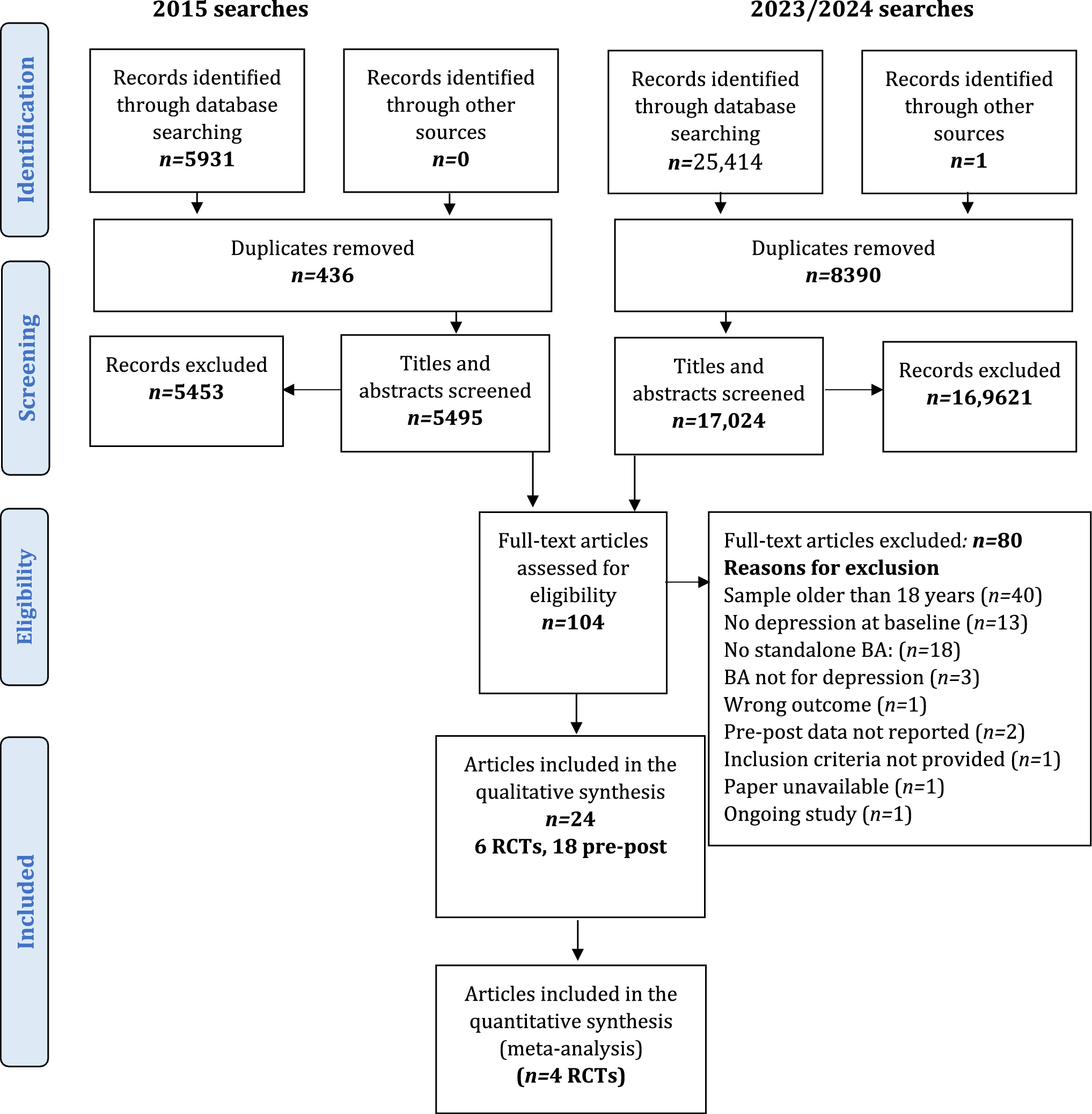
The initial search strategy identified 4507 articles and 613 duplicates were removed. Of the 3894 articles screened by title and abstract, 56 underwent full-text screening, of which 12 were eligible for inclusion. Review of the references in 23 systematic reviews identified no additional articles. Hand searching identified an additional four articles. The updated search in April 2021 identified 734 articles, from which 166 duplicates were removed, and two additional articles were identified for inclusion.
The most common reasons for excluding articles were that participants were aged 18 years or older; we could not separate the results of participants within and outside age criteria; or CBP use was not intended for medical purposes. A total of eighteen articles was included (Fig. 1).
Study characteristics
The 18 included articles were published between 1996 and 2021 and included 310 participants aged 3–18 years. One was an RCT, one was an open-label trial, three were observational studies, two were case series, and eleven were case reports. The articles covered eight neuropsychiatric or neurodevelopmental conditions: ASD (n = 5), TS (n = 3), PTSD (n = 3), FXS (n = 2), Mood Disorders (n = 2), Anxiety Disorder (n = 1), FASD (n = 1) and ID (n = 1). The RCT and open-label trial lasted 8 weeks and 12 weeks, respectively. The duration of the shortest study, a case report, was one week and the longest, also a case report, was 2 years and 5 months. Six studies evaluated the efficacy of cannabidiol (CBD) only, and four evaluated tetrahydrocannabinols (THC) only. The remaining studies evaluated whole cannabis, cannabis extracts or synthesised cannabinoid compounds which typically contained a high ratio of CBD to THC.
Study characteristics, and information on primary outcomes, CBP, efficacy and safety of the eighteen articles are shown in Table 1. Online Resource 2 contains: (i) detailed information for each of the 18 articles (including: participants secondary conditions, CBP administration and dosage, outcome measures, results, completion rates, reasons for termination, concomitant medication and adverse events experienced by participants), (ii) risk of bias and trial quality and (iii) clinical trials in progress. Online Resource 3 provides a summary and quality of evidence of case series and case reports. Online Resource 4 provides a list of the publications that were excluded after full-text review because the results of participants within and outside age criteria could not be separated.
Table 1 Summary of the characteristics, efficacy, and safety for studies of cannabinoid-based products (CBP) in the treatment of neurodevelopmental and neuropsychiatric disorders in children and adolescentsBelow, a brief description of each condition is followed by the evidence from the eighteen included studies and the fourteen relevant forthcoming clinical trials. The findings from the review are presented by condition and include information on the rationale for use of CBP, the evidence by type of CBP, the quality of evidence/risk of bias and a description of active (incomplete) trials.
Autism spectrum disorderRationale
The ECS is thought to play a role in social interaction, emotional responses, and behavioural reactivity in ASD [31]. Findings from ASD mouse models suggest that increasing AEA activity at CB1 improves function in ASD, particularly social interaction [32, 33]. In human studies, children with ASD had lower plasma and serum levels of AEA compared to healthy controls [34, 35]. Together these studies suggest impaired AEA signalling may be involved in the pathophysiology of ASD [36]. CBD, one of the primary cannabinoids in the cannabis plant, inhibits the reuptake and degradation of AEA and hence has the potential to elevate AEA levels [36]. Additionally, a clinical study showed that CB2 is upregulated in peripheral blood mononuclear cells of children with ASD compared to healthy controls and the authors proposed that CB2 is a potential target for ASD treatment [37]. Consequently, the mechanism by which cannabinoids could be used to treat ASD may be through the synthetic modulation of the ECS [38].
A prospective observational study of children and young adults with ASD (n = 53; aged 4–22) suggested CBD could improve hyperactivity, sleep, self-injury, and anxiety. Although efficacy did not differ statistically from conventional treatments (e.g., methylphenidate, melatonin, aripiprazole, selective serotonin reuptake inhibitors), non-inferiority of CBD was observed [39]. A three-arm RCT, compared the efficacy of whole plant cannabis extract (20:1 CBD/THC ratio), pure CBD and pure THC (20:1 ratio) and an oral placebo among children and young adults with ASD (n = 150; aged 5–21) [40]. No severe or serious adverse events were reported, with somnolence being the most reported mild adverse event. This trial suggested that CBD may improve disruptive behaviours in ASD [40]. These two trials were excluded from the current review as they included participants out of the age range.
Evidence in children and adolescents
We identified five published studies evaluating the efficacy of CBP in children and/or adolescents with ASD. These include three before-after observational studies with no control group [41,42,43] and two case reports [44, 45] (Table 1). The symptoms that improved most often across the studies were maladaptive behaviours (e.g., aggression, irritability, and hyperactivity), and core impairments of ASD (social skills, social communication, and repetitive behaviours). Some improvements were noted in sleep, lethargy, anxiety, mood, quality of life, adaptive behaviours, and cognition (Table 1). Adverse effects were mostly mild to moderate and transient. Concomitant medications were reported in four of the five studies, in about two-thirds of the cohort [41,42,43,45] (Online Resource 2).
In the three before-and-after observational studies [41,42,43] and a case report [45] whole plant extracts with high doses of CBD and THC or CBD and THC isolates were used (Table 1). The three observational studies included administration of whole plant extract (n = 60) [41], cannabis oil (n = 188) [42] and cannabis Sativa extract (CE) (n = 18) [43], CBD/THC ratios were: 20:1; 20:1; and 75:1, respectively. Primarily based on standardised caregiver reports, each treatment improved ASD symptoms. Specifically, in the retrospective study in which whole plant extracts were administered for an average of 10 months improvements were reported in behaviour (61%), anxiety (39%) and communication (47%) and these rates were slightly higher when examined in participants with ASD not associated with another diagnoses [41]. In the study in which sublingual cannabis oil (30% CBD, 1.5% THC) was used, more than 80% of parents reported moderate/significant improvement in their child’s global assessment, and significant improvements in quality of life, mood, sleep, and the ability to perform daily activities (e.g. dress and shower independently) [42]. The third study, in which oral capsules of CBD-enriched CE were administered (CBD dose: 3.75–6.45 mg/kg/day; THC dose: 0.05–0.09 mg/kg/day) improvements were reported in more than one of the eight ASD symptoms/signs evaluated: 60–80% of participants had some level of improvement in ADHD, motor deficits, communication and social interaction, cognitive deficits and/or sleep disorders [43] (Table 1 and Online Resource 2). Adverse events reported in these observational studies were mild/transient, the most common being sleep disturbance, restlessness, change in appetite, and nervousness [41,42,43] (Online Resource 2). Despite improvements in ASD symptoms, one case receiving the CE treatment developed worsening psycho-behavioural aspects. This study only reported side effects in children receiving concomitant medication and the authors highlighted the possibility of negative CE-drug interactions, especially among participants taking antipsychotic medications [43] (Table 1 and Online Resource 2). Dropout rates for these observational studies were between 12% and 27%, predominately due to low perceived efficacy and/or adverse events (e.g., insomnia, irritability, worsening psycho-behavioural crisis, and/or increased heart rate [43]) (Online Resource 2). The case report is described in Online Resource 3.
See Online Resource 3 for a summary of the case report that trialled Delta-9-tetrahydrocannabinol (THC) [44].
Quality of evidence/risk of bias
The five studies were uncontrolled; the assessors were typically parents and treating physicians and were not blinded to the intervention, which increased the risk of bias. Previous studies suggest 20–50% of parents report a positive response when their child with ASD receives a placebo [46], so findings from uncontrolled studies must be interpreted with caution. There were considerably more males than females in each study, which fits with the gender ratio in ASD but makes the findings difficult to generalise to females. Outcomes and outcome measures varied widely across the studies and standardised assessment tools were not always used, making it difficult to compare findings between studies or conduct meta-analyses. There was also variability in the cannabinoid strain used, e.g., THC, CBD. A potential conflict of interest was reported in one study [42] and was unclear in another [44].
Although these preliminary studies suggest CBP might improve some ASD symptoms, the high risk of bias in the five studies (Online Resource 2) indicate the need for RCTs.
Active clinical trials
Seven clinical trials (RCT (n = 4), open-label (n = 3)) are underway in Australia (n = 2) and the USA (n = 5) to assess the efficacy of CBP among children and/or adolescents with ASD (Online Resource 2).
Intellectual disabilityRationale
About 40% of children with ID experience severe emotional and behavioural problems, including irritability, aggression, and self-injurious behaviour. Anxiety is a driver of severe behavioural problem in individuals with ID and CBD has anxiolytic effects [47, 48]. However, it is not known whether ID is associated with alterations in the ECS. There is growing interest from parents of children with ID to determine whether CBP can reduce behaviour problems in children and adolescents with ID [49, 50].
Evidence in children and adolescents
An 8-week, double-blind, placebo-controlled, parallel-group, RCT was piloted to investigate the feasibility of the protocol for evaluating CBD in children and adolescents with ID and severe behavioural problems (n = 8, aged 8–16 years old) [50] (Table 1). The treatment group received CBD oil (maintenance dose of 20 mg/kg/day, with a ceiling dose of 1000 mg/day). Outcome measures included the Aberrant Behaviour Checklist—Irritability subscale (ABC-I, primary outcome); Child & Adolescent Scale of Participation; Child Health Utility 9D; Sleep Disturbance Scale for Children; Adult Quality of Life Total; Beach Center Family Quality of Life Depression Anxiety Stress Scale; and Autism Parenting Stress Index and were completed in the treatment (n = 3) and placebo (n = 4) groups (Online Resource 2). An efficacy signal was found on the ABC-I in favour of CBP treatment. Using the Monitoring of Side Effects Scale (MOSES), some minor adverse effects were experienced by participants in both groups (e.g. abdominal pain, constipation, tinnitus, restlessness, drowsiness), but no severe adverse events were reported [50] (Online Resource 2). For future trials the authors suggested use of a measure that focuses on common adverse events seen with cannabis/CBD for medical use instead of the MOSES; a decrease in the number of outcome assessments, laboratory tests and study visits; and flexibility for parents to complete some of the questionnaires at home.
Quality of evidence/risk of bias
There was a low risk of bias in the pilot RCT design. However, the sample size was too small to evaluate the significance of the positive signal for CBD. Also, all participants randomised into the CBD group had ASD compared to only one of four in the placebo group and the primary outcome measure was designed to assess behaviours in people with ASD (Online Resource 2).
Active clinical trials
A multi-site, double-blind, parallel-group, RCT to extend the pilot [50] is underway in Australia to evaluate the efficacy of CBD isolate in oral solution in reducing severe behavioural problems among children/adolescents with ID (Online Resource 2).
Fragile X syndromeRationale
FXS is caused by a mutation of the fragile X Messenger Ribonucleoprotein 1 gene (FMR1), resulting in absent or reduced production of the protein FMRP which is required for brain development. FMR1 knock-out mice have the same symptoms as people with FXS. Studies with these mice suggest that reduced expression of FMR1 dysregulates the ECS and disrupts the excitatory and inhibitory neurotransmission balance via the post synaptic release of endogenous cannabinoids, AEA and 2-AG, that stimulate CB1 receptors that occur throughout the CNS [51,52,53]. It is thought that CBD may help restore the excitatory and inhibitory balance by increasing AEA and 2-AG availability [52,53,54,55]. Two case reports in adults with FXS demonstrated reductions in anxiety and social avoidance and improvements in sleep, feeding, motor coordination and language skills following oral administration of CBD-enriched (CBD+) solutions [56]. However, these case reports relied on parental reports, did not include control groups and, include inconsistencies in the quality, purity, and administration of CBD, making it challenging to reach conclusions [56].
Evidence in children and adolescents
One uncontrolled, open-label, before-and-after trial [57] and a case report [56] suggest that CBD may benefit children and adolescents with FXS (Table 1). The 12-week open-label multi-site trial, which administered transdermal CBD gel (50 mg/day (n = 1); 100 mg/day (n = 3); 250 mg/day (n = 16)) to 20 children (aged 6–17 years), reported a significant reduction in anxiety and behaviour symptoms. The Anxiety, Depression and Mood Scale (primary outcome) showed statistically significant reductions in the mean total score and several subscales (manic/hyperactive behaviour, social avoidance, general anxiety, and compulsive behaviour) from screening to week 12. No improvement was found on the depressed mood subscale. Several secondary measures also reported significant reductions in mean scores—The Aberrant Behavior Checklist—Community for FXS: Clinical Global Impression Scale—Severity and Improvement; The Pediatric Quality of Life Inventory; The Pediatric Anxiety Rating Scale; and three Visual Analogue Scales, hyperactivity/impulsivity, tantrum/mood liability, and anxiety (Online Resource 2). Two of the twenty participants withdrew from the study on day 63 (dose: 100 mg/day) and day 64 (dose: 50 mg/day). These participants were siblings: one withdrew due to adverse effects, worsening pre-existing eczema, and the other withdrew for administrative reasons. Seventeen of the twenty participants (85%) reported at least one adverse event, the most common being: gastroenteritis (n = 5), disorders at the application site (n = 2), vomiting (n = 2) and upper respiratory tract infection (n = 2). No serious adverse events were reported [57] (Online Resource 2). See Online Resource 3 for a summary of the case report.
Quality of evidence/risk of bias
The two studies that examined the efficacy of CBP in FXS both used CBD; however, the open-label trial used a transdermal gel, and the case report used an oral paste. Both studies were uncontrolled, and assessors were not blind to the intervention, which increased the risk of bias (Online Resource 2). There were no other quality concerns with the before-and-after trial. See Online Resource 3 for a summary and quality of evidence of the case report.
Active clinical trials
Two active clinical trials are evaluating the efficacy of ZYN002, a transdermal CBD gel, for treatment of FXS. The first is an extension of the uncontrolled open-label before-and-after trial discussed above [57], intended to evaluate the long-term safety and tolerability of ZYN002 in children with FXS. The second trial is a phase 3 multicentre RCT using the same CBD product and similar dose that will be conducted by the same authors and funded by Zynerba Pharmaceuticals (Online Resource 2).
Mood disordersRationale
Depression, mania, and bipolar spectrum disorders are conditions for which novel treatments are in demand, especially when there are recurrent or refractory episodes of illness. The role of the ECS has been studied using a knock-out mouse model. Absence of the CB1 gene results in deficiency of CB1 receptor signalling and aggressive behaviour and an anhedonic state in the mice, both of which are core depressive symptoms in human adolescents [58]. In humans, antagonism at CB1 receptors with rimonabant (an inverse agonist of CB1) is associated with depressive symptoms in adult humans [59]. The antidepressant effect of CBD may involve a CB1-mediated increase in serotonin levels involving the 5HT1A receptor [60, 61].
Clinical practice guidelines for the assessment and treatment of mood disorders note that the evidence for efficacy of CBD in depression remains unproven [62]. Cross-sectional studies in Australia [63] and the USA [64] suggest a sizeable proportion of adults self-medicate with CBD to treat their depression, despite unproven efficacy [65, 66]. CBD was deemed ineffective in two manic patients, one of whom received adjunctive olanzapine [67]. Two small-scale controlled trials (n = 8; n = 13) conducted in the 1970s did not find significant effects of THC on depressive symptoms among individuals with unipolar and bipolar depressive disorders [68]. One double-blind placebo-controlled cross-over trial of THC in 34 patients with cancer reported improvements in depression. However, this study had methodological limitations and confounding effects of cancer.
Evidence in children and adolescents
There is no RCT, one case series [69], and one case report [70] evaluating the efficacy of CBP for mood disorders in children (Table 1). See Online Resource 3 for a summary of these reports.
Quality of evidence/risk of bias
The case series and case report offer no evidence for the efficacy of CBP in improving mood disorder symptoms (Online Resource 2). See Online Resource 3 for a review of the quality of evidence of these reports.
Active clinical trials
A phase 2, double-blind, randomised placebo-controlled trial was registered in Australia in 2016 to examine the safety and efficacy of CBD capsules in managing mood disorders in males aged 6–26 years old who use cannabis (Online Resource 2).
Anxiety disordersRationale
About half of cannabis users in the general population report using cannabis for anxiety [48]. Systematic reviews of animal and human studies evaluating CBD (and THC) as potential treatments for anxiety disorders [28, 47, 48, 71,72,73] suggest that CBD is anxiolytic, and THC is anxiogenic [47, 48, 71,72,73]. Although it is thought that lower doses of THC are anxiolytic, higher doses are anxiogenic [48]. The dose–response for CBD appears to follow a bell-shaped curve, with less effective results at lower and higher doses [47, 72]. CB1 receptors, 5-HT1A receptors and TRPV1 receptors are likely mediators of CBD’s anxiolytic effects [47, 72, 73]. The ineffectiveness at higher dosage may be due to activation of TRPV1 receptors, which have anxiogenic effects [47]. The anxiogenic-like effects of THC diminish when CBD is co-administered with THC, suggesting that CBD alleviates some of THC’s anxiogenic-like effects [




留言 (0)