth-grade students in Northern California [72] in contrast found that the overall prevalence of e-cigarette, cannabis, or alcohol use did not meaningfully change with a state-wide stay-at-home order.
Comparable data in youth samples in Germany are not available, but there were increases in psychological stress [38] and SDQ-based mental health problems [73] during COVID-19 lockdown in Germany. Although SDQ-scores and stress were included in the statistical analysis and DSM-IV diagnostic criteria refer to a 12 months’ time frame with the cross-sectional study we are unable to determine whether the burden related to COVID-19 has affected the results.
Finally, it should be noted that the psychometric validity of several measures in this survey study was not optimal. The associations found in this study between the various substance use disorders with stress, impulsivity, sensation seeking, as well as the SDQ-dimensions emotional problems and hyperactivity, although theoretically plausible, should be viewed with some caution.




留言 (0)