
記住我





We developed a comprehensive implementation package known as the Playbook. The Playbook is a web-based platform that supports the development of new clinic-community partnerships by providing training activities, a formal blueprint for building the partnership and Fit Together program, and all the curricular materials needed to implement the Fit Together intervention. The Playbook utilizes written, video, and audio formats, and includes supporting materials such as checklists, templates for required contracts and forms, and self-assessment components. The development of the Playbook was informed by the paper-based implementation materials and lessons learned in the ARCHES pilot study [19]. Additionally, to ensure that the Playbook balances fidelity to evidence-based treatment recommendations with adaptability to the local context, it was reviewed by several advisory groups with expertise in implementation science, community programming, pediatric obesity treatment, and public policy.
The Playbook contains four units: (1) Fit Together Overview, (2) Learning Modules, (3) Partner Checklist, and (4) Fit Together Connector Guide. A detailed description of each unit is provided in Supplementary Table 1. All partners, including clinical staff, community members, and connectors, are asked to work through the online Playbook modules at their own pace, estimating time to completion of about 10 h.
Briefly, the Fit Together Overview (Unit 1) is intended to introduce partners to the clinic-community partnership; describe the shared mission, vision, and goals; and provide the history of the Fit Together program. The Learning Modules (Unit 2) provide partners with the necessary training to create a stigma-free environment for children with obesity and provide effective care to empower families throughout the treatment process. Specific trainings include education on weight bias and stigma, motivational interviewing techniques, nutrition and physical activity, and mental health and eating disorders. The Partner Checklist (Unit 3) is designed to serve as a blueprint for Fit Together, guiding partners through the steps needed to build the partnership and start their Fit Together program. Activities include guidance on completing all of the necessary contracts and agreements (e.g., shared use or data sharing agreement) between the clinic and community sites, hiring and training the connector, developing the referral process, and planning how to use the community space. Additionally, partners are provided with suggested timing for each step, specific action items to complete each step, and recommended meeting times and topics to foster communication. The Fit Together Connector Guide (Unit 4) serves as a resource for the connector to help plan and run the Fit Together community program. The Connector Guide provides guidance on finding staff and volunteers, contacting families and conducting new participant orientation sessions, planning a Fit Together session, and all the logistical considerations associated with running a community program. Finally, in addition to the four units, the Playbook contains a resource section that includes documents and templates needed as part of the Fit Together program (e.g., shared used agreement template, sample connector job description, Fit Together flyers and brochures, and nutrition education curriculum).
Other implementation supportIn addition to the Playbook, partnerships have access to several other implementation supports.
Childhood obesity coaches. The AAP Institute for a Healthy Childhood Weight supports a network of experts (“coaches”) available to help local pediatric healthcare providers address obesity in their practices. Leveraging this existing network, Fit Together identified one AAP coach for each site. The coach participates in the training and is available to provide consultation on specific patients who may have medical causes or consequences of obesity.
Fit Together mobile application. Prior data have demonstrated greater engagement and attendance when families are connected through a mobile device [21]. To help partnerships manage their Fit Together program, and to provide this connectivity directly with families through mobile technology, we have developed an app specifically for Fit Together, in partnership with a third-party vendor, Pattern Health. The Fit Together app provides connectors with a digital tool to track attendance, send messages to families, push out program content, and run a Fit Together incentive program. The Fit Together app also includes the opportunity for children to track steps, set and achieve goals, and earn rewards for positive health behaviors, such as program-branded materials (e.g., water bottles, t-shirts) or fitness equipment.
Support for sites and families. We have created a public-facing website to provide onboarding and ongoing technical support to local teams, information for new sites who would like to start a Fit Together program in their community, information for families on how to find a Fit Together program, and general nutrition and activity resources for children.
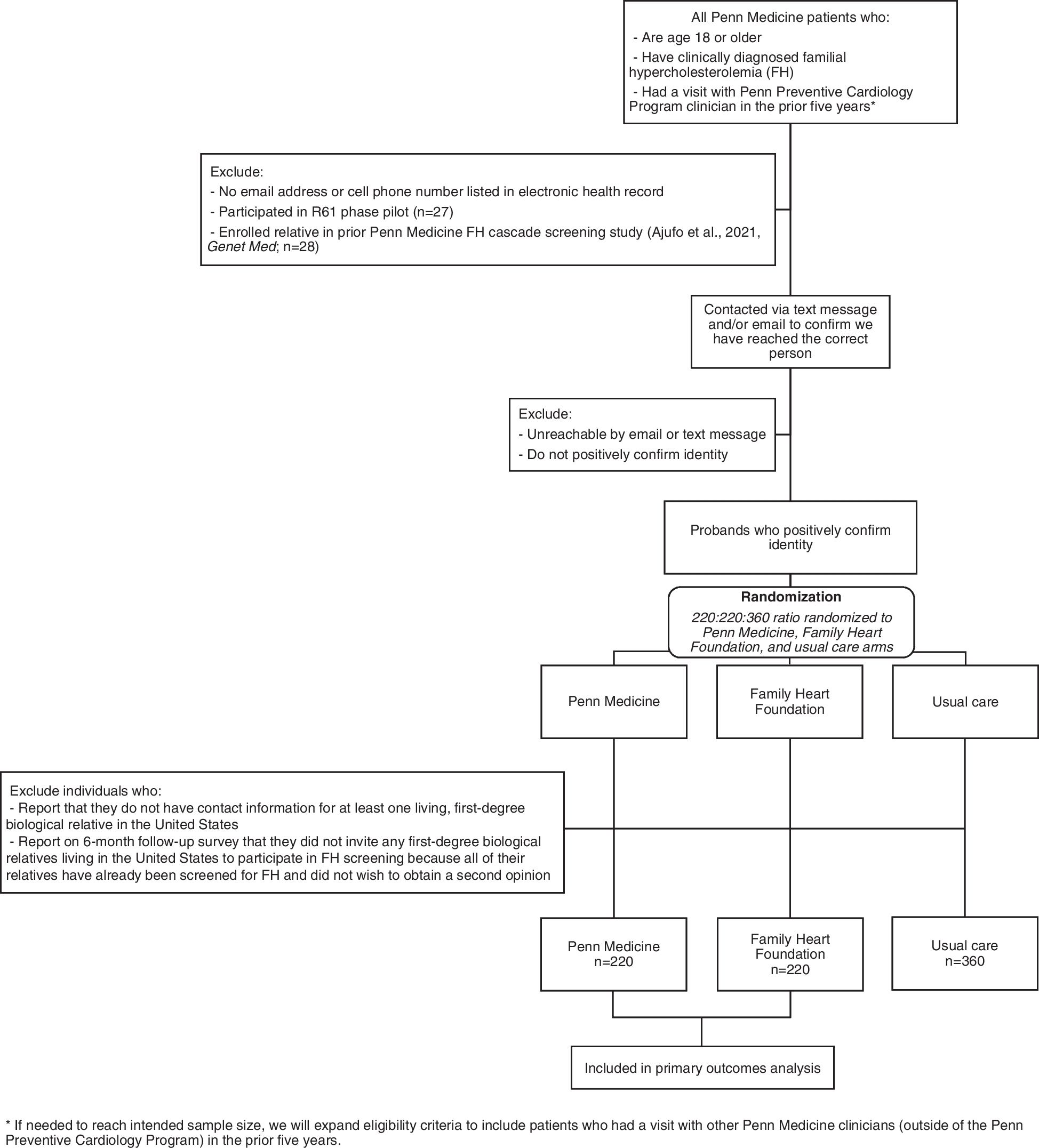
Study designA hybrid type II design will be used to evaluate the implementation strategy and to demonstrate the individual-level effectiveness of the Fit Together intervention [24]. Implementation assessment will be guided by The Process Redesign Framework [25]. Embedded within this framework will be a multi-group interrupted time series design for assessment of individual level outcomes. Because both the utility of the implementation strategy and clinical effectiveness are necessary for the development of a comprehensive dissemination and sustainability strategy, they are considered co-primary objectives. Figure 1 shows the study flow. All protocols have been reviewed and approved by the Duke University Health System Institutional Review Board (Pro00106453).
Fig. 1
Study flow including planning, participant enrollment, and intervention delivery
Setting, participants, and recruitmentThis implementation study will take place in two North Carolina counties, representing large, urban population centers, and areas with high rates of obesity and cardiovascular disease. Within each of these two locations, we have recruited pediatric clinics to deliver the clinical component of Fit Together (n=3) and serve as comparisons (n=2), and Parks and Recreation facilities (n=2) to provide space to deliver the community program.
For implementation measures, we will include all Fit Together partners from each site including pediatric providers and clinic staff, Parks and Recreation leadership and staff, and the connector. Partners will be recruited once each clinic-community partnership begins to use the Playbook. The only inclusion criteria for these individuals are that they are employed by a participating organization, are involved to some degree with the implementation of Fit Together, and can speak English or Spanish.
For effective outcomes, pediatric patients and a caregiver will be recruited through pediatric offices. At well-child visits, pediatric providers will screen children for obesity and refer eligible children to the Fit Together program or the comparison condition using the clinic’s referral process. A member of the research team will contact interested families and enroll them in the study. Then, the connector will contact families to provide additional information about the program and invite them to a new participant orientation session. To be eligible to participate in Fit Together, patients must be between the ages of 6–11 years at the time of enrollment with a BMI ≥ 95th percentile for age and sex, but less than 160% of the 95th percentile. Only children with obesity (not overweight) will be enrolled because the evidence-based model has demonstrated effectiveness only in this group and an important component of the program is that “other children look like me.” Those with a BMI above 160% of the 95th percentile (the most severe obesity) will be referred to a tertiary care weight management program for more intensive treatment. For caregivers to be eligible, they must be 18 years or older, speak English or Spanish, anticipate bringing the child to the program a majority of the time, have no plans to leave the area within the next 12 months, have a smartphone, and be willing to download the apps used in the study for the duration of participation. Although siblings may participate in Fit Together, only the first referred child will be included in the study.
InterventionSites will implement the Fit Together intervention (described above). Providers in intervention clinics will screen children for obesity, refer them to the community program, and provide medical care appropriate for a child with obesity. Children and families will have the opportunity to participate in the community program for up to 1 year.
ComparisonPatients from non-intervention clinics in the same geographic areas will serve as comparisons for individual-level outcomes. Although intervention and comparison clinics may differ somewhat, the interrupted time series design measures trajectory change, and thus provides robust evidence in the context of an implementation study. Qualifying patients who receive primary care at one of the comparison clinics will be given printed materials monthly in the form of a cooking magazine and the local parks and recreation organization newsletter and program guide. Previous studies have demonstrated that this level of intervention is not expected to result in any appreciable weight changes [26].
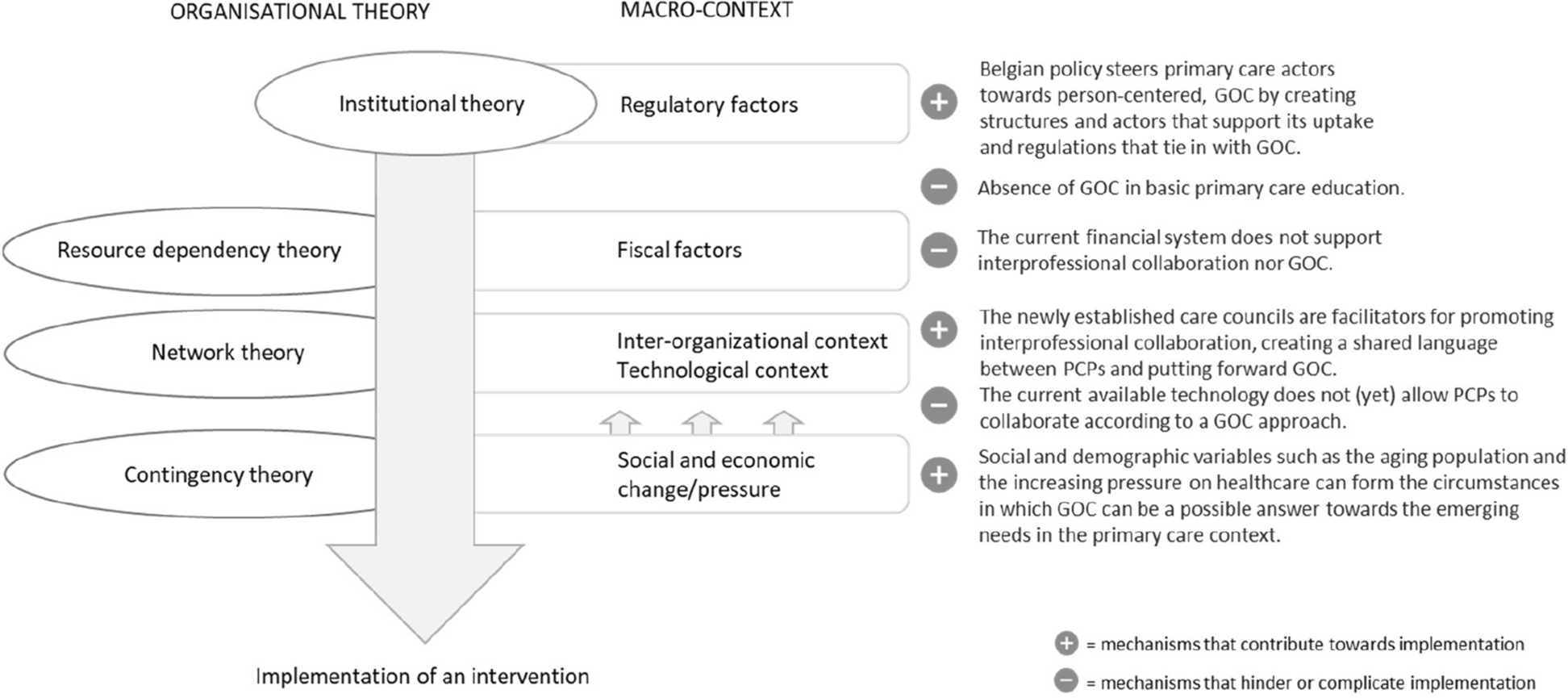
Process redesign frameworkThe Process Redesign Framework was selected to guide the evaluation of the implementation of Fit Together. This framework provides a way to re-conceptualize how care is delivered and is especially relevant when interventions are complex and implementation is likely to challenge current practices and roles [25]. It was adapted from the Consolidated Framework for Implementation Research (CFIR), retaining the domains and constructs in CFIR, while adding additional domains and constructs relevant to process redesign. Similar to CFIR, the Process Redesign Framework provides a menu of constructs for users to select from to guide the evaluation of implementation. Table 1 shows the domains and relevant constructs from the Process Redesign Framework along with the specific measures that will be used to evaluate the implementation of Fit Together.
Table 1 Measurement strategy for implementation study by the component of the Process Redesign FrameworkImplementation measuresQualitative measures
Semi-structured interviews and focus groups will be conducted with clinical and community partners 3 months after each site begins implementation of their Fit Together program and will then be conducted annually. Interviews and focus groups will be conducted following the completion of quantitative implementation surveys. Qualitative measures will examine in-depth information about barriers and facilitators to implementation, attitudes, and experiences with the implementation processes, perceptions regarding the intervention adaptability for their local context, and external factors that may affect the implementation of Fit Together (Table 1). Semi-structured guides will be developed for each stage of the project by experts in implementation science using existing interview questions developed to assess CFIR constructs as a guide [31]. Additionally, meeting notes and recordings and document artifacts (e.g., emails) will also be collected.
Quantitative measures
Self-reported surveys completed by partners will be used to assess several constructs within the Process Redesign Framework (Table 1). Survey items are drawn from existing scales including the perceived Characteristics of Intervention Scale, CFIR Inner Setting Scale, Implementation Climate Scale, Implementation Leadership Scale, Acceptability of Intervention Measure, Intervention Appropriateness Measure, Feasibility of Intervention Measure, and the Program Sustainability Assessment Tool [27,28,29,30, 33, 35]. Surveys will be completed 3 months following the start of program implementation and will then be conducted annually. To assess the fidelity of the Fit Together community program, structured observations of a subset of program sessions will be conducted throughout the delivery of the community program using the System for Observing Play and Leisure Activity in Youth (SOPLAY). SOPLAY is an observational tool that employs momentary time sampling techniques to systematically document individual (i.e., physical activity levels) and contextual factors (i.e., types of activities) [34]. To assess the reach of Fit Together, referral, enrollment, and attendance data will be collected from the clinics and community sites continuously.
Effectiveness measuresPrimary outcome
The primary measure of effectiveness will be changed in the child’s BMI at 12 months, defined as the change in BMI relative to the 95th percentile for age and sex (BMIp95). Because all participants will be above the 95th percentile, this measure is a better reflection of change compared to other measures of BMI (i.e., BMI percentile and BMI z-score) [40]. Child height, weight, and age at the time of measurement will be extracted from patient medical records at baseline, 6 and 12 months, stored securely in REDCap and used to calculate BMIp95 based on the Centers of Disease Control and Prevention SAS code [41].
Secondary outcomes
Secondary outcomes include children’s objectively measured physical activity and the proportion of children meeting treatment guidelines of ≥26 h of treatment over 6 months. These outcomes will be collected throughout the duration of the study. At baseline, children will receive a Garmin Vivo Fit 4 (Garmin International) to be worn for the duration of the study. Participants will be prompted to synchronize their Garmin device periodically and data will be retrieved from the online platform. Physical activity outcomes include steps and active minutes. To calculate treatment hours, medical visits will be documented from the electronic health record and attendance at the community program will be tracked using the Fit Together app that sites will have access to as part of the implementation support. Additional effectiveness outcomes assessed at baseline, 6 and 12 months include other clinical measures (i.e., blood pressure), dietary behaviors, self-reported physical activity, parent-reported quality of life, social drivers of health, mental health, and assessments of harm [36,37,38,39, 42, 43].
Power calculationPower calculations were based on patient-level change in BMIp95. Using data from the National Health and Nutrition Examination Survey, the population mean (SD) for those above the 95th percentile is 117.5 (15.9). Based on the three time points (baseline, 6 months, 12 months), 80% power, and an alpha of 0.05 for a two-sided test, we calculated the required sample size per arm across various plausible standardized differences and a within-subject intra-class correlation coefficient (ICC) of 0.7. Assuming a within-subject ICC of 0.7, we have 80% power to detect a 0.4 standardized decrease (6.98 points) in BMIp95 with 152 subjects retained at 12 months. There are few studies defining clinically meaningful change in BMIp95; however, a 5% reduction in BMIp95 is associated with reductions in cardiovascular disease risk factors [44].
AnalysisFor implementation analyses, there will be a relatively small sample size from the clinics and community sites; thus, no formal hypothesis testing will be conducted. Quantitative measures will be described using means (SD) for continuous outcomes and frequencies and percentages for categorical outcomes. All interviews and focus groups will be audio-recorded and transcribed verbatim. Transcripts will be analyzed using both deductive and inductive thematic analysis [45].
For participant-level analyses, demographic and clinical characteristics of patients at enrollment will be described by clinic site and by intervention assignment using means (SD) and medians (Q1, Q3) for continuous variables, and frequencies and percentages for categorical variables. Group-level differences will be evaluated as appropriate using Student’s t tests, ANOVA, and Kruskal-Wallis testing. The effect of the intervention on clinical outcomes including the patient’s BMIp95 will be evaluated using a clustered interrupted time series approach. The rate and magnitude of change in an individual’s clinical measurement over the study period will be assessed using repeated measures mixed modeling approach. All analyses will include a clustering term for the clinic attended, a variable for assignment to the intervention group, and a time-dependent indicator variable signaling whether a visit occurred in the pre-intervention period versus the post-intervention period. This indicator allows for the detection of differences in the rate of change between the groups once the intervention begins. We will conduct unadjusted intention-to-treat analyses where all patients assigned to an intervention clinic are considered exposed to the intervention. Additional analyses will control for patient-level covariates including patient age, sex, race/ethnicity, and initial BMI.
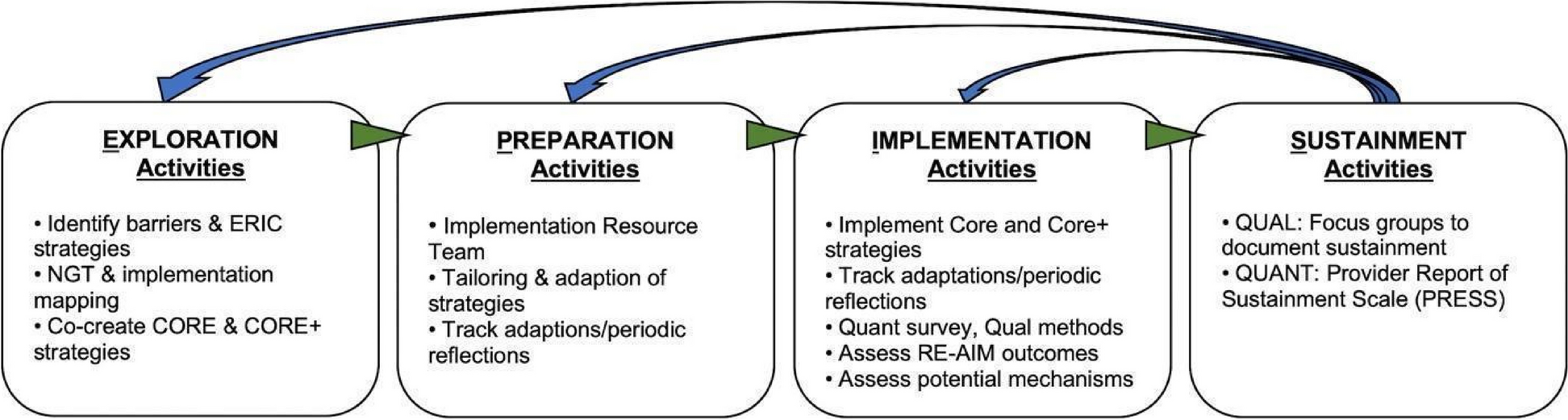
Dissemination strategyGiven the limited availability of pediatric obesity treatment, a dissemination plan will be developed to identify the ideal ways to ensure the widespread availability of Fit Together. The PCORI Dissemination Framework will be used to develop and actively implement a dissemination strategy that delivers the Fit Together intervention and implementation strategy through professional and policy channels, community stakeholders (e.g., Parks and Recreation and health care organizations), and academic venues [46]. Each step of the PCORI Dissemination Framework and the strategies used for each step in Fit Together is shown in Fig. 2. Briefly, we will engage partners at each of our sites as well as policy and dissemination and implementation advisory groups throughout the study to ensure a plan for sustainability (step 1). The advisory groups will assist in the development of the remaining strategies including the identification of appropriate targets and needs for dissemination, refining the goals for dissemination, and using study findings to tailor components of the implementation strategy for other communities (steps 2-4). Using Rogers’s Diffusion of Innovation of Theory, we will create reports appropriate for all stakeholders demonstrating each component of the model: relative advantage (advantage over other treatments), compatibility (compatibility with current processes), complexity (Playbook provides step by step guide), trialability (ability to “try out” program before making long-term commitment), and observability (outcomes can be easily observed through tools in the Playbook) (step 5) [47]. Following the completion of the study, the Playbook will be made available to the public as a web-based resource and shared with relevant organizations such as the National Parks and Recreation Association and the American Academy of Pediatrics (step 6). Finally, dissemination tactics will be adapted and expanded upon based on findings from the implementation study in order to facilitate widespread dissemination (step 7).
Fig. 2
PCORI dissemination framework
留言 (0)