
記住我
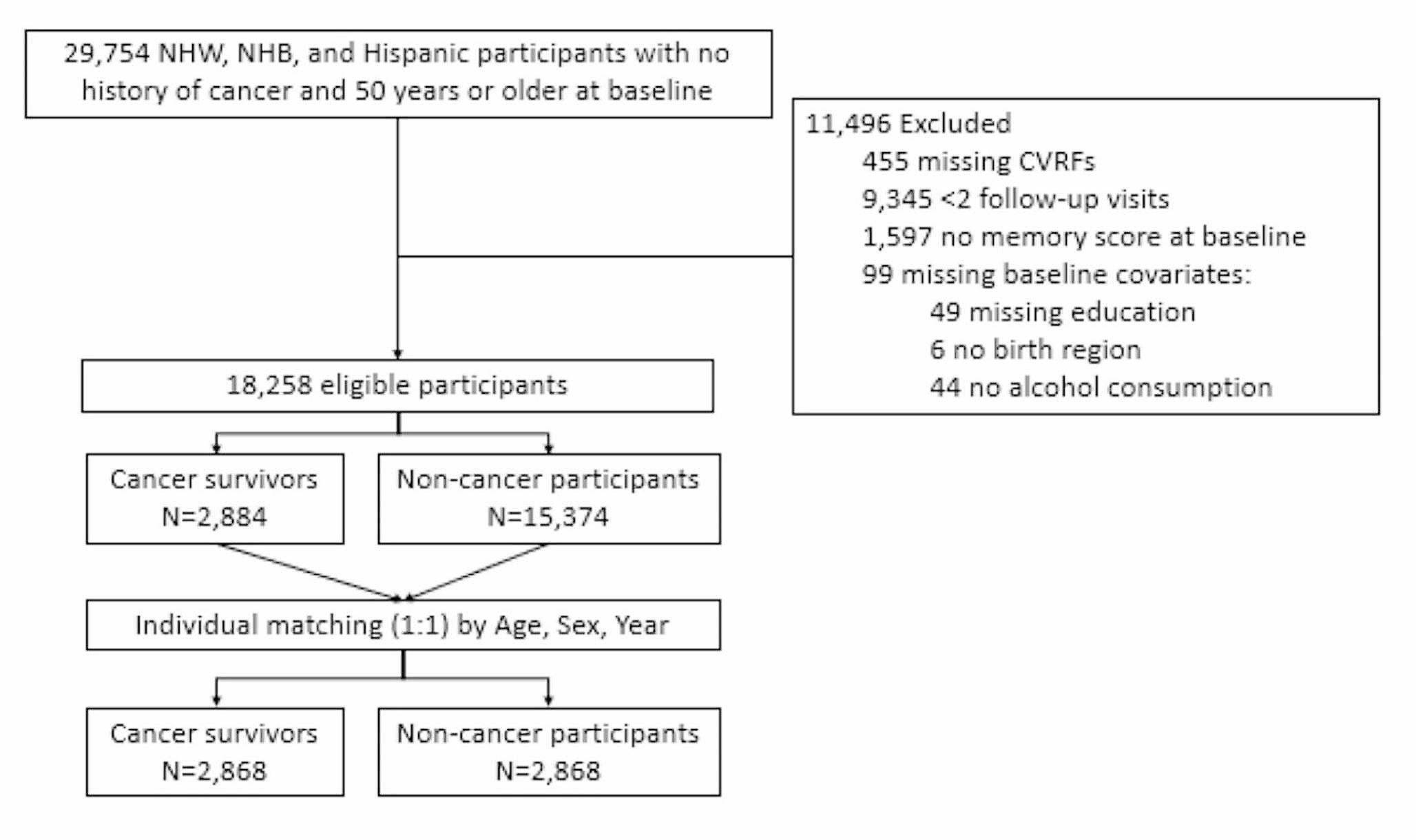


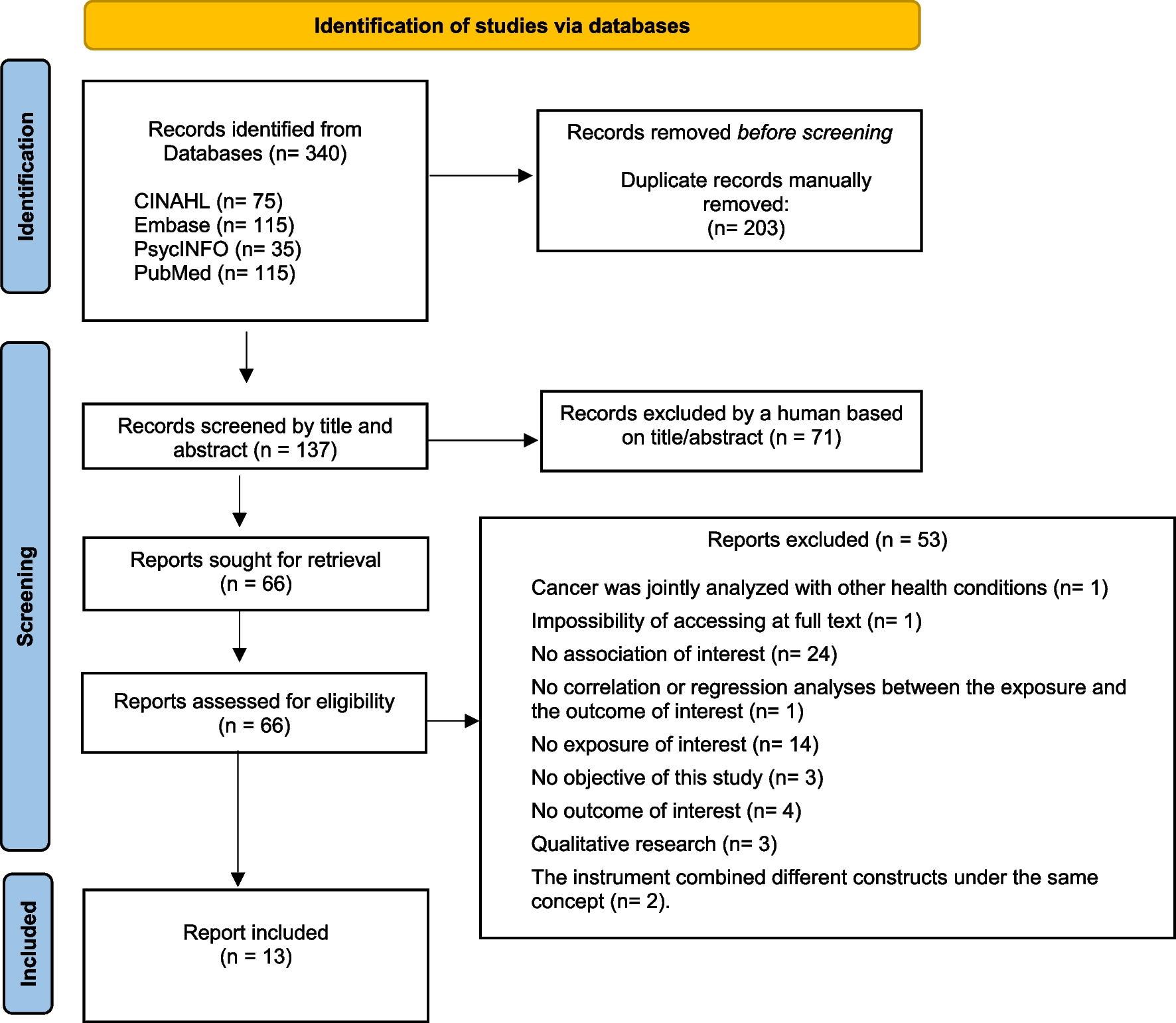
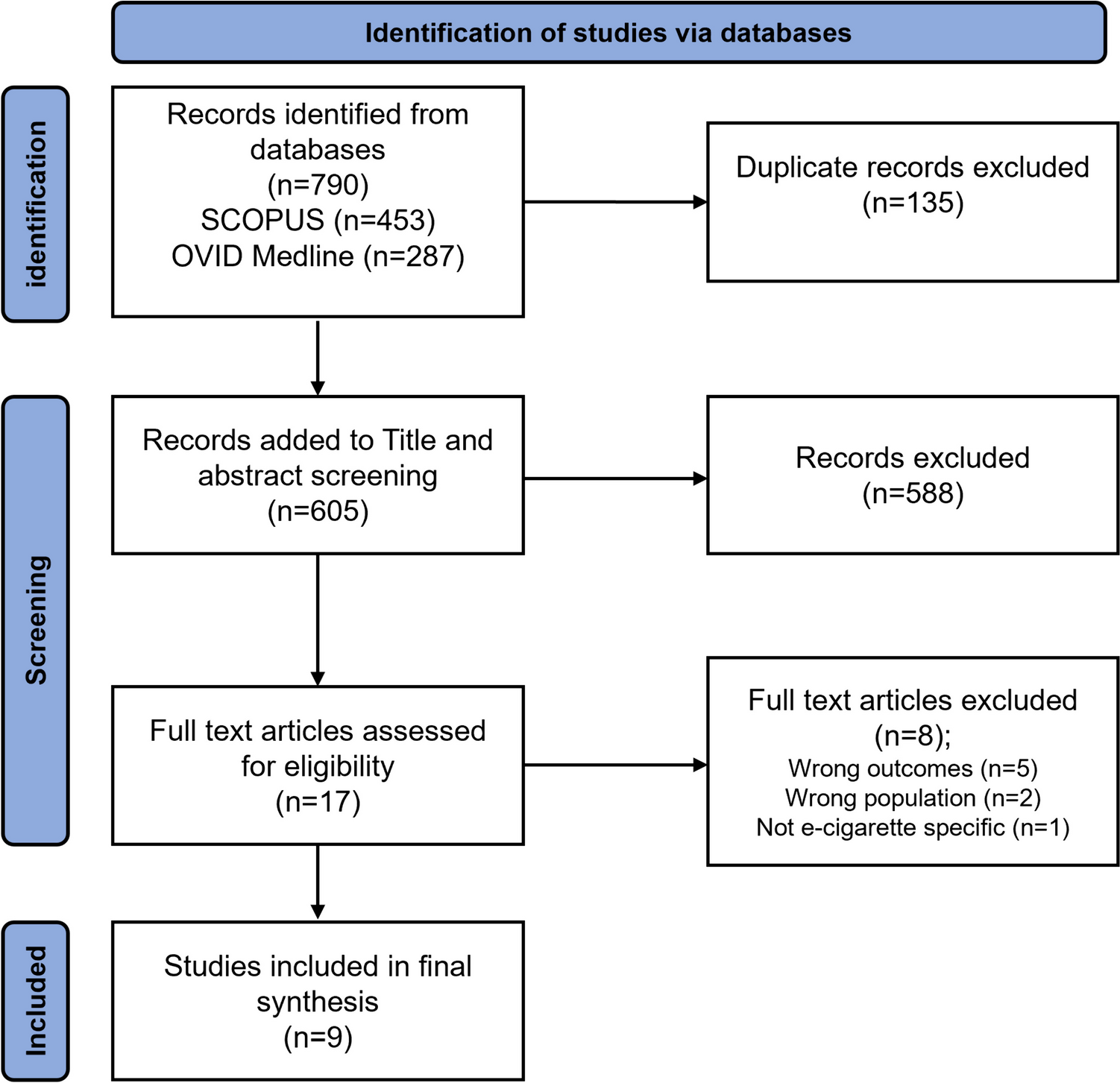
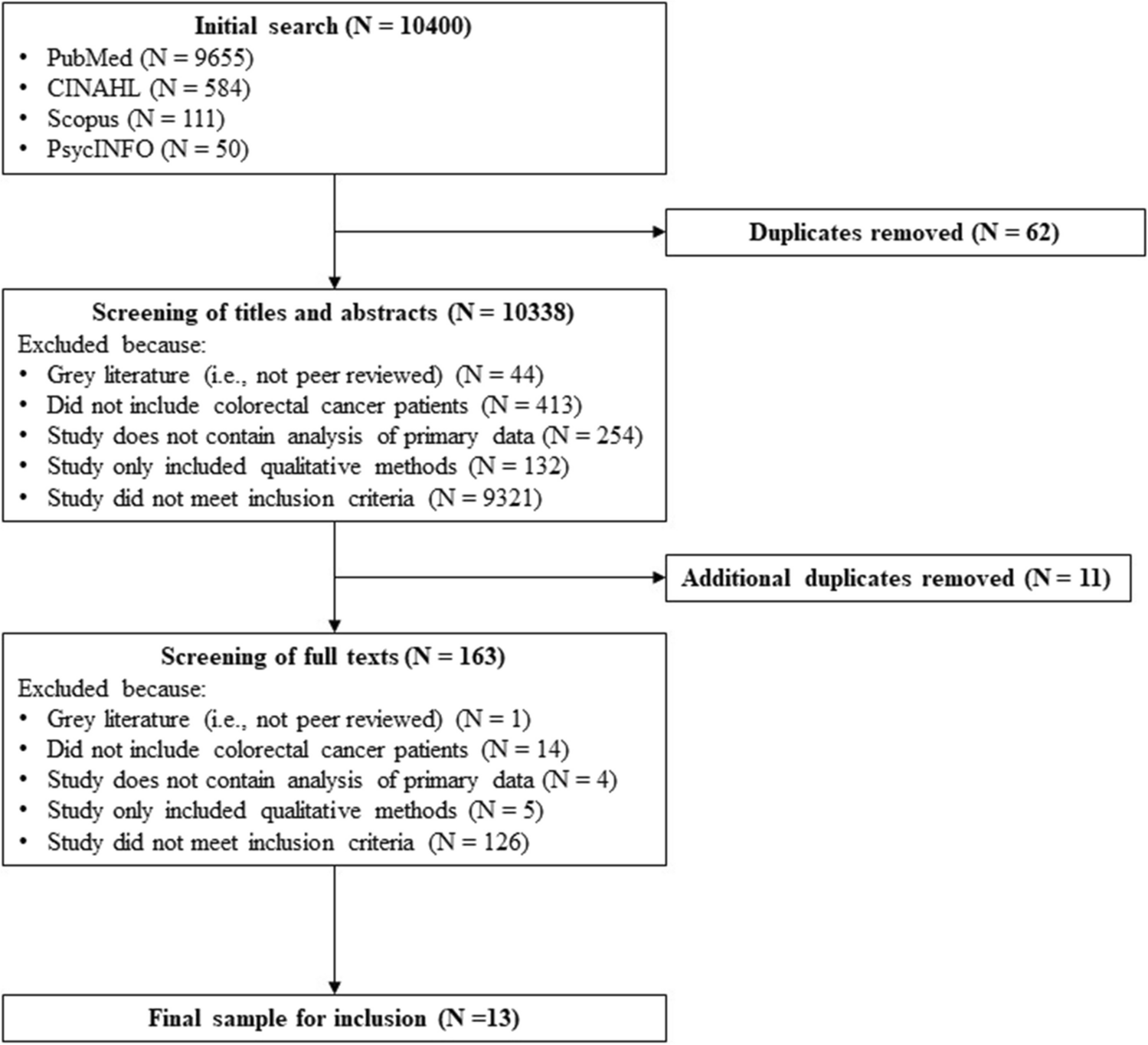
The search strategy generated 1954 articles. After removing duplicates, reviewing titles and abstracts, 39 articles were read in full. Twenty-four studies were excluded for reasons listed in Fig. 1. Fifteen studies from the databases and a further four studies through manual searching were identified as meeting the inclusion criteria. No studies were identified through Open Grey search. In total, 19 studies were included in the review involving 1,538 patients who had CIPN or were at high risk of developing CIPN. Six studies evaluated seven behavioural interventions (BIs) and 13 evaluated exercise interventions (EIs). The study selection process and results are illustrated in Fig. 1.
Fig. 1
PRISMA flowchart of study selection
Quality appraisalOverall, four of the 19 studies were rated as methodologically strong, ten as moderate and five as weak (see Online Material S-2). Earlier studies which explored exercise interventions were noted to be weak; more recent studies were mostly methodologically moderate. Regarding patient selection bias, only two studies were rated weak, while the remainder were rated mainly moderate (n=13) or strong (n=4). Confounders were controlled for most studies (n=13). For blinding, only one study was ranked strong. In the remaining studies, either the blinding process was not explained, outcome assessors were aware of the exposure status of the participant or participants were aware of the research question. Reliable and valid outcome measures were used in most studies. Regarding dropouts, seven studies had a rate of less than 20%, and were, therefore, rated as strong.
The quality of reporting of interventions was variable when assessed against the TIDieR checklist [28]. Three BI studies reported adherence in percentages but only one [13] elaborated on factors which affected adherence. Planned and actual assessment of fidelity were reported only by one EI study [50]. All remaining studies either did not report or insufficiently reported details about fidelity and adherence.
Study characteristicsAll studies included in this review were approved by ethics committees and obtained consent from study participants. A summary of characteristics of all included studies is presented in Table 1.
Table 1 Summary of characteristics of included studies involving interventionsBehavioural studiesAll BI studies originated from United States of America (USA) and participants (n=795) were recruited from outpatient chemotherapy units in various cancer centres. The six studies evaluated seven BIs. One study had a sample size of less than 20 [52]; all other studies had treatment group sample sizes between 30 and 100. Four BIs with 515 participants were delivered during chemotherapy treatment [11, 51, 52, 54]. One BI with 60 participants was delivered after treatment [53] and only one BI with 220 participants was delivered before, during and up to 2–4 weeks after treatment [13]. Only one study focussed on one CIPN symptom, i.e. pain [53]. Three studies were sub-analyses of interventions for multiple chemotherapy side effects including CIPN [13, 51, 54]; one study compared two behavioural interventions for breast cancer treatment symptoms including CIPN [51]. Four BI studies were RCTs, one was a single-arm pre-test/post-test prospective design and one was a single-arm post-test retrospective design. The outcomes measured and reported in the studies include severity of CIPN symptoms and neuropathic pain, impact on quality of life (QoL) and physical function, patient activation and intervention-specific outcomes. Three studies used validated patient-reported outcome measures (PROMs) for measuring CIPN outcomes such as the CIPN Assessment Tool [52] and QLQ-CIPN20 [13, 53]. One study used a physician-graded CIPN scoring scale [51], while another study used both a validated PROM for CIPN and an unvalidated PROM for interference of CIPN on daily activities scoring scale [54]. A validated Patient Activation Measure was used in one study to appraise the patient’s ability to actively manage their own health and symptoms [11].
Exercise studiesStudies involving exercise interventions were conducted in USA (n=4), Germany (n=4), Canada (n=2), Turkey (n=1), Australia (n=1) and India (n=1). Four EI studies used a single-arm pre-test/post-test prospective design, with study sample sizes ranging from three to twenty-nine. Out of eight RCTs, one was a sub-analysis of a primary RCT [59]. Control and intervention groups in all RCTs were similar in size but small in numbers (range: 11–19 participants per arm), except for one study with 170 in the intervention group and 185 in the control group [59]. One study adapted a quasi-experimental design whereby two groups received the intervention but at different stages of their chemotherapy treatment [66]. The main author in one study provided additional information about intervention delivery following email contact [57]. Outcomes measured were severity of CIPN symptoms and neuropathic pain, impact on quality of life (QoL) and physical function and intervention-specific outcomes. One study used a physician grading score, i.e. Total Neuropathy Score to measure CIPN symptoms [57] and one study used peripheral deep sensitivity testing only [56]. Five studies utilised validated tools such as the Leeds Assessment of Neuropathic Symptoms and Signs questionnaire [55], CIPN symptoms numeric rating scale [59], QLQ-CIPN20 [60], FACT-GOG NTx [61] and Pain DETECT questionnaire [66]. A combination of PROMs and physician grading score was used in one study [50]. The majority of the more recent studies used a combination of validated PROMs and Quantitative Sensory Testing [58, 62,63,64,65].
Intervention synthesis: behavioural interventionsFigure 2 presents the characteristics of behavioural and exercise interventions identified in this review. The six BI studies included in the review generated seven behavioural interventions, two of which were compared in one study [51].
Fig. 2
Representation of characteristics of behavioural and exercise interventions for chemotherapy-induced peripheral neuropathy
Scope and mechanisms of actionMost interventions did not solely focus on CIPN management but also included management of other chemotherapy side effects. Interventions included self-reporting of CIPN symptoms and neuropathic pain which were assessed alongside other cancer and treatment side effects [13, 51, 53, 54]. All interventions contained educational components about CIPN and management. Some interventions referred participants to established sites with information about CIPN and its management through local links and national cancer organisations [51, 53, 54]. Key topics found across interventions included general information about CIPN, safety and physical function, how to report symptoms, pharmacological and non-pharmacological interventions and referral to therapists.
Explicit details that explained mechanisms of action and how they caused a change of behaviour or achieved outcomes were lacking. Based on descriptions provided in the studies, we identified the possible mechanisms of action of the interventions listed below:
provides regular patient reminders to monitor and report their symptoms [13, 51]
encourages discussing symptom management with their nurse about managing their symptoms [51]
assists patients to acquire information, if needed [51]
gives automated advice for symptom management [51]
increases patient’s knowledge about CIPN, safety and management [11, 13, 52, 54]
assists patients to be able to self-manage symptoms [11, 52, 53]
encourages patient-provider decision-making [11]
increases patient activation to manage own symptoms [11]
provides access to symptom management strategies to use at their own pace [13, 53]
allows patients to report their symptoms [54]
provides coaching on safety-related self-care [54]
alerts nurse practitioner to poorly controlled symptoms [54]
provides instructions to enable patients to communicate CIPN symptoms to clinicians [54]
Underpinning conceptual modelsNo study explicitly applied a conceptual model for intervention development. Some of the included studies used behavioural or psychological concepts to describe the rationale or goal of the elements essential to the interventions. These include creativity, optimism, planning and expert [52], shared decision-making [11], patient activation [11, 13], cognitive-behavioural pain management [53] and self-care [13, 54]. The level of reporting was insufficient to enable identification of conceptual models and theoretical bases of interventions. The application of BCT Taxonomy v.1 [36] identified a total of 12 behaviour change techniques (BCTs) used in the intervention arms as illustrated in Fig. 3. The BCTs identified as present in all interventions were action planning, instruction on how to perform a behaviour and habit formation. Giving prompts and cues were used in all but one intervention [52].
Fig. 3
Summary of current evidence—behavioural and exercise interventions for chemotherapy-induced peripheral neuropathy
Conceptual constructs from studies and mechanisms of action, based on our interpretation, are presented in Fig. 3.
Components and context Components (activities)In two interventions, no further follow-up was provided after the initial activity which involved completing a 50-min programme of four informational modules [52] and a cross-sectional pain symptom assessment that generated recommended educational modules for participants to use as they wish [54]. Five interventions assessed self-reported severity of CIPN symptoms during chemotherapy treatment [11, 13, 51, 53, 54]. Self-reported severity assessments were conducted once [53], daily [11, 54], weekly [51] or during each clinic visit [13]. Of these five studies, two provided telephone coaching on CIPN management when CIPN symptoms were severe [51, 54]. When symptoms were poorly controlled, the system alerted the nurse practitioner to make telephone contact with the participant to provide follow-up care [54]. In one intervention, when a patient reported CIPN above the severity threshold, a nurse provided CIPN management coaching [51]. On the other hand, one intervention generated a care plan based on CIPN severity which the clinician could edit or tailor before sending to the patient by [11]. In one intervention, moderate to severe CIPN symptom grading prompted participants to read self-care messages on the website [13]. Interventions which recommended management strategies based on severity of symptoms were facilitated through guidelines provided to nurses and patients [
留言 (0)